
Subscribe
eNewsletter
Ready to get certified?
Free CDCES Coach App
eNewsletter
Free CDCES Coach App

For last week’s practice question, we quizzed participants on living with diabetes & traveling to different timezones. 65% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question: BT is heading to the south of France for a 25th wedding anniversary vacation. They usually take 32 units of glargine at 10 PM each night along with 5-7 units of bolus insulin with meals. There is a nine hour time difference between the United States and France.
They ask you how to adjust their basal insulin. What is the best response?
Answer Choices:
If you are thinking about taking the certification exam, this practice test question will set you up for success. Test writers anticipate possible answers based on the details in the question. They will wave those “juicy answers” right under your nose. Your job is to weed through the particulars, pluck out the most important elements and choose the BEST answer.
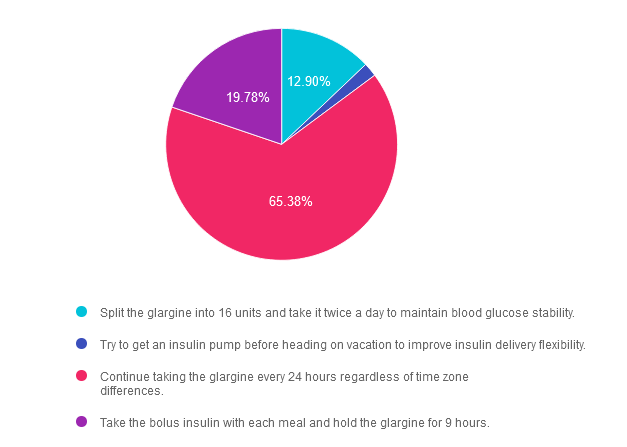
Answer 1 is incorrect. 12.90% chose this answer. “Split the glargine into 16 units and take it twice a day to maintain blood glucose stability.” Although a tempting answer, this action does not address or solve the issue of determining insulin injection timing in a different time zone.
Answer 2 is incorrect. 1.94% of you chose this answer. “Try to get an insulin pump before heading on vacation to improve insulin delivery flexibility.” This approach offers too big of an intervention based on BT’s question of when to dose their insulin in a different time zone.
Answer 3 is correct. About 65.38% of respondents chose this. “Continue taking the glargine every 24 hours regardless of time zone differences.” YES, GREAT JOB. Sometimes the most direct and simplest answer is the best answer. While traveling across time zones, as long as BT takes the basal insulin about every 24 hours and the bolus insulin with meals, they will be able to maintain their usual approach. However, accurate carb counting for French pastries and three course meals is a whole different challenge. : -)
Finally, Answer 4 is incorrect. 19.78% chose this answer. “Take the bolus insulin with each meal and hold the glargine for 9 hours.” The first part of this answer is correct, but the second part isn’t really accurate and it is too vague and confusing to make this answer the best choice. This is a great example of a “juicy answer”.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
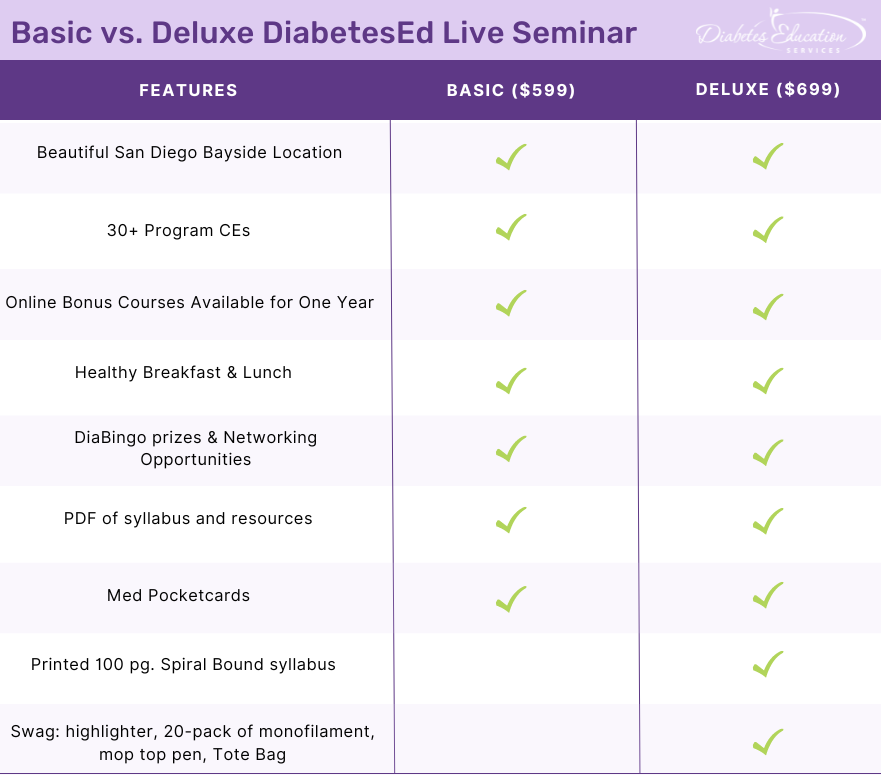
Join Coach Beverly and Team for two and a half days of knowledge-sharing, fun, networking, games with prizes, and “aha” moments in beautiful San Diego.
