Subscribe
eNewsletter
Ready to get certified?
Free CDCES Coach App
eNewsletter
Free CDCES Coach App
Free Med Pocket Cards
For last week’s practice question, we quizzed participants on what needs to be included in the initial screening for PAD, according to ADA Standards. 56.08% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question

Peripheral Artery Disease (PAD) is significantly underdiagnosed. While PAD affects around 8.5 million Americans and prevalence rises with age (up to 20% over 60), only 10-20% are clinically diagnosed, highlighting a major gap in awareness and screening.
According to the ADA Standards, what needs to be included in the initial screening for PAD?

Answer A is correct: 56.08% chose this answer, “History of leg fatigue and calf pain when walking.” YES, great job. According to the ADA, if a person presents with leg fatigue and intermittent claudication, a more detailed screening for peripheral arterial disease (PAD) and poor arterial circulation is warranted.
Answer B is incorrect: 21.08% chose this answer, “Lower extremity pain that is worse at night and restless legs.” People experiencing neuropathy will complain of leg pain and burning that is worse when resting. People with PAD complain of leg and buttock pain when walking due to diminished circulation and poor blood flow to muscles that is relieved with rest.
Answer C is incorrect: 12.45% chose this answer, “Leg cramps coupled and frequent unexplained bruising.” Only part of this answer is correct. Although leg cramps or calf pain can occur with PAD, there is not direct association with frequent unexplained bruising.
Answer D is incorrect: 10.4% chose this answer, “Onychomycosis and unusual callus formation.” People with diabetes do have an increased risk of toenail infections and onychomycosis, but this is not associated with the manifestations of PAD.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
For last week’s practice question, we quizzed participants on CS’s A1C climbing after experiencing distress. 50.55% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
CS is a 42-year-old with type 1 diabetes for just over 18 years. In the past year, their A1C changed from 7.4% to 9.1%, and weight increased by 20 pounds. Review of CGM data suggests missed insulin boluses more than 7 times per week, and discussion with CS reveals missed clinic visits due to feeling “burned out”. They score in the moderate range on the Diabetes Distress Scale.
Based on the ADA 2026 Standards of Care, which of the following is the most appropriate next step?
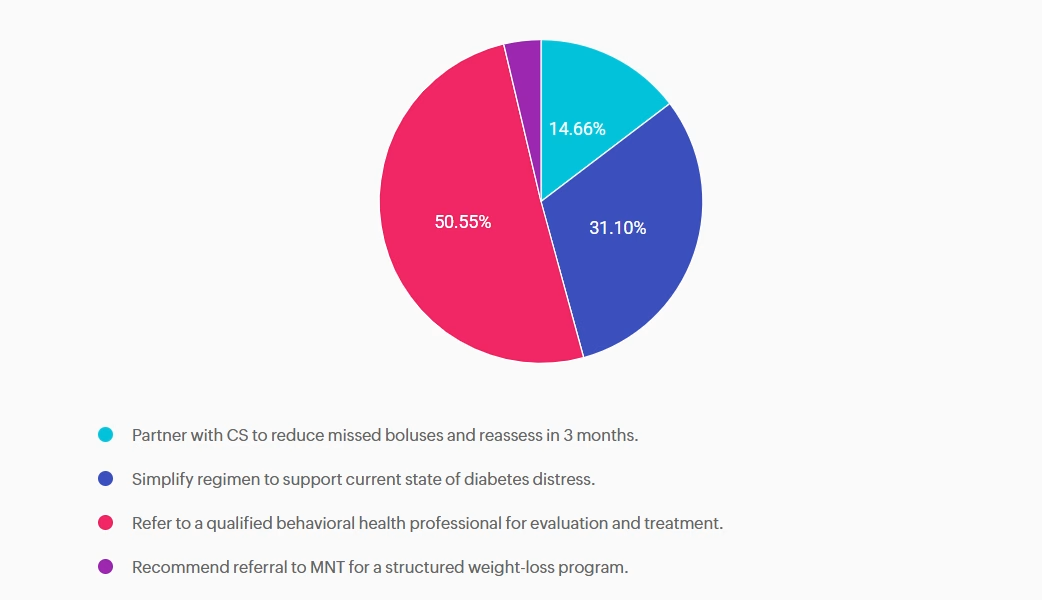
Answer A is incorrect: 14.66% chose this answer, “Partner with CS to reduce missed boluses and reassess in 3 months.” While reducing missed boluses and optimizing insulin therapy are essential to support A1c reduction, this intervention alone does not address the likely underlying psychological barriers to self-management.
