
Subscribe
eNewsletter
Ready to get certified?
Free CDCES Coach App
eNewsletter
Free CDCES Coach App

For last week’s practice question, we quizzed participants on post-meal glucose spikes. 51% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question: TR can’t figure out why her BG always spikes after breakfast.
How many grams of carb is in the following breakfast? 2 corn tortillas, 2 fried eggs with salsa, ½ cup hashbrowns and an 8 ounce glass of milk.
Answer Choices:
If you are thinking about taking the certification exam, this practice test question will set you up for success. Test writers anticipate possible answers based on the details in the question. They will wave those “juicy answers” right under your nose. Your job is to weed through the particulars, pluck out the most important elements and choose the BEST answer.
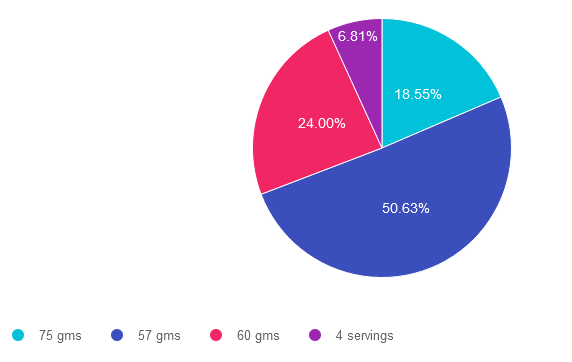
Answer 1 is incorrect. 18.55% chose this answer, “75 gms”. To answer this question accurately, it is important to be familiar with the common servings sizes of carbs and to know which foods don’t count as carbs. This answer is incorrect because it is an over estimate of carbs in this meal.
Answer 2 is correct. 50.63% of you chose this answer, “57 gms”. Yes, this is the BEST Answer. GREAT JOB. Here are the carbs broken down. 2 corn tortillas = 30gms carb, 2 fried eggs with salsa= 0 gms carb, ½ cup hashbrowns – 15 gms and an 8 ounce glass of milk =12gms. 30 + 15+ 12 = 57 gms of carbohydrate in this meal. An important fact to keep in mind for exam success; a cup of milk is 12 gms of carb, not 15gms.
Answer 3 is incorrect. About 24% of respondents chose this, “60 gms” This was the juicy answer. An important fact to keep in mind for exam success; a cup of milk is 12 gms of carb, not 15gms. Here are the carbs broken down. 2 corn tortillas = 30gms carb, 2 fried eggs with salsa= 0 gms carb, ½ cup hashbrowns – 15 gms and an 8 ounce glass of milk =12gms. 30 + 15+ 12 = 57 gms of carbohydrate in this meal.
Finally, Answer 4 is incorrect. 6.81% chose this answer, “4 servings” This answer is tempting, but the question asks “how many gms of carbohydrate” not, how many servings of carb. A great idea is to always eliminate answers that don’t match the unit of measure used in the question.
If you want more info on carb counting, you are invited to join our Virtual Conference in April. Save $100 through April 7, 2023 (see info below). We hope you appreciate this week’s rationale!
You are invited to join our Virtual Conference with our Nutrition expert speaker, Ashley LaBrier, MS, RD, CDCES, who will be providing a half-day presentation on this important topic!

Ashley LaBrier, MS, RD, CDES, is an innovator in the field of diabetes, nutrition, and technology. Ashley is a consultant and the Diabetes Education Program Coordinator at the Salinas Valley Medical Clinic’s Diabetes & Endocrine Center.
Ms. LaBrier is passionate about providing person-centered education to empower those who live with diabetes. Having been diagnosed with type 1 diabetes herself nearly 20 years ago, she combines her professional knowledge with personal experience and understanding.
Whether you are new to diabetes or a seasoned expert, you’ll benefit from this virtual conference with the latest research plus critical content that you can immediately apply to your clinical practice.
