
Subscribe
eNewsletter
Ready to get certified?
Free CDCES Coach App
eNewsletter
Free CDCES Coach App

For last week’s practice question, we quizzed participants on gestational diabetes & pregnancy complications. 68% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question: AR has PCOS type 2 diabetes and worried because they just discovered they are 6 weeks pregnant. AR takes metformin 1000mg BID plus empagliflozin (Jardiance) 25 mg and their most recent A1C is 8.6%.
Which of the following is a potential complication associated with hyperglycemia during the first 10 weeks of pregnancy?
Answer Choices:
If you are thinking about taking the certification exam, this practice test question will set you up for success. Test writers anticipate possible answers based on the details in the question. They will wave those “juicy answers” right under your nose. Your job is to weed through the particulars, pluck out the most important elements and choose the BEST answer.
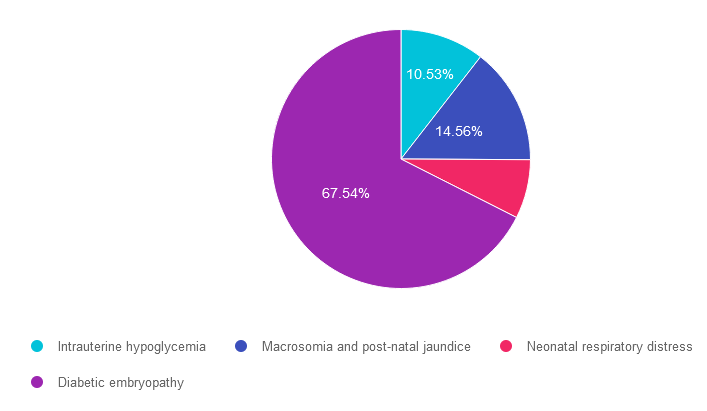
Answer 1 is incorrect. 10.53% chose this answer. “Intrauterine hypoglycemia.” Although this answer is tempting, it is not accurate. If the fetus experienced elevated blood sugars (from mom) during gestation, this stimulates increased fetal production of insulin. After delivery, baby’s who were exposed to intrauterine hyperglycemia are at higher risk of post-delivery hypoglycemia (not intrauterine hypoglycemia).
Answer 2 is incorrect. 14.56% of you chose this answer. “Macrosomia and post-natal jaundice.” Although this answer is tempting, it is not accurate. If the fetus experienced elevated blood sugars (from mom) during their first 10 weeks of gestation, this stimulates increased fetal production of insulin and can stimulate extra fat stores later in pregnancy leading to larger babies and higher risk for post delivery jaundice. However, the question is asking, what complications can elevated blood sugars cause during their first 10 weeks of pregnancy when the organs are developing?
Answer 3 is kind of incorrect. About 7.37% of respondents chose this. “Neonatal respiratory distress.” The question is asking, if the fetus experienced elevated blood sugars (from mom) during the first 10 weeks of gestation, what complications can elevated blood sugars cause during the first trimester pregnancy when the organs are developing? The lungs can be affected by first trimester hyperglycemia, causing the newborn to struggle with respiratory distress.
Finally, Answer 4 is correct. 67.54% chose this answer. “Diabetic embryopathy.” GREAT JOB. This is the best answer. If the fetus experienced elevated blood sugars (from mom) during the first 10 weeks of gestation, embryonic complications result from elevated blood sugars during the first trimester pregnancy when the organs are developing. These can include, congenital heart disease, renal anomalies and caudal regression.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Pregnancy with diabetes is confronted with a variety of issues that require special attention, education, & understanding. This course reviews those special needs while focusing on Gestational Diabetes & Pre-Existing Diabetes. Included are the most recent diagnostic criteria, management goals, & prevention of complications during pregnancy. This is a helpful review for Certification Exams & those who want more information on people who are pregnant & live with diabetes.
Objectives:
Intended Audience: A great course for healthcare professionals seeking to enhance their knowledge of the issues surrounding pregnancy and diabetes and appropriate care to improve outcomes.