Answer B is incorrect: 31.1% chose this answer, “Simplify regimen to support current state of diabetes distress.” While simplifying insulin dosing may be supportive in some cases, without addressing the underlying diabetes distress it is unlikely to achieve sustained improvement.
Answer C is correct: 50.55% chose this answer, “Refer to a qualified behavioral health professional for evaluation and treatment.” The 2026 ADA Standards of Care recommends a referral to a qualified behavioral health professional for evaluation and treatment when diabetes distress, burnout, reduced engagement in diabetes management or other psychosocial factors are impacting self-care and glycemic targets. ¹
Answer D is incorrect: 3.7% chose this answer, “Recommend referral to MNT for a structured weight-loss program.” Focusing solely on weight loss does not address the primary psychosocial barriers and weight gain may be a symptom of underlying behavioral health needs. Evaluation and treatment from a behavioral health provider would be the most appropriate next step.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!

For last week’s practice question, we quizzed participants on Katie needing support with improving her glycemic management, and what would be the best response. 76.5% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Katie is a 14-year-old living with type 1 diabetes since age 10. She uses multiple daily insulin injections (MDI) therapy to manage her diabetes and started using a continuous glucose monitor (CGM) 3 months ago at the recommendation of her endocrinology team. Her A1c has increased to 9.2% since starting CCM technology.
Her mother reports that Katie has episodes of prolonged hyperglycemia when she is away from home. When at home, her mother will remind Katie to bolus based on the alerts she gets on the CGM share app. Katie reports she mutes alarms and alerts because she doesn’t want her classmates to hear them, afraid they will judge her. When you ask if she has uploaded her data to the school nurse or her endocrinology team she says, “The app is really confusing.” Her mother is frustrated with Katie for not paying attention to the CGM, saying, “She can text her friends without any problem; I don’t know why she struggles with the CGM”.
As the diabetes healthcare provider, how can you support Katie in improving her glycemic control?
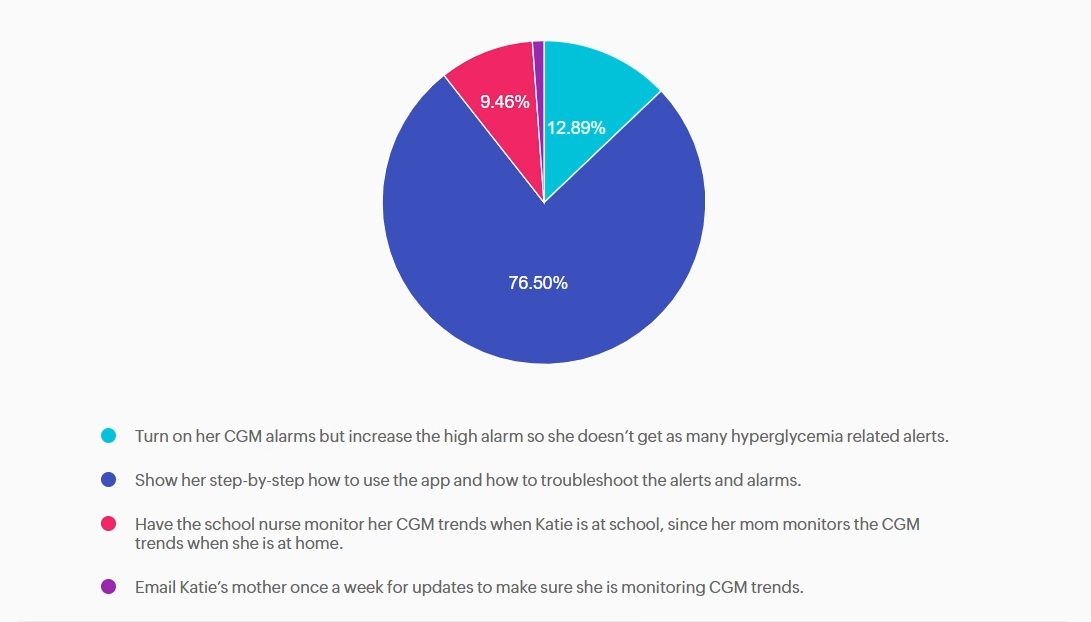
Answer A is incorrect: 12.89% chose this answer, “Turn on her CGM alarms but increase the high alarm so she doesn’t get as many
hyperglycemia related alerts.” Helping Katie turn on and increasing her high alarm will not help improve her glycemic management.