If you are seeking a state-of-the-art review of current diabetes care, this course is for you. Our team has been fine-tuning this course for over fifteen years, and we know what you need. This program can also be a great addition to your CDCES or BC-ADM exam study plan.
Group discounts are available!*
Download Course Flyer | Download Schedule
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
For last week’s practice question, we quizzed participants on their nutrition label reading ability. About 59% of respondents chose the best answer, revealing how challenging nutrition labels can be to dissect and understand, even for super-smart health care professionals. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question: You are teaching about counting fat.
If they ate 2 servings of this Macaroni and Cheese (see label), how many calories would come from total fat?
Answer Choices:

If you are thinking about taking the certification exam, this practice test question will set you up for success. Test writers anticipate possible answers based on the details in the question or image (like this nutrition label). They will wave those “juicy answers” right under your nose. Your job is to weed through the particulars, pluck out the most important elements and choose the BEST answer.
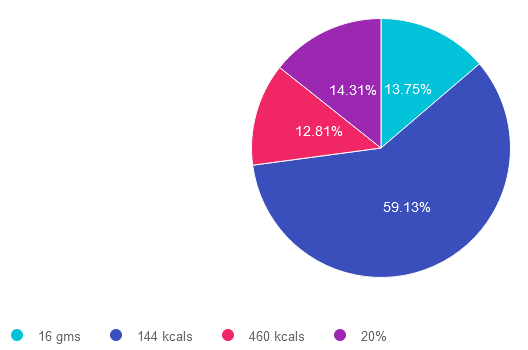
Answer 1 is incorrect. 13.75% chose this answer. “16 gms.” While it is true that there are 16 grams of fat in 2 servings of macaroni and cheese, this question doesn’t ask the test taker, “how many grams of fat”. The intent of the question is to determine how many kcals from total fat. Right away, we know this answer is wrong, because the unit is in gms not kcals.
Answer 2 is correct. 59.13% of you chose this answer. “144 kcals.” GREAT JOB. To get to this answer, you have to do a little math and know one important fact; there are 9 kcals in 1 gm of fat. On this label, one serving of macaroni and cheese has 8 gms, so 2 servings has 16 gms of total fat. 16 gms x 9 kcals = 144 kcals. In preparation for certification exams (and providing nutrition counseling), knowing how to read labels and being familiar with the kcals for protein, carbs and fats is very helpful.
Answer 3 is incorrect. About 12.81% of respondents chose this. “460 kcals.” This would be the correct answer if the question read, “how many total calories” is in 2 servings of this macaroni and cheese. However, the question is only asking for total fat calories in 2 servings. To get to best answer, you have to do a little math and know one important fact; there are 9 kcals in 1 gm of fat. On this label, one serving of macaroni and cheese has 8 gms, so 2 servings has 16 gms of total fat. 16 gms x 9 kcals = 144 kcals.
Finally, Answer 4 is incorrect. 14.31% chose this answer. “20%.” While it is true that there is 20% total fat in 2 servings of macaroni and cheese, this question doesn’t ask the test taker, “what percent of fat”. The intent of the question is to determine how many kcals from total fat. Right away, we know this answer is wrong, because the unit is in % not kcals.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
You are invited to join our Virtual Conference with our Nutrition expert speaker, Ashley LaBrier, MS, RD, CDCES, who will be providing a half-day presentation on this important topic!
Ashley LaBrier, MS, RD, CDES, is an innovator in the field of diabetes, nutrition, and technology. Ashley is a consultant and the Diabetes Education Program Coordinator at the Salinas Valley Medical Clinic’s Diabetes & Endocrine Center.
Ms. LaBrier is passionate about providing person-centered education to empower those who live with diabetes. Having been diagnosed with type 1 diabetes herself nearly 20 years ago, she combines her professional knowledge with personal experience and understanding.

Whether you are new to diabetes or a seasoned expert, you’ll benefit from this virtual conference with the latest research plus critical content that you can immediately apply to your clinical practice.