Research clearly demonstrates the importance of glucose control during hospitalization to improve outcomes not only in the inpatient setting but after discharge. This course reviews the evidence that supports inpatient glucose control & outlines practical strategies to achieve targets in the inpatient setting. We incorporate the latest American Diabetes Association’s (ADA) Standards of Medical Care in Diabetes & provide links to resources & inpatient management templates.
Objectives:
Intended Audience: A great course for healthcare professionals seeking strategies to manage and improve inpatient diabetes care.
We want to fix our mistake and clarify this important information. For last month’s practice question, a participant reached out to us and kindly shared that one of the medications listed was actually recently approved by the FDA for kids ages 10-17. We want to make this right, so you can pass on updated info to people living with diabetes and your colleagues, plus prepare for exam success! Look for 2 correct answers and explanations for this Rationale of the Week.
Question: KS is 14 years old and recently diagnosed with type 2 diabetes. Their A1C is 8.6%, LDL cholesterol is 137 mg/dL and their GFR is greater than 90.
Based on this clinical information and the ADA Standards for Pediatric Care, in addition to lifestyle and behavior changes, what medication(s) would be recommended?
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Based on this clinical information and the ADA Standards for Pediatric Care, in addition to lifestyle and behavior changes, what medication(s) would be recommended?
Answer Choices:
If you are thinking about taking the certification exam, this practice test question will set you up for success. Test writers anticipate possible answers based on the details in the question. They will wave those “juicy answers” right under your nose. Your job is to weed through the particulars, pluck out the most important elements and choose the BEST answer.
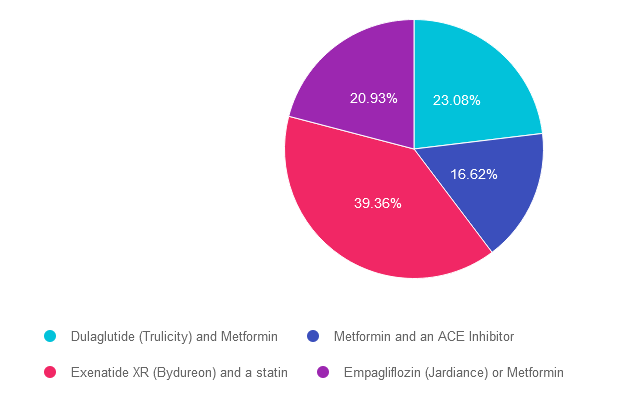
Answer 1 is CORRECT. 23.08% chose this answer. “Dulaglutide (Trulicity) and Metformin.” Both metformin and Dulaglutide (Trulicity) are FDA approved for children starting at age of ten. Dulaglutide was recently FDA approved for pediatrics up at doses up to 1.5 mg per week. We have updated our eMed PocketCards to include this GLP-1 RA as approved for kids ages 10-17.
Answer 2 is incorrect. 16.62% of you chose this answer. “Metformin and an ACE Inhibitor.” Although this answer if tempting, because metformin is FDA approved for children starting at age of ten, there is no mention of hypertension that would justify starting an ACE Inhibitor. See Med PocketCards. For this reason, this is not the best answer.
Answer 3 is CORRECT. About 39.36% of respondents chose this. “Exenatide XR (Bydureon) and a statin.” YES, this is the BEST answer. GREAT JOB. Two of the GLP-1 RA’s are approved for kids including exenatide XR and liraglutide. See Med PocketCards. In addition, statins are indicated for children age 10 or greater if they have diabetes and an LDL cholesterol of 130 mg/dL or greater.
Finally, Answer 4 is incorrect. 20.93% chose this answer. “Empagliflozin (Jardiance) or Metformin.” Although this answer if tempting, because metformin is FDA approved for children starting at age of ten, none of the SGLT-2’s are approved for pediatrics, including empagliflozin. See Med PocketCards. For this reason, this is not the best answer.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity! For more information, see ADA Standard 14 on Children and Adolescents or join our webinar (see below).
This course includes updated goals & guidelines for children living with type 1 or type 2 diabetes. This course discusses the special issues diabetes educators need to be aware of when working with children with diabetes & their families. We discuss the clinical presentation of diabetes, goals of care, & normal growth & development through the early years through adolescence. Strategies to prevent acute & long-term complications are included with an emphasis on positive coping for families & children with diabetes.