Answer B is correct: 76.5% chose this answer, “Show her step-by-step how to use the app and how to troubleshoot the alerts and alarms.” Guiding Katie through the CGM app and its functions helps her ask questions, resolve issues, and better monitor her glycemic management.
Answer C is incorrect: 9.46% chose this answer, “Have the school nurse monitor her CGM trends when Katie is at school, since her mom monitors the CGM trends when she is at home.” Asking the school nurse to monitor CGM data while Katie is at school is not helping to improve Katie’s self-management skills.
Answer D is incorrect: 1.15% chose this answer, “Email Katie’s mother once a week for updates to make sure she is monitoring CGM
trends.” Emailing Katie’s mother does not help improve Katie’s CGM self-monitoring skills or her confidence level with the CGM app.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Gain fresh insights, practical tools, and a deeper understanding of the latest in person-centered diabetes care. Our expert team brings the ADA Standards of Care to life—covering medications, behavior change, technology, and more!
If you’re preparing for the CDCES or BC-ADM exam, this conference, paired with a handful of free bonus courses, serves as the ideal study companion! Plus, this content counts toward the ADA Standards requirements for CDCES Renewal.
With interactive co-teaching, we keep sessions engaging, relevant, and fun.
Let’s learn and grow together!
Course credits through AMA PRA Category 1 Credits™, ACPE, ANCC, and CDR!
Program Objectives:
Upon completion of this activity, participants should be able to:
For last week’s practice question, we quizzed participants on the new ADA Standards and the development of type 2 diabetes. 42.48% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
According to the new 2026 ADA Standards, “type 2 diabetes is associated with insulin secretory defects related to” which of the following?
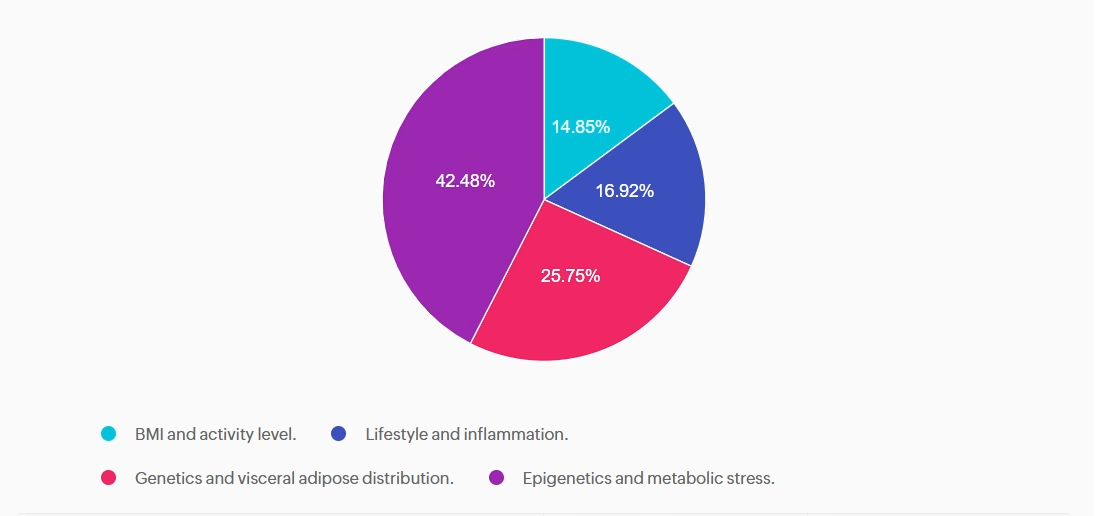
Answer A is incorrect: 14.85% chose this answer, “BMI and activity level.” This answer is incorrect but tempting. BMI level is used as a a screening tool for prediabetes and diabetes risk, but is not included as a factor contributing to secretory defects. According to the ADA, there are four factors related to insulin secretory defects in type 2 diabetes. They include; genetics, epigenetics, metabolic stress and inflammation.