If you are seeking a state-of-the-art review of current diabetes care, this course is for you. Our team has been fine-tuning this course for over fifteen years, and we know what you need. This program can also be a great addition to your CDCES or BC-ADM exam study plan.
Group discounts are available!*
Download Course Flyer | Download Schedule
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
For last week’s practice question, we quizzed participants on if fast food is the best solution for food insecurity. 90% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question: Due to the increased cost of groceries, JR tells you all they can afford to eat are fast foods.
As a diabetes care and education specialist, what is the best response?
Answer Choices:
If you are thinking about taking the certification exam, this practice test question will set you up for success. Test writers anticipate possible answers based on the details in the question. They will wave those “juicy answers” right under your nose. Your job is to weed through the particulars, pluck out the most important elements and choose the BEST answer.
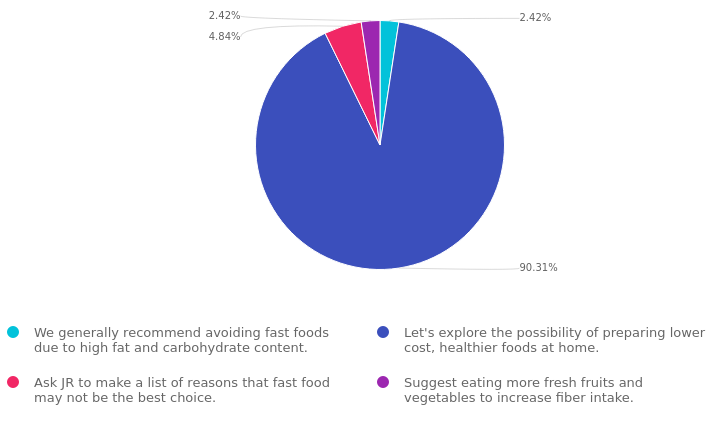
Answer 1 is incorrect. 2.42% chose this answer. “We generally recommend avoiding fast foods due to high fat and carbohydrate content.” While it is true that many fast food options are often high in fat and carbohydrates, we want to honor people choices and situations. This response might be received as critical and could limit the opportunity to collaborate on healthier approaches.
Answer 2 is correct. 90.31% of you chose this answer. “Let’s explore the possibility of preparing lower-cost, healthier foods at home.” GREAT JOB, most chose this BEST answer for good reason. This person-centered approach invites JR to explore lower cost foods that they can prepare at home. It honors JR’s concern over their limited income and invites collaborative problem solving.
Answer 3 is incorrect. 4.48% of respondents chose this. “Ask JR to make a list of reasons that fast food may not be the best choice.” As with the first answer, this response might be received as critical and could limit the opportunity to collaborate on healthier approaches.
Finally, Answer 4 is incorrect. 2.42% chose this answer. “Suggest eating more fresh fruits and vegetables to increase fiber intake.” This answer doesn’t really address the intent of the question and might limit the opportunity to collaborate on problem solving.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
You are invited to join our Virtual Conference with our Nutrition expert speaker, Ashley LaBrier, MS, RD, CDCES, who will be providing a half-day presentation on this important topic!
Ashley LaBrier, MS, RD, CDES, is an innovator in the field of diabetes, nutrition, and technology. Ashley is a consultant and the Diabetes Education Program Coordinator at the Salinas Valley Medical Clinic’s Diabetes & Endocrine Center.
Ms. LaBrier is passionate about providing person-centered education to empower those who live with diabetes. Having been diagnosed with type 1 diabetes herself nearly 20 years ago, she combines her professional knowledge with personal experience and understanding.
Whether you are new to diabetes or a seasoned expert, you’ll benefit from this virtual conference with the latest research plus critical content that you can immediately apply to your clinical practice.
If you are seeking a state-of-the-art review of current diabetes care, this course is for you. Our team has been fine-tuning this course for over fifteen years, and we know what you need. This program can also be a great addition to your CDCES or BC-ADM exam study plan.