Objectives:
Intended Audience: A great course for healthcare professionals seeking information about providing care for children with diabetes and their families.
Don’t worry if you can’t make it live. Your registration guarantees access to the recorded version in the Online University.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
For last week’s practice question, we quizzed participants on what is wrong with JR’s foot. 51% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question: JR arrives at the clinic wearing a walking boot due to a recent foot injury. Tells you that they “banged their foot” on some farm equipment and since then it has been warm and swollen. It hurt at first, but the pain has diminished with time.
When JR takes off the boot, you see that the left foot needs attention.
Based on this photo, what diabetes-related foot condition do you suspect?

Answer Choices:
If you are thinking about taking the certification exam, this practice test question will set you up for success. Test writers anticipate possible answers based on the details in the question. They will wave those “juicy answers” right under your nose. Your job is to weed through the particulars, pluck out the most important elements and choose the BEST answer.
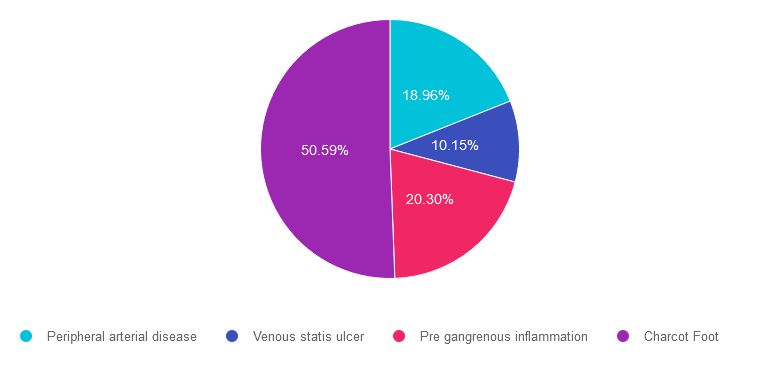
Answer 1 is incorrect. 18.96% chose this answer. Peripheral arterial disease. People experiencing peripheral arterial disease usually present with thinner, pale, lower extremities. They complain of pain in their calves or buttocks when walking due to intermittent claudication. Pulses are difficult to palpate due to diminished circulation to lower extremities.
Answer 2 is incorrect. 10.15% of you chose this answer. Venous statis ulcer. This person may have lower extremity venous disease as evidenced by the marked edema and darkened skin. However, although the foot is red and swollen there is no ulcer present in this photo.
Answer 3 is incorrect. About 20.30% of respondents chose this. Pre gangrenous inflammation. This person is certainly experiencing inflammation and edema. However, we can’t determine if their lower extremity is moving toward gangrene just from this photo.
Finally, Answer 4 is correct. 50.59% chose this answer. Charcot Foot. YES, this is the BEST answer. GREAT JOB. This person arrived with a suddenly misshapen foot, coupled with edema and redness. The skin was intact and the individual denied pain. This presentation is the hallmark of Charcot foot, a condition that is a combination of neuropathy and diminished circulation coupled with elevated blood glucose levels. It requires immediate medical attention by a foot specialist. JR sought care from a Podiatrist and his foot was secured in a cast to protect the foot and prevent further damage.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
People with diabetes are at increased risk of Lower Extremity Complications. This course reviews the steps involved in performing a detailed assessment of the lower extremities, including how to use a monofilament and tuning fork to detect neuropathy. We also discuss the significance of the Ankle Brachial Index and strategies to prevent lower extremity complications.
Objectives:
Intended Audience: This is a great course for healthcare professionals who want to learn the steps involved in providing a thorough lower extremity assessment.
Don’t worry if you can’t make it live. Your registration guarantees access to the recorded version in the Online University.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
For last week’s practice question, we quizzed participants on statins & the risk of dementia. 49% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question: LR is 78 years old with a new diagnosis of diabetes. Their A1C is 7.9%, LDL cholesterol is 98 mg/dL, GFR is 58 mg/g and their BP is 124/78. The provider recommends a referral to the RD and DSME program and writes a prescription for metformin XR 500mg daily and lovastatin 20mg. LR is worried about taking a statin because they heard it can cause dementia.