Answer B is incorrect: 16.92% chose this answer, “Lifestyle and inflammation.” This juicy answer is incorrect. Lifestyle is not a direct factor related to insulin secretory defects, but inflammation is a contributor. According to the ADA, there are four factors related to insulin secretory defects in type 2 diabetes. They include; genetics, epigenetics, metabolic stress and inflammation.
Answer C is incorrect: 25.75% chose this answer, “Genetics and visceral adipose distribution.” This answer is incorrect. Visceral adiposity is associated with an increased risk for diabetes, but does not contribute to insulin secretory defects. According to the ADA, there are four factors related to insulin secretory defects in type 2 diabetes. They include; genetics, epigenetics, metabolic stress and inflammation.
Answer D is correct: 42.48% chose this answer, “Epigenetics and metabolic stress.” This answer is correct, GREAT JOB! According to the ADA, there are four factors related to insulin secretory defects in type 2 diabetes. They include; genetics, epigenetics, metabolic stress and inflammation.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!

For last week’s practice question, we quizzed participants on JR studying to take their CDCES exam, and they have questions studying for the 2025 or 2026 ADA Standards of Care. 55.56% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
JR has been diligently studying to take their CDCES exam at the end of January 2026. They are wondering if they should study the 2025 or 2026 ADA Standards of Care.
As a mentor to healthcare professionals entering the field of diabetes, what do you recommend?
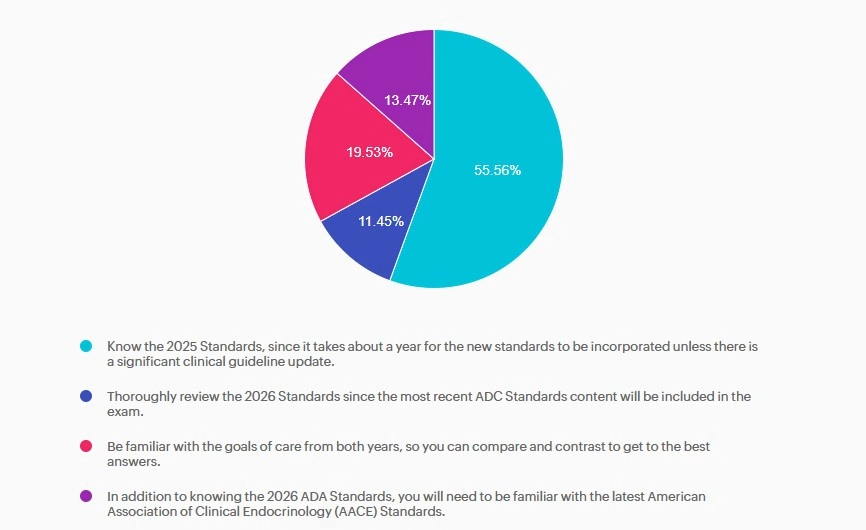
Answer A is correct: 55.56% chose this answer, “Know the 2025 Standards, since it takes about a year for the new standards to be incorporated unless there is a significant clinical guideline update.” Answer A is the BEST answer. It takes at least a year for the CBDCE to update the exam based on the ADA Standards. Knowing the 2025 Standards along with any urgent clinical updates announced in 2026 will help prepare JR for success.
Answer B is incorrect: 11.45% chose this answer, “Thoroughly review the 2026 Standards since the most recent ADC Standards content will be included in the exam.” Answer B is not the best answer. Since it takes at least a year for the CBDCE to update the exam based on the ADA Standards, JR can feel comfortable knowing the 2025 Standards along with any urgent clinical updates announced in 2026.
Answer C is incorrect: 19.53% chose this answer, “Be familiar with the goals of care from both years, so you can compare and contrast to get to the best answers.” Answer C is not the best answer. Thinking about comparing and contrasting two consecutive years standards and lead to testing confusion. JR can feel comfortable knowing the 2025 Standards along with any urgent clinical updates announced in 2026.