You don’t want to miss this one-of-a-kind learning opportunity. Get away from all those daily responsibilities and immerse yourself in a fun and intensive conference with plenty of networking opportunities.
Attendees will leave this conference with new tools and a more complete understanding of the latest advances in diabetes care, from medications to technology to Medical Nutrition Therapy!
Bring your colleagues and enjoy our friend discount.
Our team expertly translates the complex science of diabetes into understandable terms while keeping it real, practical, and fun.
Team of expert faculty includes:
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the diabetes certification exams. CBDCE & ADCES does not endorse any preparatory or review materials for the certification exams, except for those published by CBDCE & ADCES.
For last week’s practice question, we quizzed participants on actions for managing stage 2, type 1 diabetes. 63% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question: LT has just been diagnosed with stage 2, type 1 diabetes. They have 2 positive antibodies and their blood sugars are slightly elevated. They ask you if they are a candidate for “that therapy” that can protect their beta cells and slow progression of type 1 diabetes.
What is the most accurate response?
Answer Choices:
If you are thinking about taking the certification exam, this practice test question will set you up for success. Test writers anticipate possible answers based on the details in the question. They will wave those “juicy answers” right under your nose. Your job is to weed through the particulars, pluck out the most important elements and choose the BEST answer.
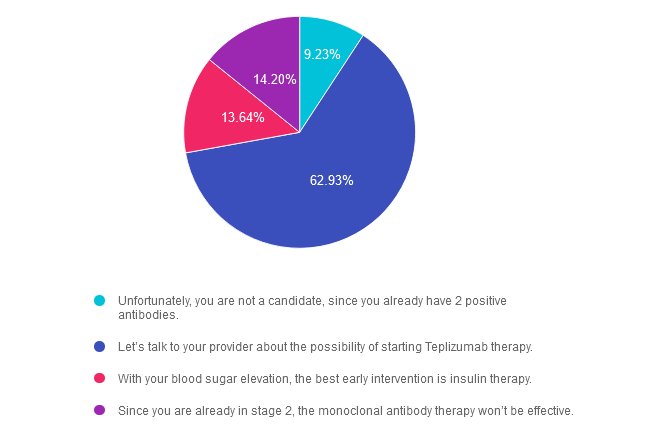
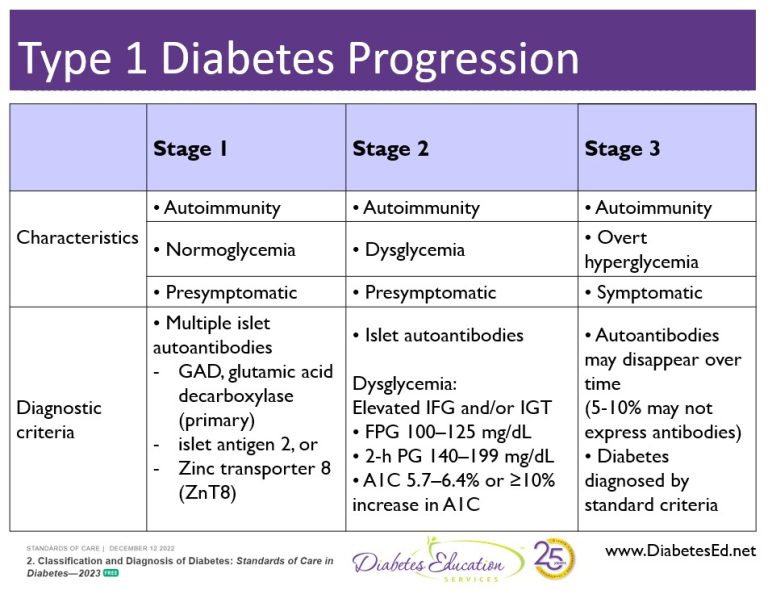
Answer 1 is incorrect. 9.23% chose this answer. “Unfortunately, you are not a candidate, since you already have 2 positive antibodies.” Teplizumab IS indicated for the individual in stage 2 type 1 diabetes, or for those with two or more islet autoantibodies and abnormal glycemia but still asymptomatic. People with stage 2 type 1 diabetes, have a nearly 100% lifetime risk of progression to clinical (stage 3) type 1 diabetes and a 75% risk of developing the condition within 5 years.