Based on the ADA Standards, what is the best response?
Answer Choices:
If you are thinking about taking the certification exam, this practice test question will set you up for success. Test writers anticipate possible answers based on the details in the question. They will wave those “juicy answers” right under your nose. Your job is to weed through the particulars, pluck out the most important elements and choose the BEST answer.
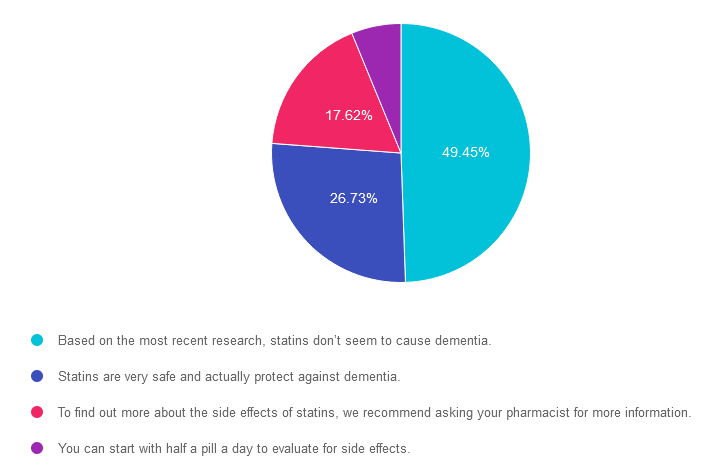
Answer 1 is correct. 49.45% chose this answer. “Based on the most recent research, statins don’t seem to cause dementia.” YES, is the BEST answer. According to ADA 2023 SOC 10 a recent systematic review of the U.S. Food and Drug Administration’s (FDA’s) postmarketing surveillance databases, randomized controlled trials, and cohort, case-control, and cross-sectional studies evaluating cognition in patients receiving statins found that published data do not reveal an adverse effect of statins on cognition (138). Therefore, a concern that statins or other lipid-lowering agents might cause cognitive dysfunction or dementia is not currently supported by evidence and should not deter their use in individuals with diabetes at high risk for ASCVD (138).
Answer 2 is incorrect. 26.73% of you chose this answer. “Statins are very safe and actually protect against dementia.” Although the first part of this statement is correct, statins are safe, there is no evidence presented in the ADA Standards that statins protect against dementia.
Answer 3 is incorrect. About 17.62% of respondents chose this. “To find out more about the side effects of statins, we recommend asking your pharmacist for more information.” Although pharmacists are incredibly knowledgeable about medications, diabetes specialists can relate evidence based information to the people we serve, instead of making them take additional action to get the information they need to move forward. The good news is that there is no evidence that statins or other lipid-lowering agents might cause cognitive dysfunction or dementia and their use is recommended in individuals with diabetes at high risk for ASCVD.
Finally, Answer 4 is incorrect. 6.19% chose this answer. “You can start with half a pill a day to evaluate for side effects.” This approach is tempting, but it doesn’t address the fear of the statin causing dementia. The good news is that there is no evidence that statins or other lipid-lowering agents might cause cognitive dysfunction or dementia and their use is recommended in individuals with diabetes at high risk for ASCVD.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
We are living longer & more people are getting diabetes. The American Diabetes Association has updated the Older Adults Standards, with special attention to considering the reduction of medication & insulin therapy intensity. The older population has unique issues & special needs that require consideration as we provide diabetes self-management education. This online course highlights key areas of assessment, intervention, and advocacy for older clients living with diabetes.
Objectives:
Intended Audience: An important course for healthcare professionals seeking to gain an understanding of the special issues and goals for older adults.
Don’t worry if you can’t make it live. Your registration guarantees access to the recorded version in the Online University.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
For last week’s practice question, we quizzed participants on diabetes distress. 78% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question: JR has type 1 diabetes and tells you, “My doctor just doesn’t seem to understand how to manage type 1 diabetes. Sometimes, I just skip my appointments because it feels like a waste of time.” JR’s most recent A1C was 8.7% and their time in ranges keeps decreasing with each visit.