Answer D is incorrect: 13.47% chose this answer, “In addition to knowing the 2026 ADA Standards, you will need to be familiar with the latest American Association of Clinical Endocrinology (AACE) Standards.” Answer D is not the best answer. Since it takes at least a year for the CBDCE to update the exam based on the ADA Standards, JR can feel comfortable knowing the 2025 Standards along with any urgent clinical updates announced in 2026.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
For last week’s practice question, we quizzed participants on SJ having questions about their insulin pen, and what would be the best response. 41.72% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
SJ is 52 years old with a 10-year history of type 2 diabetes. They recently started on insulin degludec U-100 Flex Touch pen 15 units per day. At a follow-up visit, SJ brings their insulin pen and mentions they have been keeping it in their work bag since starting therapy. They are unsure how long they can continue to use this same pen.
What is the best advice for SJ for insulin storage in this situation?
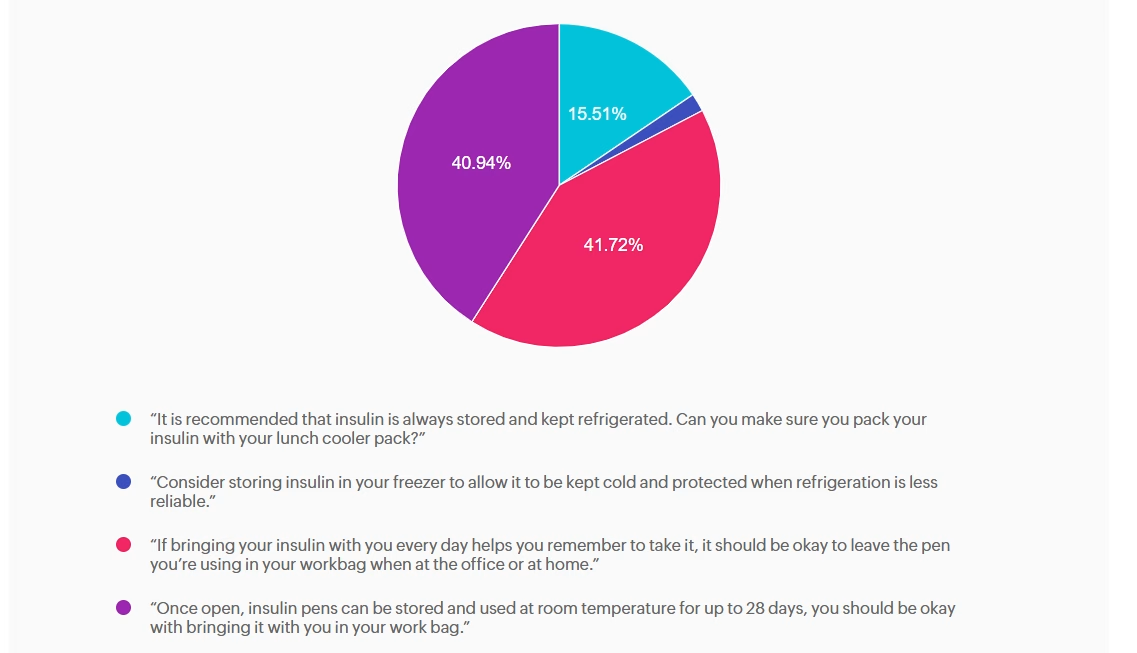
Answer A is incorrect: 15.51% chose this answer, “It is recommended that insulin is always stored and kept refrigerated. Can you make
sure you pack your insulin with your lunch cooler pack?” While refrigeration is ideal for insulin storage, insulin does not always need to be refrigerated. Once in use, most insulins, including degludec, are stable at room temperature (below 86F or 30 C). Advising refrigeration may create unnecessary barriers and does not reflect degludec’s stability profile.
Answer B is incorrect: 1.83% chose this answer, “Consider storing insulin in your freezer to allow it to be kept cold and protected when
refrigeration is less reliable.” Freezing damages insulin molecules, making the insulin ineffective and unsafe to use. This option contradicts manufacturer and clinical safety guidance.
Answer C is correct: 41.72% chose this answer, “If bringing your insulin with you every day helps you remember to take it, it should be
okay to leave the pen you’re using in your workbag when at the office or at home.” Insulin degludec is stable at room temperature below 86°F (30°C) for up to 56 days (8 weeks) once opened. If SJ’s work bag is not exposed to excessive heat or freezing, keeping the pen there is acceptable and may in fact support consistent dosing. We can also calculate SJ’s monthly insulin pen usage (15 units per day + 2 unit prime per injection = 510 units per month or 2 pens per month), knowing he will easily use more insulin than open insulin pen stability time window.