Group discounts are available!*
Download Course Flyer | Download Schedule
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
For last week’s practice question, we quizzed participants on person-centered care. 62% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question: TR is a healthcare professional who provides diabetes care and education support. They are interested in providing more person-centered care to the individuals they serve.
Which of the following statements verifies they are on the right track?
Answer Choices:
If you are thinking about taking the certification exam, this practice test question will set you up for success. Test writers anticipate possible answers based on the details in the question. They will wave those “juicy answers” right under your nose. Your job is to weed through the particulars, pluck out the most important elements and choose the BEST answer.
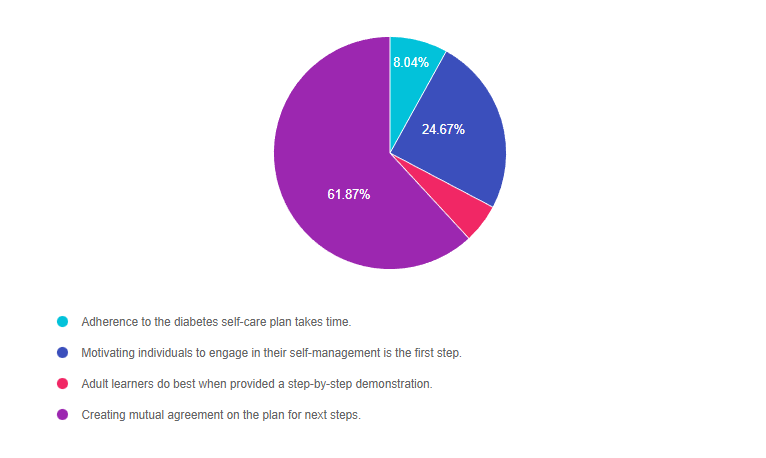
Answer 1 is incorrect. 8.04% chose this answer. “Adherence to the diabetes self-care plan takes time.” Under the umbrella of a person-centered care approach, the terms “adherence” and “compliance” are outdated concepts that are no longer used. For example, if we say that TR is adherent, it means that they are following the provider’s instructions instead of being an active participant in care. This person-centered approach engages the individual in the decision-making process and self-care plan.
Answer 2 is incorrect. 24.67% of you chose this answer. “Motivating individuals to engage in their self-management is the first step.” This is a juicy answer that sounds really good. However, it is not a realistic expectation to believe we can motivate people to make changes in their self-management. We can provide coaching and support, but ultimately, the person with diabetes needs to find their own motivation to make slow and steady behavior change. For this reason, this approach is not considered a person-centered approach.
Answer 3 is incorrect. 5.42% of respondents chose this. “Adult learners do best when provided a step-by the-step demonstration.” This answer is partially correct. Adult learners do apply their previous knowledge to the task at hand. However, more importantly than just observing, adult learners need to participate in the learning activity and have “hand’s on” practice to solidify their knowledge.
Finally, Answer 4 is correct. 61.87% chose this answer. “Creating mutual agreement on the plan for next steps.” YES, this is the BEST PERSON-CENTERED ANSWER. This approach invites the person with diabetes to fully participate in determining their needs and goals while making plans for the future in collaboration with the provider.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Your team is invited to our Virtual DiabetesEd™ Training Conference! Set your team apart and prepare for diabetes certification!
Join this state-of-the-art conference taught by content experts, Diana Isaacs, PharmD, BCPS, BCACP, BC-ADM, CDCES, Beverly Thomassian RN, MPH, CDCES, BC-ADM, and Ashley LaBrier who are passionate about improving diabetes care.
Group discounts are available!*
All hours earned count toward your CDCES Accreditation Information
Many of you have requested to set up payment plans for your orders and we have found a great solution for this! During checkout, on the payment page, you can now select “Shop Pay” to pay in 3 installments instead of just one payment.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparator
For last week’s practice question, we quizzed participants on prediabetes after GDM. It was a challenging question and 60% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question:
LR experienced gestational diabetes with their third pregnancy and now, at age 41, was just diagnosed with prediabetes. LR’s BMI is 29.3 and she is trying to lose weight.
