
Subscribe
eNewsletter
Ready to get certified?
Free CDCES Coach App
eNewsletter
Free CDCES Coach App

For last week’s practice question, we quizzed participants on getting A1C to goal. 65% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question: AR’s has an A1C of 7.5% and is taking empagliflozin (Jardiance) 10mg daily, plus trying to eat healthy and ride their bike 4-5 days a week for 30 minutes. The provider suggests increasing the empagliflozin dose to 25mg to get the A1C below 7%. AR says that they don’t want to increase their medication dose and says they are dedicated to lowering their A1C through more activity.
Based on this scenario, what ADA recommended activity addition or change would help AR reach their A1C target?
Answer Choices:
If you are thinking about taking the certification exam, this practice test question will set you up for success. Test writers anticipate possible answers based on the details in the question. They will wave those “juicy answers” right under your nose. Your job is to weed through the particulars, pluck out the most important elements and choose the BEST answer.
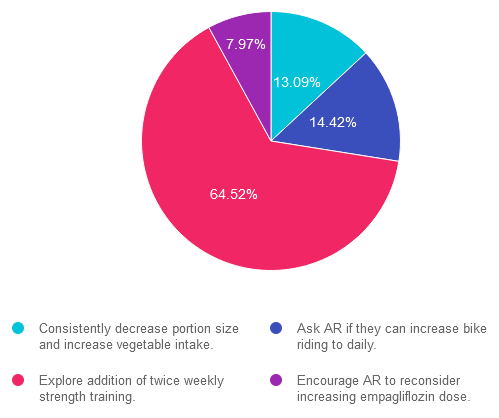
Answer 1 is incorrect. 13.09% chose this answer. “Consistently decrease portion size and increase vegetable intake.” This juicy answer is tempting, since it addresses portion size and includes more vegetable intake. However, it is not the best answer since it doesn’t match AR’s stated goal that “they are dedicated to lowering their A1C through more activity.”
Answer 2 is incorrect. 14.42% of you chose this answer. “Ask AR if they can increase bike riding to daily.” Based on the ADA Standards, individuals are encouraged to maintain 150 minutes of activity a week, plus strengthening activities twice weekly. Asking AR to increase bike to riding to daily, is not the best approach in this scenario to achieve A1C targets.
Answer 3 is correct. About 64.52% of respondents chose this. “Explore addition of twice weekly strength training.” YES, this is the best answer. Based on the ADA Standards, individuals are encouraged to maintain 150 minutes of activity a week, plus strengthening activities twice weekly. Studies show that increasing muscle mass significantly lowers glucose and A1C.
Finally, Answer 4 is incorrect. 7.97% chose this answer. “Encourage AR to reconsider increasing empagliflozin dose.” This juicy answer is tempting, since increasing the empagliflozin dose would most likely decrease AR’s blood sugar. However, it is not the best answer since it doesn’t match AR’s stated goal that “they are dedicated to lowering their A1C through more activity.”
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!.
For last week’s practice question, over 1,900 participants submitted their answers for how LR could improve glucose while preparing for pregnancy. 37% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question: LR is 29 years old, has newly discovered diabetes and polycystic ovary syndrome (PCOS) and is trying to get pregnant. In addition to treating the diabetes and PCOS, LR would like to lose weight. LR was referred to the RD/RDN and encouraged to increase activity level. To treat PCOS and diabetes, LR was started on metformin ER 500mg BID. After a month of treatment, LR’s A1C was still above 8%.
According to ADA Standards, besides increasing the metformin dose, what additional therapy could be added to get LR’s glucose to goal?
Answer Choices:
If you are thinking about taking the certification exam, this practice test question will set you up for success. Test writers anticipate possible answers based on the details in the question. They will wave those “juicy answers” right under your nose. Your job is to weed through the particulars, pluck out the most important elements and choose the BEST answer.
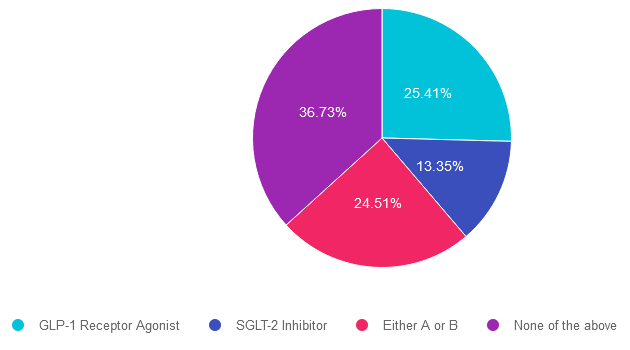
Answer 1 is incorrect. 25.41% chose this answer. “GLP-1 Receptor Agonist.” Given that LR has elevated blood glucose and wants to lose weight, starting a GLP-1 seems like a reasonable idea. However, GLP-1’s are not FDA approved for use during pregnancy. Since LR is trying to get pregnant, this class of medication would not be recommended.