Based on this, you realize that JR’s provider-related diabetes distress:
Answer Choices:
If you are thinking about taking the certification exam, this practice test question will set you up for success. Test writers anticipate possible answers based on the details in the question. They will wave those “juicy answers” right under your nose. Your job is to weed through the particulars, pluck out the most important elements, get rid of false answers, do any math very carefully and choose the BEST answer.
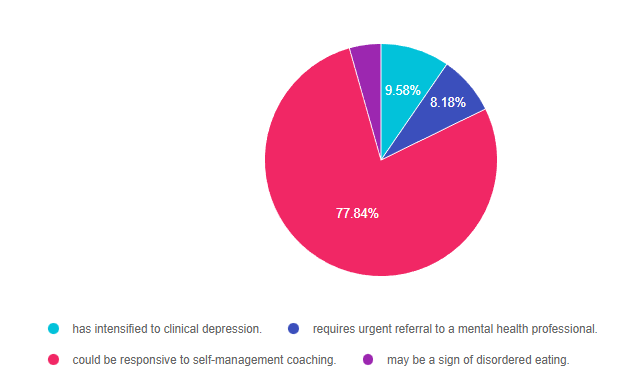
Answer 1 is incorrect. 9.58% chose this answer. “has intensified to clinical depression.” This is a tempting answer, but we don’t enough evidence to support that JR is struggling with depression. If we had JR complete the Diabetes Distress Scale, he would certainly score high on provider related distress based on this statement, “My doctor just doesn’t seem to understand how to manage type 1 diabetes. Sometimes, I just skip my appointments because it feels like a waste of time.” These comments certainly fit in the distress category. Through careful questioning and exploration, the diabetes educator could certainly help with problem solving.
Answer 2 is incorrect. 8.18% of you chose this answer. “requires urgent referral to a mental health professional.” Based on JR’s statement, “My doctor just doesn’t seem to understand how to manage type 1 diabetes. Sometimes, I just skip my appointments because it feels like a waste of time,” JR is certainly in distress. However, there is no language indicating that JR is in imminent danger of self-harm. Through careful questioning and exploration, the diabetes educator could certainly carefully assess JR’s mental health state and help with problem solving and referrals as needed.
Answer 3 is correct. About 77.84% of respondents chose this. “could be responsive to self-management coaching.” YES. This is the best answer. We could start by administering the Diabetes Distress Scale and then hone in on the high scoring areas. Then through careful questioning and exploration, the diabetes educator could certainly help with problem solving and identify if additional resources or referrals are needed.
Finally, Answer 4 is incorrect. 4.39% chose this answer. “may be a sign of disordered eating.” but we don’t enough evidence to support that JR is experiencing disordered eating. However, if we had JR complete the Diabetes Distress Scale, he would certainly score high on provider related distress based on this statement, “My doctor just doesn’t seem to understand how to manage type 1 diabetes. Sometimes, I just skip my appointments because it feels like a waste of time.”
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Addressing diabetes distress can be tricky, even for seasoned healthcare professionals.
We invite you to attend this hands-on training program that provides the essential steps to address diabetes distress combined with an innovative approach to glucose management. Our experts offer realistic strategies to address diabetes distress that you can immediately apply to your practice setting. Plus, the ReVive 5 Program provides a breadth of tools and resources to create more meaningful connections with people with diabetes.
“ReVive 5” breathes new life into our relationship with diabetes, bringing a fresh perspective to both the person with diabetes and the provider.
Team of Experts: ReVive 5 is taught by a team of 3 Interdisciplinary Experts:

Accredited Training Program:
Speakers Interviews – Learn more about the ReVive 5 Team
What is the Biggest Takeaway when Addressing Diabetes Distress? – Dr. Susan Guzman
Do you have to be a Mental Health Expert to Tackle Diabetes Distress? – Dr. Lawrence Fisher
Why I Transformed my Approach to Diabetes Self-Management Education- Coach Beverly
Don’t worry if you can’t make it live. Your registration guarantees access to the recorded version in the Online University.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
For last week’s practice question, we quizzed participants on counting every pen(ny.) 47% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question: KL takes 5-10 units of insulin glulisine (Apidra) based on an insulin scale before each of their 3 daily meals and 30 units of glargine (Basaglar) at bedtime.
Based on this information, how many u-100 glulisine (Apidra) insulin pens would KL use a month?
Answer Choices:
If you are thinking about taking the certification exam, this practice test question will set you up for success. Test writers anticipate possible answers based on the details in the question. They will wave those “juicy answers” right under your nose. Your job is to weed through the particulars, pluck out the most important elements, get rid of false answers, do any math very carefully and choose the BEST answer.
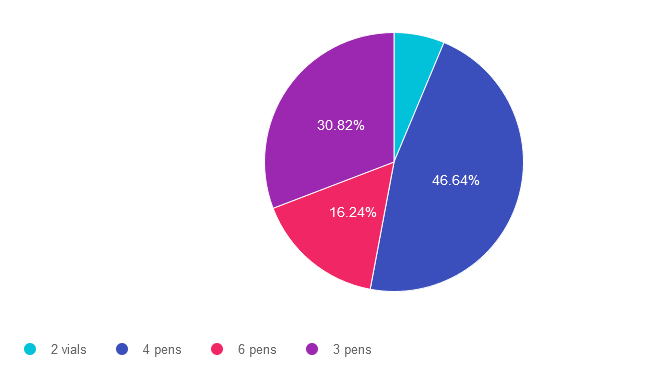
Answer 1 is incorrect. 6.31% chose this answer. “2 vials.” One way to quickly eliminate a wrong answer is to see if the units in the question match the units in the answer. The question asks, “How many pens” would JR need a month and this answer is in “vials”. We can cross this one off as false. **See complete math explanation below.
Answer 2 is correct. 46.64% of you chose this answer. “4 pens.” YES.. Great job. You not only calculated JR’s insulin needs, but added in extra insulin for priming too! **See complete math explanation below.
Answer 3 is incorrect. About 16.24% of respondents chose this. “6 pens.” This was a juicy answer that lured respondents into adding together the glulisine and glargine dose. The answer only asks for how many glulisine pens would JR need a month. **See complete math explanation below.
Finally, Answer 4 is incorrect. 30.82% chose this answer. “3 pens.” This was the juiciest answer of all. However, it doesn’t take into account the 2 units of insulin used to prime the pen before each injection. Also, if they had 3 pens of 300 units each, what if they made a mistake or wasted a dose, or needed a little extra.. they might be short on insulin. We always want to allow for a little cushion, just in case. **See complete math explanation below.
**Complete explanation – Doing the math.
If JR takes 5-10 units of insulin glulisine (Apidra) 3 times a day, we have to assume they will be taking the highest dose each time, so they don’t run out of insulin. That means JR uses 30 units a day of glulisine. 30 units a day x 30 days in a month = 900 units. But wait, JR needs to prime the pen first with a 2 unit “air shot” before each injection to make sure insulin is flowing through the needle before each of their 3 injections. So this means that JR is using up to 12 units of insulin 3 times a day or 36 units x 30 days = 1,080 units of glulisine a month. The next thing we need to know is that each U-100 glulisine pen holds 300 units of insulin (see our Insulin Storage Cheat Sheet 2023). Now, we can do the math. JR uses 1,080 units of insulin a day. Since each pen holds 300 units, we take 1080 and divide by 300 for a total of 3.6. This means JR will need 4 pens of glulisine each month to manage their diabetes.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Whether you are a novice or an expert in providing diabetes care, we invite you to attend this exciting training program that provides the essential steps to address diabetes distress combined with an innovative approach to glucose management that will revolutionize your practice.
“ReVive 5” breathes new life into our relationship with diabetes, bringing a fresh perspective to both the person with diabetes and the provider.