Based on the 2023 ADA Standards of Care, in addition to providing LR with lifestyle coaching, what other intervention is recommended?
Answer Choices:
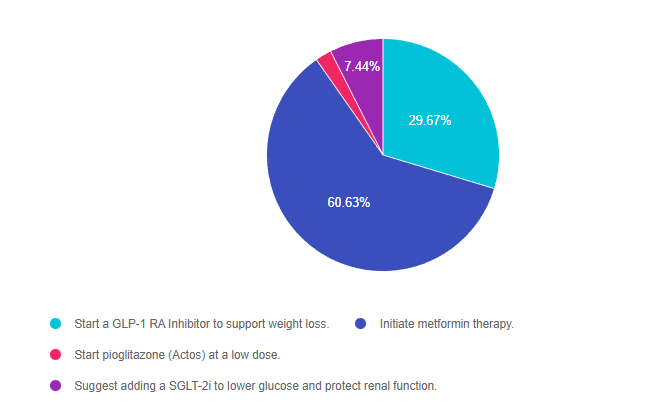
Answer 1 is incorrect. 29.67% chose this answer, “Start a GLP-1 RA Inhibitor to support weight loss.” Since LR has prediabetes, not diabetes, and her BMI is less than 30, GLP-1 RA therapy isn’t indicated. Plus, this recommendation isn’t included in the ADA standards (see below).
Answer 2 is correct. 60.63% of you chose this answer, “Initiate metformin therapy.” YES, this is the BEST answer. GREAT JOB! For people with a history of GDM who now express prediabetes, they have a very high risk of getting diabetes in the near future. In addition to referring to a Diabetes Prevention Program, the Standards recommend initiation of metformin therapy to delay the onset of diabetes.
Answer 3 is incorrect. 2.27% of respondents chose this answer, “Start pioglitazone (Actos) at a low dose” Although low dose pioglitazone is recommended for those with prediabetes or diabetes and a history of stroke, LR has no history of stroke. In addition, pioglitazone is associated with weight gain and is not recommended in the ADA Standards to treat prediabetes.
Finally, Answer 4 is incorrect. 7.44% chose this answer, “Suggest adding a SGLT-2i to lower glucose and protect renal function.” Since LR has prediabetes, not diabetes and no signs of kidney problems, SGLT-2i therapy isn’t indicated. Plus, this recommendation isn’t included in the ADA standards (see below).
Thank you so much for reading this “Rationale of the Week”. For more information on this topic, we also invite you to join our Online Courses and Virtual DiabetesEd Training Program.
For last week’s practice question, we quizzed participants on the new ADA Standards for lipid management. It was a complicated question and 43% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question:
JR is 67 with type 1 diabetes and was discharged a few months ago after receiving a coronary artery bypass. JR is on insulin pump therapy and a CGM, with a recent A1C of 6.7%. Their blood pressure is 129/78.
Other recent labs include:
JR’s medications include: insulin, atorvastatin 80mg, atenolol 50mg, and aspirin therapy. JR has met with the dietitian and is trying to eat healthfully. They have lost 5 pounds over the past few months.
Based on the 2023 ADA Standards of Care and JR’s history, which of the following is considered best practice?
Answer Choices:
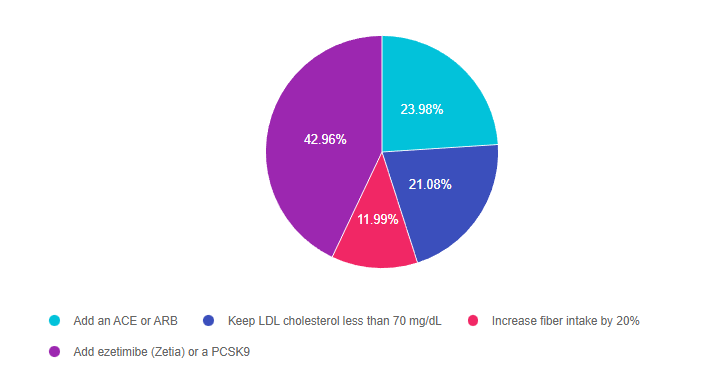
Answer 1 is incorrect. 23.93% chose this answer, “Add an ACE or ARB.” This was a juicy answer. However, since the B/P is on target at less than 130/80 and JR does not have an elevated UACR, adding an ACE or ARB is not indicated at this time.