Answer 2 is incorrect. 13.35% of you chose this answer. “SGLT-2 Inhibitor.” Given that LR has elevated blood glucose and wants to lose weight, starting a SGLT-2i seems like a reasonable idea. However, SGLT-2i’s are not FDA approved for use during pregnancy. Since LR is trying to get pregnant, this class of medication would not be recommended.
Answer 3 is incorrect. About 24.51% of respondents chose this. “Either A or B.” Given that LR has elevated blood glucose and wants to lose weight, starting either a SGLT-2i or a GLP-1 seems like a reasonable idea. However, SGLT-2i’s and GLP-1’s are not FDA approved for use during pregnancy. Since LR is trying to get pregnant, neither class of medication would not be recommended.
Finally, Answer 4 is correct. 36.73% chose this answer. “None of the above.” YES, This is the Best Answer. Metformin is the only non-insulin diabetes medication the ADA recommends for the first trimester of pregnancy. Many people with PCOS are treated with metformin to decrease insulin resistance and ovulation can resume, resulting in pregnancy. The ADA recommends stopping metformin after the first trimester and starting insulin if blood glucose levels remain above target.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
“ReVive 5 Program is the best program I have ever attended – should be required for all diabetes educators! Thank you so much for translating this research into practical approaches!!” – Sarah F.

Addressing diabetes distress can be challenging, even for seasoned healthcare professionals.
We invite you to attend this hands-on training program that provides the essential steps to address diabetes distress combined with an innovative approach to glucose management.
Team of Experts: ReVive 5 is taught by a team of 3 Interdisciplinary Experts:
Lawrence Fisher, Ph.D., ABPP, Professor Emeritus, UCSF
Susan Guzman, PhD
Beverly Thomassian, RN, MPH, CDCES, BC-ADM
Accredited Training Program:
“ReVive 5” breathes new life into our relationship with diabetes, bringing a fresh perspective to both the person with diabetes and the provider.
This bundle is specifically designed for healthcare professionals who are studying for the Certified Diabetes Care and Education Specialist (CDCES) exam.
The online bundle includes Level 1, Level 2, and Level 3 (Boot Camp), plus online Technology & Test-Taking Toolkits.
This bundle is specifically designed for healthcare professionals who are studying for the Board Certified in Advanced Diabetes Management (BC-ADM) exam.
This bundle includes our Level 2, Level 3 (Boot Camp), and Level 4, plus online Technology & Test-Taking Toolkits.
The next edition of the Review Guide will be released in August. We will be preselling as soon as we get the thumbs up.

This exclusive Everything Bundle provides access to ALL of our Online University Courses and Training Programs. This bundle is perfect for those who need CEs to renew their license or diabetes certification or are looking for a comprehensive update on all topics of diabetes.
Subscribers enjoy over 40 courses taught by Coach Beverly and her team of experts on topics ranging from Diabetes Distress to MNT, Technology to Pattern Management with a focus on providing evidence-based, person-centered diabetes care.
The first person who purchases our Everything Bundle wins our last copy of the Diabetes Review Guide 5th Ed.
All hours earned count toward your CDCES Accreditation Information
The ADCES (formerly AADE) Art and Science of Diabetes Care and Education, 5th Edition is a specialist’s one-volume, go-to resource for the core knowledge and skills for providing person-centered care and education to persons with diabetes and related chronic conditions. This is a core resource for those who are studying for the Certified Diabetes Care and Education Specialist (CDCES) exam.
ADCES will be releasing an updated edition of the Art & Science Desk reference in August 2023
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
For last week’s practice question, we quizzed participants on person-centered care. 55% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question: MR has an A1C of 9.6% and is deciding whether or not to start another diabetes medication to help lower their glucose. MR’s parent had diabetes and severe complications due to chronic hyperglycemia.
What would best describe the application of the Health Belief Model in this situation?
Answer Choices:
If you are thinking about taking the certification exam, this practice test question will set you up for success. Test writers anticipate possible answers based on the details in the question. They will wave those “juicy answers” right under your nose. Your job is to weed through the particulars, pluck out the most important elements and choose the BEST answer.