Team of Experts: ReVive 5 is taught by a team of 3 Interdisciplinary Experts:
Accredited Training Program:
Speakers Interviews – Learn more about the ReVive 5 Team
What is the Biggest Takeaway when Addressing Diabetes Distress? – Dr. Susan Guzman
Do you have to be a Mental Health Expert to Tackle Diabetes Distress? – Dr. Lawrence Fisher
Why I Transformed my Approach to Diabetes Self-Management Education- Coach Beverly
Don’t worry if you can’t make it live. Your registration guarantees access to the recorded version in the Online University.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
For last week’s practice question, we quizzed participants on being at risk for NASH. 63% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question: JR is 46 years old with type 2 diabetes and a BMI of 33. In addition, JR has hypertension and hyperlipidemia, with elevated liver enzymes (ALT and AST).
According to the latest ADA Standards, which of the following would best help determine if JR is at risk for liver fibrosis and cirrhosis?
Answer Choices:
If you are thinking about taking the certification exam, this practice test question will set you up for success. Test writers anticipate possible answers based on the details in the question. They will wave those “juicy answers” right under your nose. Your job is to weed through the particulars, pluck out the most important elements and choose the BEST answer.
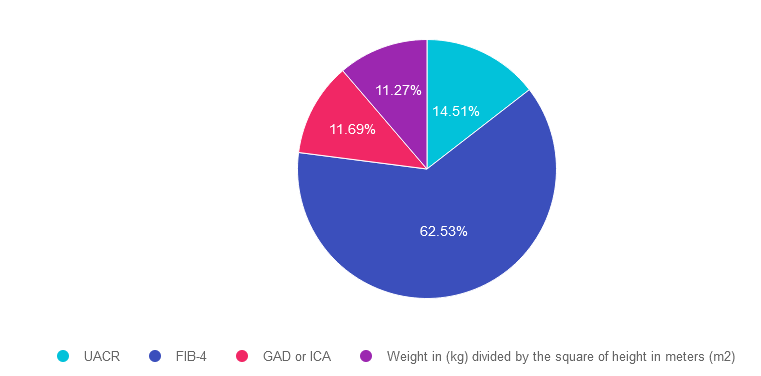
Answer 1 is incorrect. 14.51% chose this answer. “UACR.” This is a juicy answer, however the Urinary Albumin Creatinine Ratio (UACR) evaluates kidney function and doesn’t provide any hepatic insights. Instead we would recommend the Fibrosis-4 Index for Liver Fibrosis helps determine risk of hepatic cirrhosis and inflammation (see answer 2).
Answer 2 is correct. 62.53% of you chose this answer. “FIB-4.” GREAT JOB. The Fibrosis-4 Index for Liver Fibrosis helps determine risk of hepatic cirrhosis and inflammation. By entering the person’s age, AST, ALT and Platelet count using the FIB-4 calculator, a risk level is calculated (see slide below). The hope is that by screening for hepatic issues early, we can take action to protect the liver and improve outcomes.
Answer 3 is incorrect. About 11.69% of respondents chose this. “GAD or ICA.” Although this answer is familiar, it does not match the intent of the question. GAD and ICA are blood tests to determine if someone has autoimmune mediated type 1 diabetes. Instead we would recommend the Fibrosis-4 Index for Liver Fibrosis helps determine risk of hepatic cirrhosis and inflammation (see answer 2).
Finally, Answer 4 is incorrect. 11.27% chose this answer. “Weight in (kg) divided by the square of height in meters (m2).” This answer is also familiar since it is the formula to determine a person’s body mass index (BMI). Instead we would recommend the Fibrosis-4 Index for Liver Fibrosis helps determine risk of hepatic cirrhosis and inflammation (see answer 2).
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity! Learn more by attending our Virtual Conference plus save $100 through April 18, 2023.

Your team is invited to our Virtual DiabetesEd™ Training Conference! Set your team apart and prepare for diabetes certification!
Join this state-of-the-art conference taught by content experts, Diana Isaacs, PharmD, BCPS, BCACP, BC-ADM, CDCES, Beverly Thomassian RN, MPH, CDCES, BC-ADM, and Ashley LaBrier who are passionate about improving diabetes care.