Answer 2 is incorrect. 21.08% of you chose this answer, “Keep LDL cholesterol less than 70 mg/dL.” Since JR has ASCVD, as evidenced by their need for a coronary artery bypass, the LDL target is less than 55 mg/dL. This new intensified LDL target is based on the 2023 updated guidelines. Read our blog on New Lipid Guidelines here.
Answer 3 is incorrect. 11.99% of respondents chose this answer, “Increase fiber intake by 20%.” While increasing fiber intake is always a good idea, in may not be enough to help JR get their LDL to a target level of less than 55 mg/dl.
Finally, Answer 4 is correct. 42.96% chose this answer, “Add ezetimibe (Zetia) or a PCSK9.” Yes, this is the best answer, GREAT JOB. Since JR has ASCVD, as evidenced by their need for a coronary artery bypass, the LDL target is less than 55 mg/dL. Since they are already on max dose of atorvastatin at 80mg, the ADA Guidelines recommend adding an additional agent, either ezetimibe (Zetia) or a PCSK9 to further lower the LDL to reach a target of less than 55 mg/dL. Download Lipid Medication Cheat Sheet Here
Thank you so much for reading this “Rationale of the Week”. For more information on this topic, we encourage you to Read our blog on New Lipid Guidelines and Download Lipid Medication Cheat Sheet Here. We also invite you to join our Online Courses and Virtual DiabetesEd Training Program.
Whether you are new to diabetes or a seasoned expert, you’ll benefit from this virtual conference with the latest research plus critical content that you can immediately apply to your clinical practice.
If you are seeking a state-of-the-art review of current diabetes care, this course is for you. Our team has been fine-tuning this course for over fifteen years, and we know what you need. This program can also be a great addition to your CDCES or BC-ADM exam study plan.
Group discounts are available!*
Download Course Flyer | Download Schedule
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
For last week’s practice question, we quizzed participants on low blood sugars and beer. 38% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question:
JL is 19 and has type 1 diabetes, drinks a “few beers” on the weekends with their college friends. JL uses an insulin pump, but mostly relies of fingerstick checks to monitor blood sugars. According to their log, JL experienced a few low blood glucose levels the past weekend of 62, 49, and 51.
Based on the ADA Standards, what is the most important recommendation for JL?
Answer Choices:
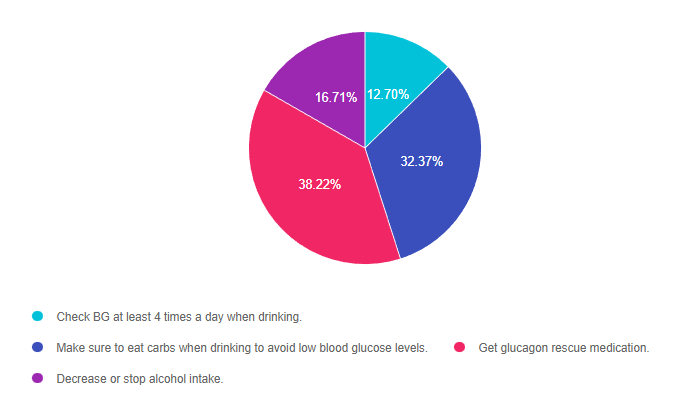
Answer 1 is incorrect. 12.70% chose this answer, “Check BG at least 4 times a day when drinking.” This is a juicy answer. Although monitoring will help JL detect low blood sugars, it doesn’t necessarily translate into taking action to prevent or treat these frequent bouts of level 2 hypoglycemia.