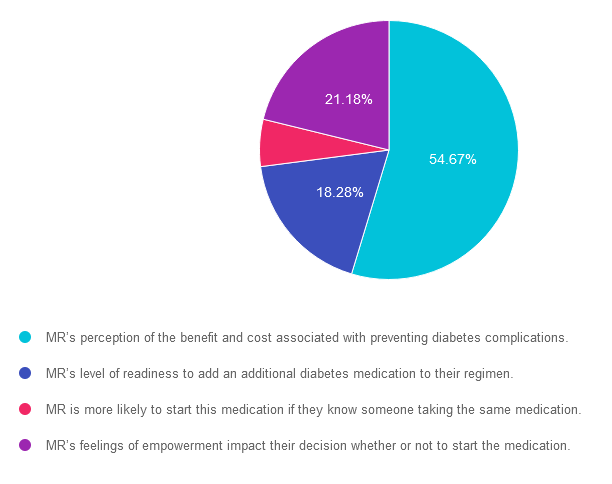
Answer 1 is correct. 54.67% chose this answer. “MR’s perception of the benefit and cost associated with preventing diabetes complications.” GREAT JOB. The Health Belief Model (HBM) focuses on individual beliefs and perceptions about health-related behavior change. It suggests that behavior change is influenced by an individual’s perception of the severity of a health problem, their susceptibility to it, the benefits of behavior change, and the barriers or cues to action. In other words it looks at the cost-benefit of a given situation.
Answer 2 is incorrect. 18.28% of you chose this answer. “MR’s level of readiness to add an additional diabetes medication to their regimen.” This answer actually refers the Stages of Change (transtheoretical) Model: This model proposes that individuals go through a series of stages when changing behavior: precontemplation, contemplation, preparation, action, and maintenance. It suggests that people move through these stages in a cyclical manner and that interventions should be tailored to each stage.
Answer 3 is incorrect. About 5.88% of respondents chose this. “MR is more likely to start this medication if they know someone taking the same medication.” This answer reflects the Social Cognitive Theory (SCT): This theory emphasizes the reciprocal interaction between personal factors (such as cognition and self-efficacy), environmental factors, and behavior. It suggests that behavior change is influenced by observing others (social modeling), self-regulation, and the belief that one can successfully perform the behavior (self-efficacy).
Finally, Answer 4 is incorrect. 21.18% chose this answer. “MR’s feelings of empowerment impact their decision whether or not to start the medication.” This answer refers to the empowerment model which is a theoretical framework that focuses on empowering individuals or communities to take control of their own lives and make informed decisions. It emphasizes the importance of promoting autonomy, self-efficacy, and participation in decision-making processes. The empowerment model is often applied in various fields, including social work, community development, healthcare, and education.

Learning behavior change theories and getting to the best answer for certification exams can be tricky. To say thanks for 25 years, Coach Beverly is going to host a FREE Webinar where she dissects common learning theories that are not only helpful for your clinical practice, but also for exam preparation.
Join her August 23rd at 11:30 am PT. For live webinars, Coach Beverly stays after class to answer any lingering questions you may have on the topic.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
“ReVive 5 Program is the best program I have ever attended – should be required for all diabetes educators! Thank you so much for translating this research into practical approaches!!” – Sarah F.
Addressing diabetes distress can be tricky, even for seasoned healthcare professionals.
We invite you to attend this hands-on training program that provides the essential steps to address diabetes distress combined with an innovative approach to glucose management. Our experts offer realistic strategies to address diabetes distress that you can immediately apply to your practice setting. Plus, the ReVive 5 Program provides a breadth of tools and resources to create more meaningful connections with people with diabetes.
Team of Experts: ReVive 5 is taught by a team of 3 Interdisciplinary Experts:
Accredited Training Program:
“ReVive 5” breathes new life into our relationship with diabetes, bringing a fresh perspective to both the person with diabetes and the provider.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the diabetes certification exams. CBDCE & ADCES does not endorse any preparatory or review materials for the certification exams, except for those published by CBDCE & ADCES.
For last week’s practice question, we quizzed participants on ADA recommendations for meal planning with diabetes. 41% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question: Which of the following diabetes meal planning recommendations is accurate according to ADA Standards of Care?
Answer Choices:
If you are thinking about taking the certification exam, this practice test question will set you up for success. Test writers anticipate possible answers based on the details in the question. They will wave those “juicy answers” right under your nose. Your job is to weed through the particulars, pluck out the most important elements and choose the BEST answer.
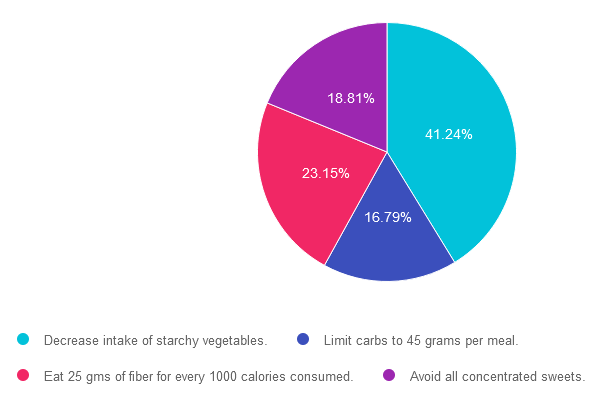
Answer 1 is correct. 41.24% chose this answer. “Decrease intake of starchy vegetables.” YES, this is the BEST answer. According to ADA Standard 5, “Reducing overall carbohydrate intake for individuals with diabetes has demonstrated evidence for improving glycemia and may be applied in a variety of eating patterns that meet individual needs and preferences. Eating plans should emphasize nonstarchy vegetables, fruits, legumes, and whole grains, as well as dairy products, with minimal added sugars. However, “macronutrient distribution should be based on an individualized assessment of current eating patterns, preferences, and metabolic goals.”
Answer 2 is incorrect. 16.79% of you chose this answer. “Limit carbs to 45 grams per meal.” This is a juicy answer, but is an older approach that is no longer recommended. According to ADA Standard 5, “Evidence suggests that there is not an ideal percentage of calories from carbohydrate, protein, and fat for people with diabetes. However, macronutrient distribution should be based on an individualized assessment of current eating patterns, preferences, and metabolic goals.”
Answer 3 is incorrect. About 23.15% of respondents chose this. “Eat 25 gms of fiber for every 1000 calories consumed.” WOW, that would be a LOT of fiber. This is a great number to know for certification exams. According to ADA Standard 5, “People with diabetes and those at risk for diabetes are encouraged to consume a minimum of 14 g of fiber/1,000 kcal, with at least half of grain consumption being whole, intact grains, according to the Dietary Guidelines for Americans.”
Finally, Answer 4 is incorrect. 18.81% chose this answer. “Avoid all concentrated sweets.” Even if you are not sure what the best answer is at first, this answer has two red flags, the word “avoid” and the word “all”. Since the ADA recommends flexibility and tailoring to the individual, this would not be the best person-centered answer. According to ADA Standard 5, “Dietary guidance should emphasize the importance of a healthy dietary pattern as a whole rather than focusing on individual nutrients, foods, or food groups, given that individuals rarely eat foods in isolation.”
We hope you appreciate this week’s rationale! For more info on ADA Standard 5, click here. Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
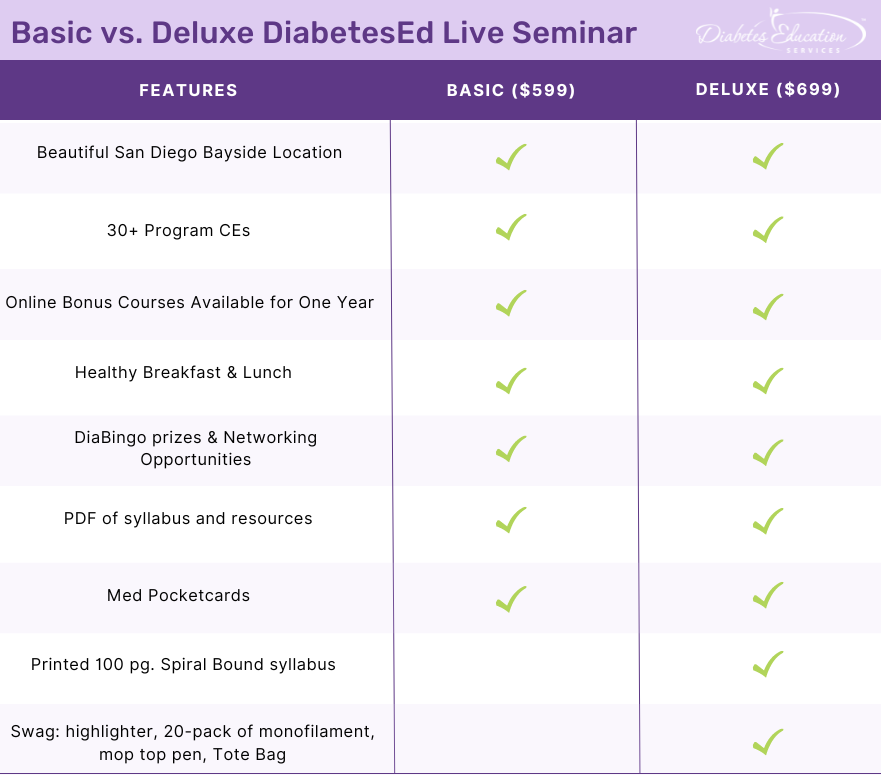
Join Coach Beverly and Team for two and a half days of knowledge-sharing, fun, networking, games with prizes, and “aha” moments in beautiful San Diego.
You don’t want to miss this one-of-a-kind learning opportunity. Get away from all those daily responsibilities and immerse yourself in a fun and intensive conference with plenty of networking opportunities.
Attendees will leave this conference with new tools and a more complete understanding of the latest advances in diabetes care, from medications to technology to Medical Nutrition Therapy!
Bring your colleagues and enjoy our friend discount.
Our team expertly translates the complex science of diabetes into understandable terms while keeping it real, practical, and fun.
Team of expert faculty includes:
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
For last week’s practice question, we quizzed participants on reimbursement for group DSME classes through Medicare. 48% of respondents chose the best answer. We want to clarify and share this important information, so you can prepare for certification exams and pass it on to your colleagues.