Answer D is incorrect: 40.94% chose this answer, “Once open, insulin pens can be stored and used at room temperature for up to 28 days, you should be okay with bringing it with you in your work bag.” While it is correct that insulin does not always require refrigeration once in use, the specific duration varies by insulin type; degludec lasts longer than 28 days.
To learn more, check out our Insulin Storage Cheat Sheet.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
For last week’s practice question, we quizzed participants on RT forgetting their insulin, and what would be the best response. 62.93% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
JR was recently diagnosed with type 2 diabetes, but based on their history of pancreatitis, you suspect JR actually has Diabetes Type 3c.
Which of the following symptoms match a diagnosis of Diabetes Type 3c?
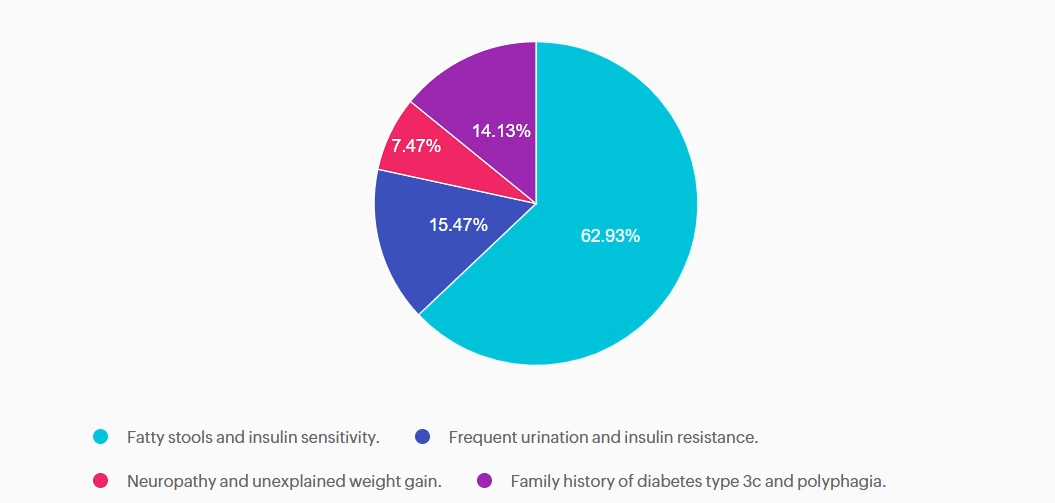
Answer A is correct: 62.93% chose this answer, “Fatty stools and insulin sensitivity.” Steatorrhea, or fatty stools, results from poor fat digestion due to insufficient pancreatic enzymes—a key feature of type 3c diabetes, with it’s hallmark exocrine enzyme insufficiency. People with diabetes type 3c, can also be very insulin sensitive, since they don’t have the insulin resistance associated with type 2 diabetes. In addition to diabetes medications, they may benefit from pancreatic enzyme replacement therapy (PERT) to improve absorption of fatty foods and decrease steatorrhea.
Answer B is incorrect: 15.47% chose this answer, “Frequent urination and insulin resistance.” Frequent urination and insulin resistance is associated with type 2 diabetes. With type 3c, since many of the beta cells are destroyed due to trauma not genetics, these individuals may have polyuria from hyperglycemia, but they are not usually insulin resistant, just deficient.
Answer C is incorrect: 7.47% chose this answer, “Neuropathy and unexplained weight gain.” They may get neuropathy if their blood glucose is elevated for a long period of time, but that is not part of the differential. People with type 3c usually experience weight loss due to the lack of pancreatic enzymes that help with nutrient absorption.
Answer D is incorrect: 14.13% chose this answer, “Family history of diabetes type 3c and polyphagia.” Type 3c diabetes is not passed on through genes, it is due to exocrine damage to the pancreas which can lead to destruction of beta cells. Most common causes of diabetes type 3c include pancreatitis, cystic fibrosis, pancreatic cancer, and hemochromatosis. Some people could experience extreme hunger if their glucose levels are elevated for an extended period of time.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
For last week’s practice question, we quizzed participants on Gestational Diabetes: Diabetes Care in the Fourth Trimester. 51% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
MT is a 29-year-old with Type 1 diabetes who is currently 14 weeks pregnant. She uses a continuous glucose monitor (CGM) with concurrent fingersticks and uploads her glucose data weekly. Her CGM settings was already set to the recommended time in
range and the latest CGM report shows the following: time in range (TIR): 67%, time below range: 6%, time above range: 27%.