Group discounts are available!*
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
For last week’s practice question, we quizzed participants on having their cake and eating it too. A whopping 94% of respondents chose the best answer. We want to celebrate your success and give you all a shout out for a job well done.
Before we start though if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question: AJ is a 9-year-old with type 1 diabetes, A1c of 7.2%, and uses an insulin pump and CGM. They ask you how to include a piece of birthday cake for an upcoming birthday celebration.
What is the best advice?
Answer Choices:
If you are thinking about taking the certification exam, this practice test question will set you up for success. Test writers anticipate possible answers based on the details in the question. They will wave those “juicy answers” right under your nose. Your job is to weed through the particulars, pluck out the most important elements and choose the BEST Person-Centered answer.
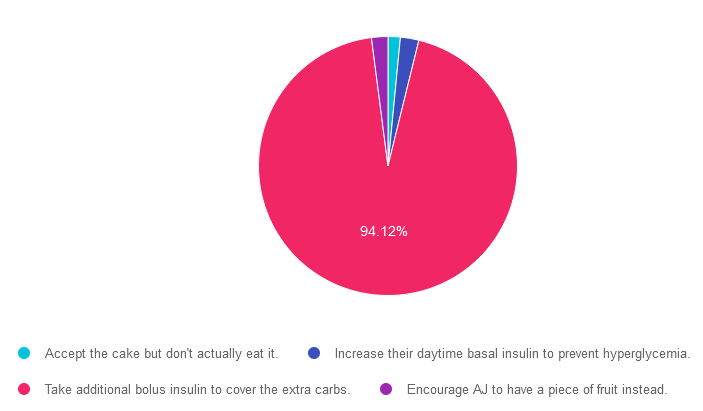
Answer 1 is incorrect. 1.53% chose this answer. “Accept the cake but don’t actually eat it.” Since this doesn’t honor AJ’s choice to accept and enjoy the cake, it is not the best answer. People with diabetes can absolutely enjoy special treats by adjusting their bolus insulin dose to account for the extra carbs to prevent post cake hyperglycemia.
Answer 2 is incorrect. 2.3% of you chose this answer. “Increase their daytime basal insulin to prevent hyperglycemia.” People with diabetes can absolutely enjoy special treats by adjusting their bolus insulin dose to account for the extra carbs to prevent post cake hyperglycemia.
Answer 3 is correct. About 94.12% of respondents chose this. “Take additional bolus insulin to cover the extra carbs.” YAY! This person centered approach is the BEST guilt free answer since it recognizes and respects AJ’s choice to enjoy a piece of birthday cake while still managing blood sugars with extra bolus insulin.
Finally, Answer 4 is incorrect. 2.05% chose this answer. “Encourage AJ to have a piece of fruit instead.” Since this doesn’t honor AJ’s choice to accept and enjoy the cake, it is not the best answer. People with diabetes can absolutely enjoy special treats by adjusting their bolus insulin dose to account for the extra carbs to prevent post cake hyperglycemia.
We hope you appreciate this week’s person-centered rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
You are invited to join our Virtual Conference with our Nutrition expert speaker, Ashley LaBrier, MS, RD, CDCES, who will be providing a half-day presentation on this important topic!

Ashley LaBrier, MS, RD, CDES, is an innovator in the field of diabetes, nutrition, and technology. Ashley is a consultant and the Diabetes Education Program Coordinator at the Salinas Valley Medical Clinic’s Diabetes & Endocrine Center.
Ms. LaBrier is passionate about providing person-centered education to empower those who live with diabetes. Having been diagnosed with type 1 diabetes herself nearly 20 years ago, she combines her professional knowledge with personal experience and understanding.
Whether you are new to diabetes or a seasoned expert, you’ll benefit from this virtual conference with the latest research plus critical content that you can immediately apply to your clinical practice.
If you are seeking a state-of-the-art review of current diabetes care, this course is for you. Our team has been fine-tuning this course for over fifteen years, and we know what you need. This program can also be a great addition to your CDCES or BC-ADM exam study plan.
Group discounts are available!*
Download Course Flyer | Download Schedule
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.