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question:
JR is 73 years old and has Medicare Part A and B insurance. JR completed a Diabetes Self-Management Program at a local hospital when they were in their late 60s and tells you they want to repeat the group sessions since they have forgotten much of the information.
What is the most accurate response?
Answer Choices:
If you are thinking about taking the certification exam, this practice test question will set you up for success since there are questions on Medicare Reimbursement. Test writers anticipate possible answers based on the details in the question. They will wave those “juicy answers” right under your nose. Your job is to weed through the particulars, pluck out the most important elements and choose the BEST answer.
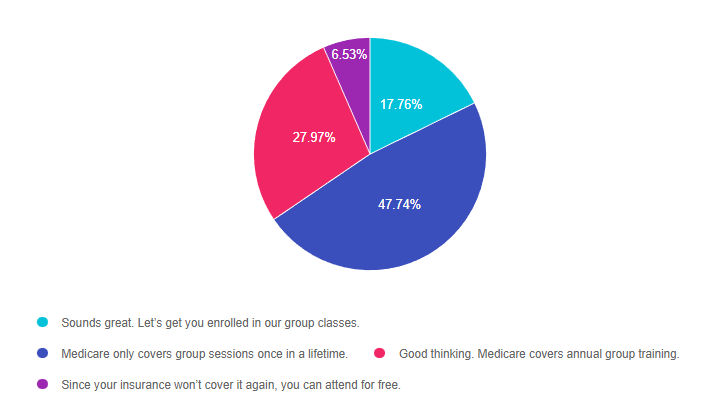
Answer 1 is incorrect. 17.76% chose this answer. “Sounds great. Let’s get you enrolled in our group classes.” A very welcoming answer, but unfortunately, it’s not accurate. According to Medicare Reimbursement Guidelines, Initial Diabetes Self Management Training (DSMT) is a “once-in-a-lifetime” Medicare benefit. Since JR completed a Diabetes Self-Management Program at a local hospital when they were in their late 60s, we assume that Medicare was billed for the service, since Medicare coverage starts at age 65. For this reason, it is important to verify that the beneficiary has not received any initial DSMT in the past prior to the delivery of the initial DSMT.
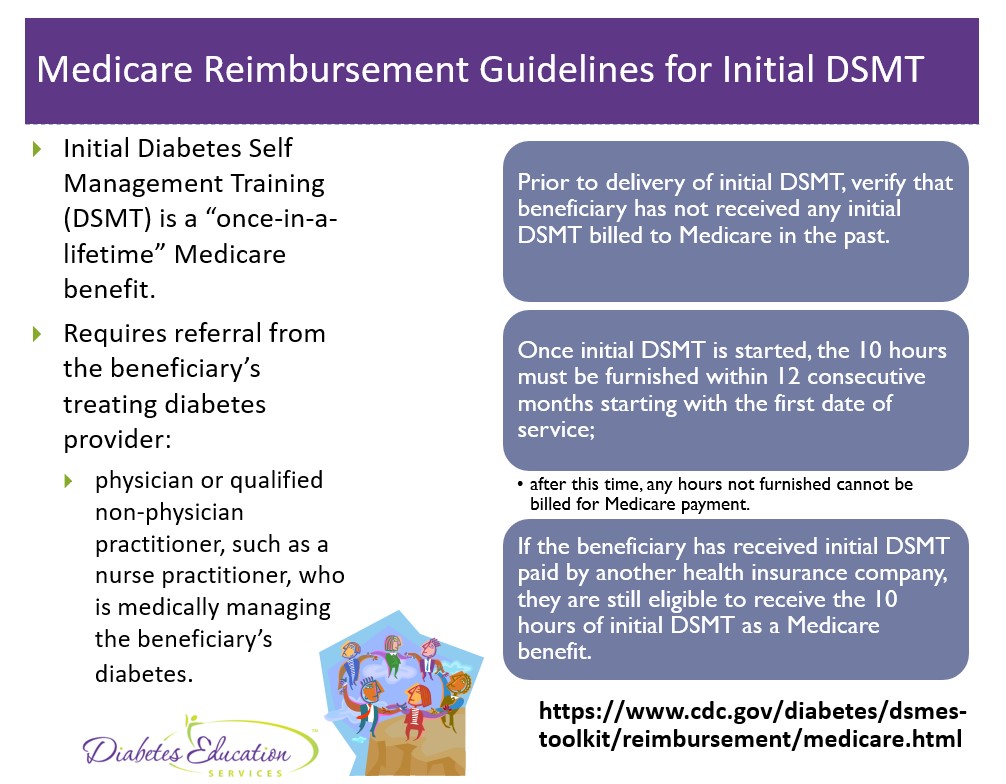
Answer 2 is correct. 47.74% of you chose this answer. “Medicare only covers group sessions once in a lifetime.” YES, this is the best answer. According to Medicare Reimbursement Guidelines, Initial Diabetes Self Management Training (DSMT) is a “once-in-a-lifetime” Medicare benefit. Since JR completed a Diabetes Self-Management Program at a local hospital when they were in their late 60s, we assume that Medicare was billed for the service, since Medicare coverage starts at age 65. For this reason, it is important to verify that the beneficiary has not received any initial DSMT in the past prior to the delivery of the initial DSMT.
However, if the beneficiary has received initial DSMT paid by another health insurance company, he/she is still eligible to receive the 10 hours of initial DSMT as a Medicare benefit.
Answer 3 is incorrect. About 27.97% of respondents chose this. “Good thinking. Medicare covers annual group training.” Another tempting answer, but not accurate. According to Medicare Reimbursement Guidelines, Initial Diabetes Self Management Training (DSMT) is a “once-in-a-lifetime” Medicare benefit. Since JR completed a Diabetes Self-Management Program at a local hospital when they were in their late 60s, we assume that Medicare was billed for the service, since Medicare coverage starts at age 65. For this reason, it is important to verify that the beneficiary has not received any initial DSMT in the past prior to the delivery of the initial DSMT.
Finally, Answer 4 is incorrect. 6.53% chose this answer. “Since your insurance won’t cover it again, you can attend for free.” This answer is kind hearted, but not correct. For Medicare, initial DSMT group classes can only be provided once in a lifetime and should be billed to Medicare and not offered for free. Programs can create a self-pay/uninsured policy where services are discounted (must be consistent in charges and discounts etc.).
Here is a summary slide on Medicare Reimbursement Guidelines.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity! You can read through the Medicare Reimbursement Guidelines here or the ADCES Info Sheet on DSMT Reimbursement join our Setting Up a Successful Diabetes Program & Medicare Reimbursement Webinar for more information.
Join Coach Beverly and Team for two and a half days of knowledge-sharing, fun, networking, games with prizes, and “aha” moments in beautiful San Diego.
You don’t want to miss this one-of-a-kind learning opportunity. Get away from all those daily responsibilities and immerse yourself in a fun and intensive conference with plenty of networking opportunities.
Attendees will leave this conference with new tools and a more complete understanding of the latest advances in diabetes care, from medications to technology to Medical Nutrition Therapy!
Bring your colleagues and enjoy our friend discount.
Our team expertly translates the complex science of diabetes into understandable terms while keeping it real, practical, and fun.
Team of expert faculty includes:
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the diabetes certification exams. CBDCE & ADCES does not endorse any preparatory or review materials for the certification exams, except for those published by CBDCE & ADCES.
For last week’s practice question, we quizzed participants on carrying insulin. 69% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question: JL has new type 1 diabetes and their time in range is about 40%. They tell you that carrying insulin pens around on ice is such a hassle that they don’t give insulin before eating out.
What is the best response?
Answer Choices:
If you are thinking about taking the certification exam, this practice test question will set you up for success. Test writers anticipate possible answers based on the details in the question. They will wave those “juicy answers” right under your nose. Your job is to weed through the particulars, pluck out the most important elements and choose the BEST answer.
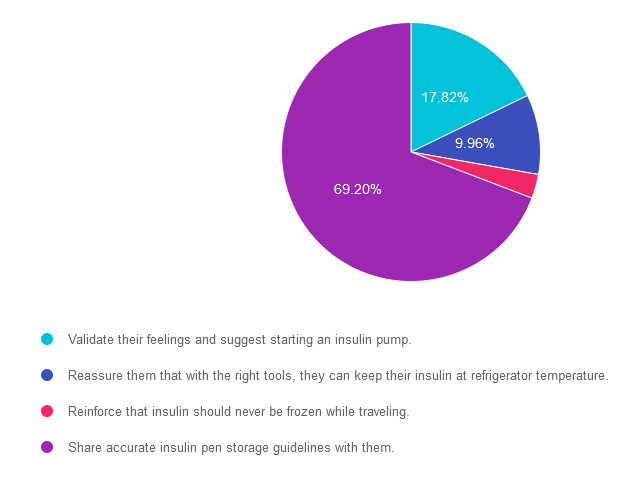
Answer 1 is incorrect. 17.82% chose this answer. “Validate their feelings and suggest starting an insulin pump.” Although this answer is tempting, it’s not the best answer. The first part of the answer that suggests validating their feelings is accurate. However, we would want to explore accurate insulin pen storage options before suggesting switching over to an insulin pump. Please see our insulin storage guidelines cheat sheet for more information.
Answer 2 is incorrect. 9.96% of you chose this answer. “Reassure them that with the right tools, they can keep their insulin at refrigerator temperature.” Once the person uses the insulin pen for the first time, it no longer needs to be refrigerated. Each type of insulin pen has storage guidelines for insulin kept at room temperature. Please see our insulin storage guidelines cheat sheet for more information.
Answer 3 is incorrect. About 3.01% of respondents chose this. “Reinforce that insulin should never be frozen.” It is true that insulin should never be frozen, but this is not the best answer. We also want to follow up with accurate and safe insulin pen storage information.
Finally, Answer 4 is correct. 69.20% chose this answer. “Share accurate insulin pen storage guidelines with them.” Yes, this is the best answer! Once insulin pens are used for the first time, they can be stored at room temperature. Of course, users have to avoid letting them overheat at temperatures of 86 degrees Fahrenheit or greater or getting too cold. Either situation can damage the insulin molecule. Please see our insulin storage cheat sheet for more information and feel free to share this info with colleagues and people with diabetes alike.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
“ReVive 5 Program is the best program I have ever attended – should be required for all diabetes educators! Thank you so much for translating this research into practical approaches!!” – Sarah F.
Addressing diabetes distress can be challenging, even for seasoned healthcare professionals.
We invite you to attend this hands-on training program that provides the essential steps to address diabetes distress combined with an innovative approach to glucose management.
Team of Experts: ReVive 5 is taught by a team of 3 Interdisciplinary Experts:
Lawrence Fisher, Ph.D., ABPP, Professor Emeritus, UCSF
Susan Guzman, PhD
Beverly Thomassian, RN, MPH, CDCES, BC-ADM
Accredited Training Program:
“ReVive 5” breathes new life into our relationship with diabetes, bringing a fresh perspective to both the person with diabetes and the provider.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
For last week’s practice question, we quizzed participants on in-patient diabetes care. 42% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
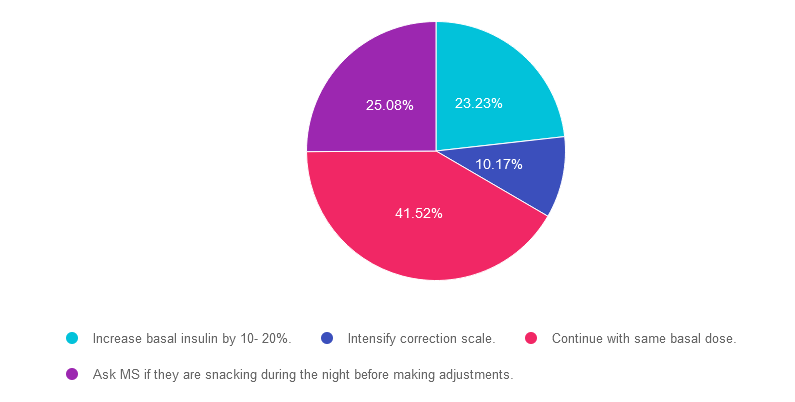
Question: JR was admitted to the hospital with an infection and newly discovered diabetes. To get glucose to ADA target range for hospitalized individuals, JR was started on 12 units of basal insulin plus bolus insulin with meals. JR experienced a morning BG of 87 mg/dL, so the provider decreased the basal insulin to 9 units. JR’s morning blood sugar the next day was 157 mg/dL.
What is the best action?
Answer Choices:
If you are thinking about taking the certification exam, this practice test question will set you up for success. Test writers anticipate possible answers based on the details in the question. They will wave those “juicy answers” right under your nose. Your job is to weed through the particulars, pluck out the most important elements and choose the BEST answer.
Answer 1 is incorrect. 23.23% chose this answer. “Increase basal insulin by 10- 20%.” This is a juicy answer because we typically consider the target glucose range 80-130 fasting and before meals. However, according to ADA Standards, the target glucose range during hospitalization is 140-180 mg/dL in general, and 100-180mg/dL in the non-critical care setting. Based on these inpatient goals, we wouldn’t need to increase basal insulin since JR’s morning glucose of 157 is right on target.
Answer 2 is incorrect. 10.17% of you chose this answer. “Intensify correction scale.” Another juicy answer because we typically consider the target glucose range 80-130 fasting and before meals. However, according to ADA Standards, the target glucose range during hospitalization is 140-180 mg/dL in general, and 100-180mg/dL in the non-critical care setting. Based on these inpatient goals, we wouldn’t need to intensify the correction scale since JR’s morning glucose of 157 is right on target. In addition, correction insulin doesn’t have much impact on fasting glucose. That’s the job of basal insulin.
Answer 3 is correct. About 41.52% of respondents chose this. “Continue with same basal dose.” YES, this is the BEST answer. According to ADA Standards, the target glucose range during hospitalization is 140-180 mg/dL in general, and 100-180mg/dL in the non-critical care setting. Based on these inpatient goals, we wouldn’t need to intensify the basal insulin since JR’s morning glucose of 157 is right on target.