Answer 2 is correct. 62.93% of you chose this answer. “Let’s talk to your provider about the possibility of starting Teplizumab therapy.” YES, this is the BEST ANSWER, According to ADA Standards, Teplizumab is the first disease-modifying therapy that impedes the progression of type 1 diabetes by binding to the surface of T cells to dampen the unwanted immune system response. It can delay the onset of symptomatic stage 3 type 1 diabetes in adults and children 8 years and older with stage 2 type 1 diabetes (see staging chart). It is administered by intravenous infusion once daily for 14 consecutive days and is expected to cost in the region of $200,000 for the course of treatment. Based on current data, it can delay the expression of stage 3 diabetes by 2 years or longer.
Answer 3 is incorrect. About 13.64% of respondents chose this. “With your blood sugar elevation, the best early intervention is insulin therapy.” Actually, according to ADA Guidelines, LT is a perfect candidate, since Teplizumab IS indicated for the individual in stage 2 type 1 diabetes, or for those with two or more islet autoantibodies and abnormal glycemia but still asymptomatic.
Finally, Answer 4 is incorrect. 14.20% chose this answer. “Since you are already in stage 2, the monoclonal antibody therapy won’t be effective.” Actually, according to ADA Guidelines, LT is a perfect candidate, since Teplizumab IS indicated for the individual in stage 2 type 1 diabetes, or for those with two or more islet autoantibodies and abnormal glycemia but still asymptomatic.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
For more information, see our blog on Teplizumab Therapy to Delay Type 1 Diabetes.
Join Coach Beverly and Team for two and a half days of knowledge-sharing, fun, networking, games with prizes, and “aha” moments in beautiful San Diego.
You don’t want to miss this one-of-a-kind learning opportunity. Get away from all those daily responsibilities and immerse yourself in a fun and intensive conference with plenty of networking opportunities.
Attendees will leave this conference with new tools and a more complete understanding of the latest advances in diabetes care, from medications to technology to Medical Nutrition Therapy!
Bring your colleagues and enjoy our friend discount.
Our team expertly translates the complex science of diabetes into understandable terms while keeping it real, practical, and fun.
Team of expert faculty includes:
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the diabetes certification exams. CBDCE & ADCES does not endorse any preparatory or review materials for the certification exams, except for those published by CBDCE & ADCES.
For last week’s practice question, we quizzed participants on the effects of nocturnal hyperglycemia. 63% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question: JR is 11 years old with type 1 diabetes and their parent shares their concern that the blood glucose seems to be rising overnight with morning hyperglycemia. The parent is worried that JR may be sneaking snacks in the night.
As a diabetes specialist, you know that this glucose rise is most likely due to:
Answer Choices:
If you are thinking about taking the certification exam, this practice test question will set you up for success. Test writers anticipate possible answers based on the details in the question. They will wave those “juicy answers” right under your nose. Your job is to weed through the particulars, pluck out the most important elements and choose the BEST answer.
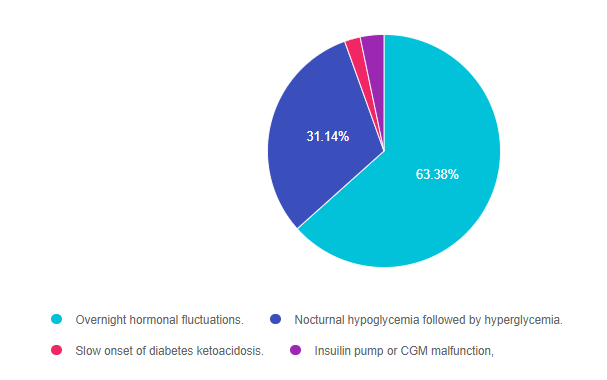
Answer 1 is correct. 63.38% chose this answer. “Overnight hormonal fluctuations.” YES, this is the best answer. There is an increased release of counterregulatory and growth hormones during the night, that is especially noteworthy during the teen years. These hormones contribute to insulin resistance and can cause morning hyperglycemia, often referred to as the Dawn Phenomena. For this reason, basal insulin dosing and rates need ongoing adjustment to address this nocturnal insulin resistance.
Answer 2 is incorrect. 31.14% of you chose this answer. “Nocturnal hypoglycemia followed by hyperglycemia.” Even though this phenomena, referred to as Somogyi effect, could cause morning hyperglycemia, there is no information in the test question that indicates JR is experiencing lows over night. Symptoms of hypoglycemia during the night might include; morning headaches, night sweats, vivid dreams or waking up hungry.
Answer 3 is incorrect. About 2.19% of respondents chose this. “Slow onset of diabetes ketoacidosis.” Even though hyperglycemia is associated ketoacidosis, JR has no symptoms of ketoacidosis like lethargy, fruity breath, urine ketones or dehydration.
Finally, Answer 4 is incorrect. 3.29% chose this answer. “Insulin pump or CGM malfunction.” While pump malfunction can lead to hyperglycemia, there is no information contained in the test question that would lead us to believe that JR is using any diabetes technology.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Join Coach Beverly and Team for two and a half days of knowledge-sharing, fun, networking, games with prizes, and “aha” moments in beautiful San Diego.
You don’t want to miss this one-of-a-kind learning opportunity. Get away from all those daily responsibilities and immerse yourself in a fun and intensive conference with plenty of networking opportunities.
Attendees will leave this conference with new tools and a more complete understanding of the latest advances in diabetes care, from medications to technology to Medical Nutrition Therapy!
Bring your colleagues and enjoy our friend discount.
Our team expertly translates the complex science of diabetes into understandable terms while keeping it real, practical, and fun.
Team of expert faculty includes:
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
For last week’s practice question, we review strategies for keeping glucose “under control.” 79% of respondents chose the best answer which is awesome. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question: JR is 13 years old and has type 1 diabetes and their time in range is usually less than 50%. JR’s mom finds empty soda bottles hidden in the back of JR’s drawer along with some candy bars.
JR’s mom is very upset about this discovery and asks you how to get this “situation under control”. What is the most appropriate response?
Answer Choices:
If you are thinking about taking the certification exam, this practice test question will set you up for success. Test writers anticipate possible answers based on the details in the question. They will wave those “juicy answers” right under your nose. Your job is to weed through the particulars, pluck out the most important elements and choose the BEST answer.
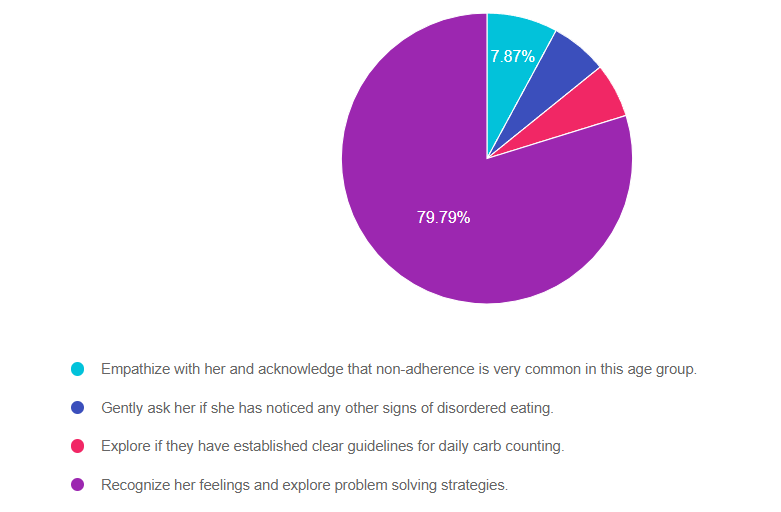
Answer 1 is incorrect. 7.87% chose this answer. “Empathize with her and acknowledge that non-adherence is very common in this age group.” Although this answer starts out with empathy, the second half reinforces the outdated concept of “non-adherence”. If JR is eating candy bars and drinking sodas, then hiding the evidence, indicates that JR might be experiencing big emotions around food restrictions that need exploration.
Answer 2 is incorrect. 6.30% of you chose this answer. “Gently ask her if she has noticed any other signs of disordered eating.” We can’t assume that JR has disordered eating because they are eating candy bars and drinking sodas, then hiding the evidence. This behavior may indicate that JR is experiencing big emotions around food restrictions that need exploration.
Answer 3 is incorrect. About 6.04% of respondents chose this. “Explore if they have established clear guidelines for daily carb counting.” Even though JR is eating candy bars and drinking sodas, then hiding the evidence, it doesn’t indicate that they additional information on carb counting or are in need of stricter guidelines.
Finally, Answer 4 is correct. 79.79% chose this answer. “Recognize her feelings and explore problem-solving strategies.” YES, GREAT JOB. This is the best answer. If JR is eating candy bars and drinking sodas, then hiding the evidence, this indicates that JR might be experiencing big emotions around food restrictions that need exploration.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Join Coach Beverly and Team for two and a half days of knowledge-sharing, fun, networking, games with prizes, and “aha” moments in beautiful San Diego.
You don’t want to miss this one-of-a-kind learning opportunity. Get away from all those daily responsibilities and immerse yourself in a fun and intensive conference with plenty of networking opportunities.
Attendees will leave this conference with new tools and a more complete understanding of the latest advances in diabetes care, from medications to technology to Medical Nutrition Therapy!
Bring your colleagues and enjoy our friend discount.
Our team expertly translates the complex science of diabetes into understandable terms while keeping it real, practical, and fun.
Team of expert faculty includes:
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
For last week’s practice question, we review how to help improve time in range. 79% of respondents chose the best answer which is awesome. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question: TR is 25 and has new type 1 diabetes and is hoping to get on an insulin pump soon. TR weighs 70 kgs and takes 8 units basal insulin at bedtime, plus takes 1 unit bolus insulin for every 15 gms of carbohydrate and their correction for hyperglycemia is 1 unit for every 50 points above 120. When looking at TR’s ambulatory glucose profile, their time in range is 32% with 67% above range and about ~1% below range. Glucose levels tend to increase starting with dinner at 5pm and stay elevated throughout the night.
Based on this information, what change(s) could help improve time in range?
Answer Choices:
If you are thinking about taking the certification exam, this practice test question will set you up for success. Test writers anticipate possible answers based on the details in the question. They will wave those “juicy answers” right under your nose. Your job is to weed through the particulars, pluck out the most important elements and choose the BEST answer.
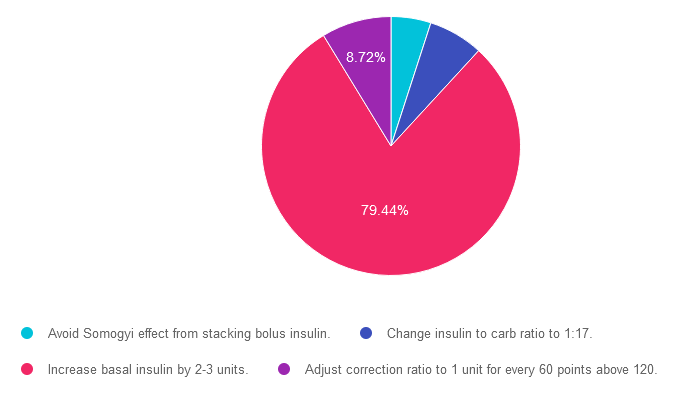
Answer 1 is incorrect. 4.98% chose this answer. “Avoid Somogyi effect from stacking bolus insulin.” Somogyi is when blood sugars drop and the counter-regulatory system releases hormones that can dramatically increase blood sugar levels (sometimes referred to as rebound hyperglycemia). Since TR’s glucose levels tend to increase starting with dinner at 5pm and stay elevated throughout the night, they are not experiencing the hypoglycemia associated with the Somogyi effect.
Answer 2 is incorrect. 6.85% of you chose this answer. “Change insulin to carb ratio to 1:17.” Since TR’s glucose levels tend to increase starting with dinner at 5pm and stay elevated throughout the night, this is not due to post meal hyperglycemia. Overnight hyperglycemia is usually connected to inadequate basal insulin dosing.
Answer 3 is correct. About 79.44% of respondents chose this. “Increase basal insulin by 2-3 units.” YES, GREAT JOB! Since TR’s glucose levels tend to increase starting with dinner at 5pm and stay elevated throughout the night, this is an indication that TR has inadequate basal insulin dosing.
Finally, Answer 4 is incorrect. 8.72% chose this answer. “Adjust correction ratio to 1 unit for every 60 points above 120.” Since TR’s glucose levels tend to increase starting with dinner at 5pm and stay elevated throughout the night, this is not due to post meal hyperglycemia or inadequate bolus insulin correction coverage. Overnight hyperglycemia is usually connected to inadequate basal insulin dosing.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
As diabetes technology is becoming commonplace in our practice, figuring out how to make sense of all the data can seem overwhelming. Dr. Isaacs has a special knack for breaking down the essential elements of the Ambulatory Glucose Profile (AGP) and other reports to provide participants with a clear road map for data interpretation. She includes tons of sample practice cases utilizing CGM, connected pens, and insulin pumps.
By attending this interactive workshop, participants will become more confident in interpreting the AGP and continuous glucose monitor (CGM) data and determining needed medication and lifestyle adjustments.
Topics include:
Instructor: Diana Isaacs, PharmD, BCPS, BCACP, CDCES, BC-ADM, FADCES, FCCPCES, was awarded ADCES Diabetes Care and Educational Specialist of the Year for her educational platform promoting the use of CGM for people with diabetes and other innovations. She is the Director of Education & Training in Diabetes Technology at the Cleveland Clinic. She has numerous diabetes publications and research projects focusing on medications, CGM, and diabetes technology. You won’t want to miss this hands-on workshop with an international expert in the field.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
For last week’s practice question, we quizzed participants on Hypoglycemia before meals. 37% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question: JR has type 1 diabetes and is worried how to best adjust insulin to address hypoglycemia and prevent future episodes. They tell you that their blood sugar yesterday before lunch was 67 mg/dL and they were getting ready to eat 45 gms of carb and cover with 3 units of insulin.
JR asks, what is the best strategy in this situation? What action do you advise JR to take?
Answer Choices:
If you are thinking about taking the certification exam, this practice test question will set you up for success. Test writers anticipate possible answers based on the details in the question. They will wave those “juicy answers” right under your nose. Your job is to weed through the particulars, pluck out the most important elements and choose the BEST answer.
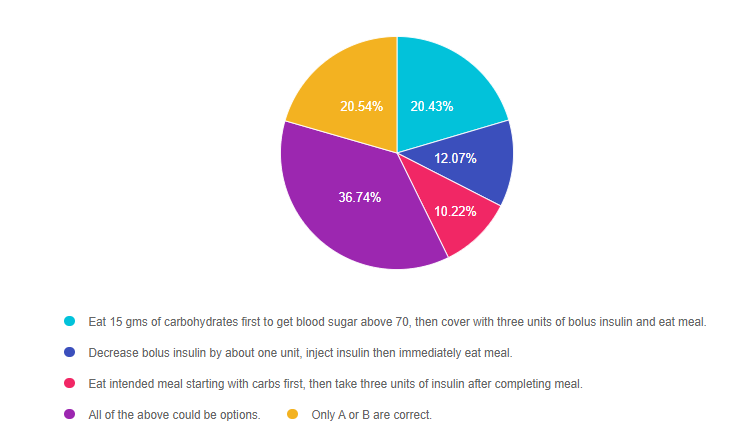
Answer 1 is incorrect. 20.43% chose this answer. “Eat 15 gms of carbohydrates first to get blood sugar above 70, then cover with three units of bolus insulin and eat meal.” This standard intervention, often referred to as the “rule of 15”, is a safe approach that is certainly a correct option.
Answer 2 is incorrect. 12.07% of you chose this answer. “Decrease bolus insulin by about one unit, inject insulin then immediately eat meal.” This standard intervention is also a safe approach that is certainly a correct option.
Answer 3 is incorrect. About 10.22% of respondents chose this. “Eat intended meal starting with carbs first, then take three units of insulin after completing meal.” This creative intervention is certainly a viable option that JR could choose.
Answer 4 is correct. 36.74% chose this answer. “All of the above could be options.” YES, this is the BEST answer. People with type 1 diabetes can use a variety of approaches to address and treat hypoglycemia. As diabetes care and education coaches, we take a person-centered approach, leaning into the individual’s expertise. If an approach is safe and fits into JR’s lifestyle and comfort zone, we are going to support their decision. We also keep the door open to reviewing the impact of the approach and engaging in collaborative problem solving as needed.
Finally, Answer 5 is incorrect 20.54% of you chose this answer. “Only A or B are correct.” Not quite the best answer since people with type 1 diabetes can use a variety of approaches to address and treat hypoglycemia. As diabetes care and education coaches, we take a person-centered approach, leaning into the individual’s expertise. If an approach is safe and fits into JR’s lifestyle and comfort zone, we are going to support their decision. We also keep the door open to reviewing the impact of the approach and engaging in collaborative problem solving as needed. That is why the answer choice “C” could also be correct. JR might be most comfortable with taking the insulin after the meal to avoid another hypoglycemic event.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Join Coach Beverly and Team for two and a half days of knowledge-sharing, fun, networking, games with prizes, and “aha” moments in beautiful San Diego.