Answer 2 is incorrect. 32.37% of you chose this answer, “Make sure to eat carbs when drinking to avoid low blood glucose levels.” This is another juicy answer and a solid recommendation. For people with type 1 who experience hypoglycemia when drinking alcohol, eating 15gms of carb along with each alcohol serving can help maintain glucose levels. However, this answer is not based on the ADA Standards of Care.
Answer 3 is correct. 38.22% of respondents chose this answer, “Get glucagon rescue medication.” This is the BEST answer. According to the ADA’s Standard 6 on Glycemic Targets, “6.12 Glucagon should be prescribed for all individuals at increased risk of level 2 or 3 hypoglycemia, so that it is available should it be needed”. JL is experiencing Level 2 hypoglycemia with glucose levels dropping to 49 and 51. (see image from Glucagon PocketCard to right for Hypo Levels). While prevention of hypoglycemia is the long term goal, in the short term we need to make sure JL has access to a glucagon rescue med and that their significant others are trained on how to administer this life saving glucose booster.
Finally, Answer 4 is incorrect. 16.71% chose this answer, “Decrease or stop alcohol intake.” While we might want to have a conversation about alcohol and safety, the ADA Standards allow for 1 alcohol serving a day for women and 2 alcohol servings a day for men. In this situation, we might want to discuss adjusting insulin dosing and carbohydrate intake to prevent future bouts of hypoglycemia. However, for safety sake, JL will need a glucagon rescue med prescribed in case of a severe low blood glucose.
Thank you so much for reading this “Rationale of the Week”. For more information on this topic, we encourage you to join our Online Courses and Virtual DiabetesEd Training Program.

Can’t join all the sessions live? No problem. Your registration guarantees you access to the recorded lectures for a full year.
This bundle is specifically designed for healthcare professionals who are studying for the Board Certified in Advanced Diabetes Management (BC-ADM) or the Certified Diabetes Care and Education Specialist (CDCES) certification exam.
Intended Audience: This library of critical information is designed for individuals or groups of diabetes specialists, including RNs, RDs, Pharmacists, Nurse Practitioners, Clinical Nurse Specialists, Physician Assistants, and other health care providers interested in staying up to date on current practices of care for people with diabetes and preparing for the BC-ADM or the CDCES certification Exam.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
For last week’s practice question, we quizzed participants on the best action for a safe surgery. 51% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question:
PZ is having elective surgery in the morning. Diabetes medications include 20 units glargine (Semglee) at hs, metformin BID and empagliflozin (Jardiance).
According to 2023 ADA Standards, what are the best actions for a safe surgery?
Answer Choices:
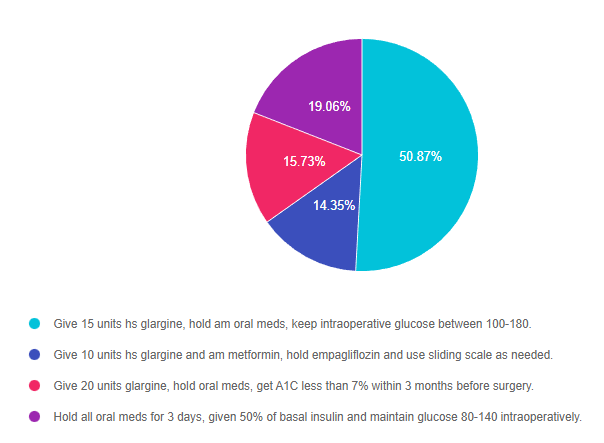
Answer 1 is correct. 50.87% chose this answer, “Give 15 units hs glargine, hold am oral meds, keep intraoperative glucose between 100-180.” YES, GREAT JOB! The ADA Standard 16 on Hospitalization has been updated with new perioperative glucose goals and preop medication adjustments. To prevent intraoperative hypoglycemia, the glucose goal was increased to 100-180. In addition, they recommend reducing basal insulin by 20-25% the night before surgery and holding all oral meds the morning of surgery. SGLT-2s are held for 3-4 days before surgery to decrease risk of DKA in the perioperative period. In this vignette, we reduced PZ’s basal insulin from 20 units to 15 units (25% decrease) and held all oral meds the morning of surgery. In addition, the 2023 Standards recommend achieving an A1C less than 8% before elective surgeries. Since about 20% of people undergoing surgery have diabetes, these guidelines are super helpful and important to improve post surgical outcomes.