Finally, Answer 4 is incorrect. 25.08% chose this answer. “Ask MS if they are snacking during the night before making adjustments.” Another juicy answer. It doesn’t really matter if MS was snacking, since according to ADA Standards, the target glucose range during hospitalization is 140-180 mg/dL in general, and 100-180mg/dL in the non-critical care setting. Based on these inpatient goals, regardless of whether or not they were snacking, JR’s morning glucose of 157 is right on target.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Research clearly demonstrates the importance of glucose control during hospitalization to improve outcomes not only in the inpatient setting but after discharge. This course reviews the evidence that supports inpatient glucose control & outlines practical strategies to achieve targets in the inpatient setting. We incorporate the latest American Diabetes Association’s (ADA) Standards of Medical Care in Diabetes & provide links to resources & inpatient management templates.
Objectives:
Intended Audience: A great course for healthcare professionals seeking strategies to manage and improve inpatient diabetes care.
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
For last week’s practice question, we quizzed participants on gestational diabetes & medication. A whopping 70% of respondents chose the best answer – great job. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
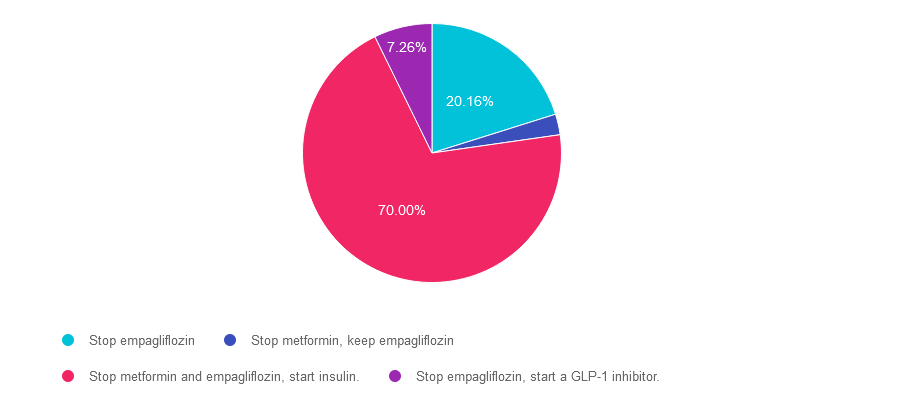
Question: AR has PCOS and type 2 diabetes and is in shock because they just discovered they are 6 weeks pregnant. AR takes metformin 1000mg BID plus empagliflozin (Jardiance) 25 mg and their most recent A1C is 8.6%.
Which of the following actions do you recommend?
Answer Choices:
If you are thinking about taking the certification exam, this practice test question will set you up for success. Test writers anticipate possible answers based on the details in the question. They will wave those “juicy answers” right under your nose. Your job is to weed through the particulars, pluck out the most important elements and choose the BEST answer.
Answer 1 is incorrect. 20.16% chose this answer. “Stop empagliflozin.” It is true that empagliflozin and all SGLT-2’s are not indicated during pregnancy. However, there is a better answer given that her A1C of 8.6% is above the pregnancy target of less than 6.5%.
Answer 2 is incorrect. 2.58% of you chose this answer. “Stop metformin, keep empagliflozin.” Empagliflozin and all SGLT-2’s are contraindicated during pregnancy, so this answer is not the best choice.
Answer 3 is correct. About 70% of respondents chose this. “Stop metformin and empagliflozin, start insulin.” GREAT JOB. Given that her A1C of 8.6% is above the pregnancy target of less than 6.5%, insulin absolutely needs to be started to get glucose to goal. According to the ADA Standards, the provider may opt to continue the metformin treatment for PCOS for the first trimester But given the urgent need to get blood glucose to target, this individual will be most effectively managed with a combination of nutrition therapy and insulin.
Finally, Answer 4 is incorrect. 7.26% chose this answer. “Stop empagliflozin, start a GLP-1 inhibitor.” Yes, we need to stop empagliflozin since all SGLT-2’s are contraindicated during pregnancy. However, GLP-1 Inhibitors are also contraindicated during pregnancy, so this answer is incorrect.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Pregnancy with diabetes is confronted with a variety of issues that require special attention, education, & understanding. This course reviews those special needs while focusing on Gestational Diabetes & Pre-Existing Diabetes. Included are the most recent diagnostic criteria, management goals, & prevention of complications during pregnancy. This is a helpful review for Certification Exams & those who want more information on people who are pregnant & live with diabetes.
Objectives:
Intended Audience: A great course for healthcare professionals seeking to enhance their knowledge of the issues surrounding pregnancy and diabetes and appropriate care to improve outcomes.
Research clearly demonstrates the importance of glucose control during hospitalization to improve outcomes not only in the inpatient setting but after discharge. This course reviews the evidence that supports inpatient glucose control & outlines practical strategies to achieve targets in the inpatient setting. We incorporate the latest American Diabetes Association’s (ADA) Standards of Medical Care in Diabetes & provide links to resources & inpatient management templates.
Objectives:
Intended Audience: A great course for healthcare professionals seeking strategies to manage and improve inpatient diabetes care.