You don’t want to miss this one-of-a-kind learning opportunity. Get away from all those daily responsibilities and immerse yourself in a fun and intensive conference with plenty of networking opportunities.
Attendees will leave this conference with new tools and a more complete understanding of the latest advances in diabetes care, from medications to technology to Medical Nutrition Therapy!
Bring your colleagues and enjoy our friend discount.
Our team expertly translates the complex science of diabetes into understandable terms while keeping it real, practical, and fun.
Team of expert faculty includes:
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
For last week’s practice question, we quizzed participants on Hypoglycemia during exercise. 79% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question: JR has type 1 and tells you they limit their carbohydrate intake to 30 gms a day to prevent hyperglycemia. Their A1C is 6.7% and time in range is over 70%. They tell you their main goal is to figure out how to prevent hypoglycemia during exercise.
What would be the best response using a person-centered approach?
Answer Choices:
If you are thinking about taking the certification exam, this practice test question will set you up for success. Test writers anticipate possible answers based on the details in the question. They will wave those “juicy answers” right under your nose. Your job is to weed through the particulars, pluck out the most important elements and choose the BEST answer.
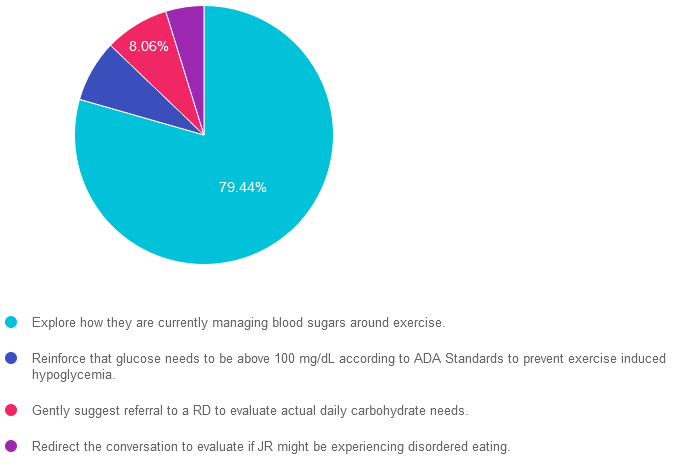
Answer 1 is correct]. 79.44% chose this answer. “Explore how they are currently managing blood sugars around exercise.” YES, GREAT JOB! Since this response is person centered and respectful of JR’s desire to learn how to prevent hypoglycemia, it is the best answer. Sometimes, we might be tempted to focus on a different goal than what the individual is requesting. However, by addressing their priorities FIRST, we build trust and create meaningful connections.
Answer 2 is incorrect. 7.73% of you chose this answer. “Reinforce that glucose needs to be above 100 mg/dL according to ADA Standards to prevent exercise induced hypoglycemia.” This answer doesn’t allow for exploration, personalization and customization. A glucose goal of “above 100” pre-exercise does not fit for everyone. People with type 1 diabetes often feel more comfortable with a blood sugar 180 mg/dL or greater before engaging in activity to prevent hypoglycemia from glucose expenditure during exercise.
Answer 3 is incorrect. About 8.06% of respondents chose this. “Gently suggest referral to a RD to evaluate actual daily carbohydrate needs.” Although, JR is limiting his intake to 30gms carb a day, they have stated that they want to work on preventing exercise related hypoglycemia. Sometimes, we might be tempted to focus on a different goal than what the individual is requesting. However, by addressing their priorities FIRST, we build trust and create meaningful connections.
Finally, Answer 4 is incorrect. 4.77% chose this answer. “Redirect the conversation to evaluate if JR might be experiencing disordered eating.” Although, JR is limiting his intake to 30gms carb a day, they have stated that they want to work on preventing exercise related hypoglycemia. Sometimes, we might be tempted to focus on a different goal than what the individual is requesting. However, by addressing their priorities FIRST, we build trust and create opportunities to explore other topics in the future.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
“ReVive 5 Program is the best program I have ever attended – should be required for all diabetes educators! Thank you so much for translating this research into practical approaches!!” – Sarah F.

Addressing diabetes distress can be tricky, even for seasoned healthcare professionals.
We invite you to attend this hands-on training program that provides the essential steps to address diabetes distress combined with an innovative approach to glucose management. Our experts offer realistic strategies to address diabetes distress that you can immediately apply to your practice setting. Plus, the ReVive 5 Program provides a breadth of tools and resources to create more meaningful connections with people with diabetes.
Team of Experts: ReVive 5 is taught by a team of 3 Interdisciplinary Experts:
Accredited Training Program:
“ReVive 5” breathes new life into our relationship with diabetes, bringing a fresh perspective to both the person with diabetes and the provider.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
For last week’s practice question, we quizzed participants on post-meal hypoglycemia. 69% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question:
JR has lived with type 1 diabetes for over 30 years and has been complaining that they feel full and bloated after eating and experiencing more post-meal hypoglycemia.
Based on this information, what is the most appropriate recommendation for JR?
Answer Choices:
If you are thinking about taking the certification exam, this practice test question will set you up for success. Test writers anticipate possible answers based on the details in the question. They will wave those “juicy answers” right under your nose. Your job is to weed through the particulars, pluck out the most important elements and choose the BEST answer.
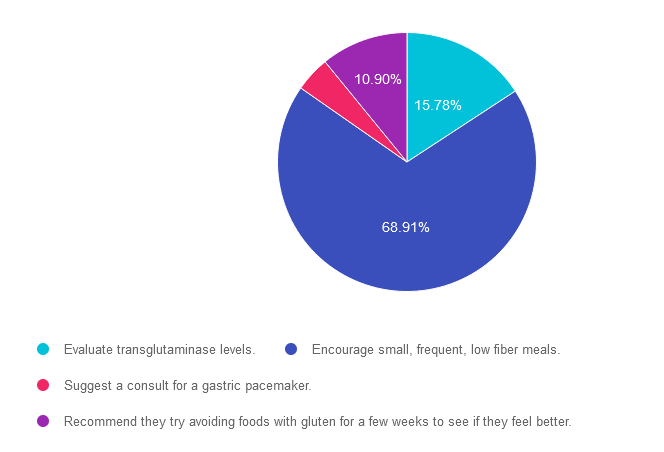
Answer 1 is incorrect. 15.78% chose this answer. “Evaluate transglutaminase levels.” Based on JR’s symptoms of “feeling full and bloated after eating and experiencing more post-meal hypoglycemia” we are not suspecting celiac disease since there is no mention of bloating after gluten rich foods. Plus, post meal hypoglycemia is more likely associated with the delayed gastric emptying associated with gastroparesis. Since transglutaminase is a test used to detect celiac disease, this is not the best answer.
Answer 2 is correct. 68.91% of you chose this answer. “Encourage small, frequent, low fiber meals.” YES. GREAT JOB! JR’s symptoms of “feeling full and bloated after eating and experiencing more post-meal hypoglycemia” are both classic symptoms of gastroparesis and delayed gastric emptying. This autonomic neuropathic condition is treated with glucose improvement and smaller, low fiber meals to support gastric movement. In addition, a referral to a GI specialist is certainly warranted.
Answer 3 is incorrect. About 4.41% of respondents chose this. “Suggest a consult for a gastric pacemaker.” JR’s symptoms of “feeling full and bloated after eating and experiencing more post-meal hypoglycemia” are both classic symptoms of gastroparesis and delayed gastric emptying. This autonomic neuropathic condition is treated with glucose improvement and smaller, low fiber meals to support gastric movement. However, before suggesting a consult for a gastric pacemaker, JR would first need a referral to a GI specialist to confirm diagnosis and evaluate best next steps.
Finally, Answer 4 is incorrect. 10.90% chose this answer. “Recommend they try avoiding foods with gluten for a few weeks to see if they feel better.” Based on JR’s symptoms of “feeling full and bloated after eating and experiencing more post-meal hypoglycemia” we are not suspecting celiac disease since there is no mention of bloating after gluten rich foods. Plus, post meal hypoglycemia is more likely associated with the delayed gastric emptying associated with gastroparesis.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Join Coach Beverly and Team for two and a half days of knowledge-sharing, fun, networking, games with prizes, and “aha” moments in beautiful San Diego.
You don’t want to miss this one-of-a-kind learning opportunity. Get away from all those daily responsibilities and immerse yourself in a fun and intensive conference with plenty of networking opportunities.
Attendees will leave this conference with new tools and a more complete understanding of the latest advances in diabetes care, from medications to technology to Medical Nutrition Therapy!
Bring your colleagues and enjoy our friend discount.
Our team expertly translates the complex science of diabetes into understandable terms while keeping it real, practical, and fun.
Team of expert faculty includes:
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
{kind=link}