Answer 2 is incorrect. 14.35% of you chose this answer, “Give 10 units hs glargine and am metformin, hold empagliflozin and use sliding scale as needed.” This is answer is close and partly correct, because it recommends holding the oral medications. However, the first part of the answer is incorrect since a basal insulin reduction of 50% is too aggressive. People release lots of counterregulatory hormones during surgery, so they still need at least 75% of their usual basal insulin dose to prevent intraoperative hyperglycemia. If the person uses NPH basal insulin, they would need to reduce the evening dose by 50%. Since about 20% of people undergoing surgery have diabetes, these guidelines are super helpful and important to improve post surgical outcomes.
Answer 3 is incorrect. 15.73% of respondents chose this answer, “Give 20 units glargine, hold oral meds, get A1C less than 7% within 3 months before surgery.” This is answer is close and partly correct, because it recommends holding the oral medications. However, the first part of the answer is incorrect since the basal insulin needs to be reduced by 20-25% to prevent intraoperative hypoglycemia. In addition, the 2023 Standards recommend achieving an A1C less than 8% (not 7%) before elective surgeries. Since about 20% of people undergoing surgery have diabetes, these guidelines are super helpful and important to improve post surgical outcomes.
Finally, Answer 4 is incorrect. 19.06% chose this answer, “Hold all oral meds for 3 days, given 50% of basal insulin and maintain glucose 80-140 intraoperatively.” This entire answer is incorrect for the following reasons. Oral meds are held the day of surgery, except for SGLT2i’s, which are held for 3-4 days pre-op. As far as basal insulin, the ADA guidelines recommend giving 75-80% of usual dose, except for NPH insulin, which is reduced by 50%. Lastly, the intraoperative glucose target is 100 -180. Since about 20% of people undergoing surgery have diabetes, these guidelines are super helpful and important to improve post surgical outcomes.
Thank you so much for reading this “Rationale of the Week”.
We invite you to join Coach Beverly on May 30, 2023 – Hospital and Hyperglycemia 1.5 CEs
This course, updated annually, is an essential review for anyone in the field of diabetes. Join Coach Beverly as she summarizes the 2023 updates to the American Diabetes Association’s Standards of Medical Care in Diabetes and provides critical teaching points and content for healthcare professionals involved in diabetes care and education.
Objectives:
Intended Audience: This course is a knowledge-based activity designed for individuals or groups of diabetes professionals, including RNs, RDs, Pharmacists, Nurse Practitioners, Clinical Nurse Specialists, Physician Assistants, and other health care providers interested in staying up to date on current practices of care for people with prediabetes, diabetes, and other related conditions.
Don’t worry if you can’t make it live. Your registration guarantees access to the recorded version in the Online University.
All hours earned count toward your CDCES Accreditation Information
Can’t join all the sessions live? No problem. Your registration guarantees you access to the recorded lectures for a full year.
This bundle is specifically designed for healthcare professionals who are studying for the Board Certified in Advanced Diabetes Management (BC-ADM) or the Certified Diabetes Care and Education Specialist (CDCES) certification exam.
Intended Audience: This library of critical information is designed for individuals or groups of diabetes specialists, including RNs, RDs, Pharmacists, Nurse Practitioners, Clinical Nurse Specialists, Physician Assistants, and other health care providers interested in staying up to date on current practices of care for people with diabetes and preparing for the BC-ADM or the CDCES certification Exam.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.