Based on current ADA Standard of Care, which of the following statements is most accurate regarding her CGM values?
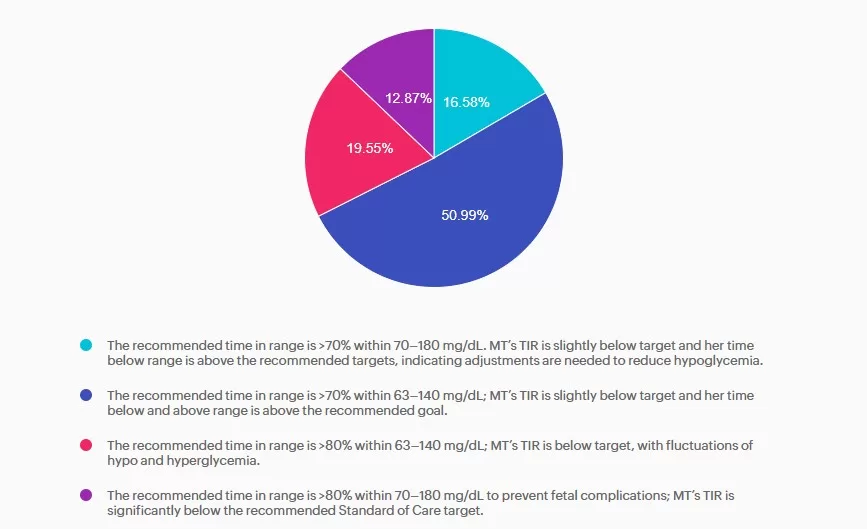
Answer A is incorrect: 16.58% chose this answer, “The recommended time in range is >70% within 70–180 mg/dL. MT’s TIR is slightly below target and her time below range is above the recommended targets, indicating adjustments are needed to reduce hypoglycemia.” Answer A is incorrect. The answer uses non-pregnancy CGM target range of 70–180 mg/dL. Pregnancy target range for individuals with type 1 diabetes are lower, keep reading for the best answer.
Answer B is correct: 51% chose this answer, “The recommended time in range is >70% within 63–140 mg/dL; MT’s TIR is slightly below target and her time below and above range is above the recommended goal.” Answer B is correct. Based on the 2025 ADA Standards of Care the recommended time in range targets for individuals with type 1 diabetes during pregnancy is >70% between 63-140 mg/dL, < 4% under 63 mg/dL with < 1 % under 54 mg/dL, and < 25% over 140 mg/dL.
Answer C is incorrect: 19.55% chose this answer, “The recommended time in range is >80% within 63–140 mg/dL; MT’s TIR is below target, with fluctuations of hypo and hyperglycemia.” Answer C is incorrect. The time in range target is above the evidenced-based
minimum and MT is having frequent hypoglycemia in addition to hyperglycemia, both outside the goal ranges.
Answer D is incorrect: 12.87% chose this answer, “The recommended time in range is >80% within 70–180 mg/dL to prevent fetal
complications; MT’s TIR is significantly below the recommended Standard of Care target.” Answer D is incorrect. The recommended target range for individuals with type 1diabetes during pregnancy is 63-140 mg/dL as stated above.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
with Coach Beverly Thomassian RN, MPH, CDCES, BC-ADM
Course credits through AMA PRA Category 1 Credits™, ACPE, ANCC, and CDR!
This course is included in our Level 2 | Standards of Care Intensive
This Level 2 course fulfills the annual ADA Standards of Care component required for CDCES certification renewal. They also count toward your CDCES and BC-ADM certification CE requirements.
Join Coach Bev for an in-depth exploration of the 2026 ADA Standards! This is our most popular course of the year, offering the perfect opportunity to immerse yourself in the essential content featured in this comprehensive 300-page clinical guidebook.
This course, updated annually, is an essential review for anyone in the field of diabetes. Join Coach Beverly as she summarizes the annual updates to the American Diabetes Association’s (ADA) Standard of Medical Care in Diabetes. This course provides critical teaching points and content for healthcare professionals involved in diabetes care and education.
Topics:
Course Objectives:
Upon completion of this activity, participants will be able to: