
Subscribe
eNewsletter
Ready to get certified?
Free CDCES Coach App
eNewsletter
Free CDCES Coach App

Our September 7th Question of the week quizzed test takers on carb counting. 55% of respondents chose the correct answer. This was a hard question. Figuring out how much insulin to cover carbs is an important topic to review, so we can pass on correct info to people living with diabetes.
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer below: Answer Question
Question: LS uses an insulin pump and CGM. Most recent report reveals LS is running 56% time in range and 44% above target range. LS asks for help with carb counting. A typical breakfast includes: ½ cup of milk, 2 tablespoons peanut butter and 1 piece whole grain bread, 3 oz’s of grapes and one cup of black coffee with Splenda. LS’s insulin to carb ratio for breakfast is 1:12, for lunch and dinner is 1:15.
Based on this, how much insulin does LS need for breakfast?
Answer Choices:
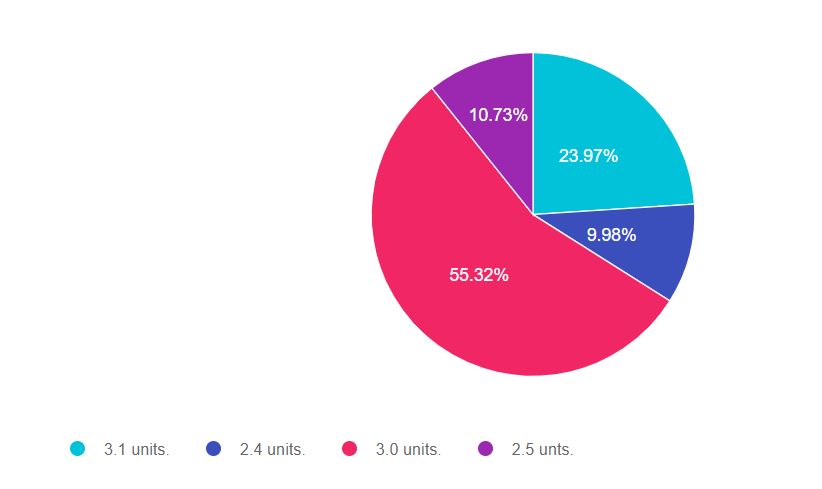
As shown above, the most common choice was option 3, the second most common answer was option 1, then option 4, and finally option 2.
If you are thinking about taking the certification exam, this practice test question will set you up for success. Test writers anticipate possible answers based on the details in the question. They will wave those “juicy answers” right under your nose. Your job is to weed through the particulars, do careful math, be familiar with the exchange list and choose the BEST answer.
Diabetes Exchange List – a brief summary of serving size and carbohydrate counts for common foods. Excellent study tool for the exam.
Here are the carb counts of the foods listed:
LS’s insulin to carb ratio:
Answer 1 is incorrect. 23.97% chose this answer, “3.1 units.” If you chose this answer you are so close. For the exam, remember that one cup of milk has 12gms of carbohydrate (not 15gms). Please see the link to the exchange list for the carb counts of common foods.
Answer 2 is incorrect. 9.98% of you chose this answer, “2.4 units.” If you chose this answer, you may have used the lunch/dinner insulin to carb ratio of 1:15 instead of the breakfast ratio of 1:12. This is an easy mistake to make, so make sure to read the question carefully and take your time doing the math. You got this.
Answer 3 is correct. 55.32% of respondents chose this answer, “3.0 units.” GREAT JOB. This is the best answer. The total carb intake for LS is 36 gms. Since the Insulin to Carb (I:CR) ratio for breakfast is 1:12, to find out how much insulin LS needs for breakfast, just divide gms of carb by the I:CR or 36 / 12 = 3 units.
Finally, Answer 4 is incorrect. 10.73% chose this answer, “2.5 units.” If you chose this answer. there are 2 things to be aware of: one cup of milk has 12gms of carbohydrate (not 15gms) and you may have used the lunch/dinner insulin to carb ratio of 1:15 instead of the breakfast ratio of 1:12. These are easy mistakes to make, so make sure to read the question carefully, be familiar with common carbs and take your time doing the math. You got this.
Diabetes Exchange List a brief summary of serving size and carbohydrate counts for common foods. Excellent study tool for the exam.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Want to learn more about carb counting and more?
We address this topic from many different angles during our Virtual Course!
Did you miss the live conference? No worries! You can register now to watch on-demand
Whether you are new to diabetes or a seasoned expert, you’ll benefit from this virtual conference with the latest research plus critical content that you can immediately apply to your clinical practice.
If you are seeking a state-of-the-art review of current diabetes care, this course is for you. Our team has been fine-tuning this course for over fifteen years, and we know what you need. This program can also be a great addition to your CDCES or BC-ADM exam study plan.
Team of expert faculty includes:
In addition to informative lectures, we also use group activities and case studies to highlight the essential knowledge, skills, and strategies needed to succeed in diabetes education today!

CEs: Includes over 30 CEs
Program Info: 2021 Diabetes Educator Course Flyer & Schedule (subject to change)
Speakers: View Conference Faculty.
Dates: Your registration fee includes access to FREE podcast and all recorded webinars for one year.
Two Registration Options
Virtual DiabetesEd Specialist Conference Deluxe | Oct. 6-8 | 30+ CEs
Deluxe Virtual Program for $459 includes:
+Plus Syllabus, Standards and Swag:
2021 Diabetes Educator Course Flyer & Schedule (subject to change)
Virtual DiabetesEd Specialist Conference Basic | Oct. 6-8 | 30+ CEs
Basic virtual program for $359 includes:
2021 Diabetes Educator Course Flyer & Schedule (subject to change)
Team of Experts: Our team of expert faculty has been fine-tuning this course for over fifteen years and we know what you need to succeed! In addition to informative lectures, we also use group activities and case studies to highlight the essential knowledge, skills, and strategies needed to succeed in diabetes education today!
When you register for our Virtual Course, you have immediate access to these Bonus DiabetesEd University Online Courses – for FREE!
2021 Diabetes Educator Course Flyer & Schedule (subject to change)
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]
Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
Our August 31st Question of the week quizzed test takers on interventions. Over 90% of respondents chose the correct answer. Great job! We thought that this was an important topic to review, so we can pass on correct info to people living with diabetes.
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer below: Answer Question
Question: JR is 43 with type 2 diabetes who shows up for their usual visit and happens to mention that they have had moments of feeling dizzy over the past few months. A few times, they have checked their blood sugars during these spells, and they were 121 and 136. JRs medications include glipizide 10mg BID, metformin 1000mg BID, lisinopril 20mg, atorvastatin 20mg. JR has lost about 10 lbs since their last visit by eating more whole foods and grains and less fast foods.
Based on this assessment, what is the next best action?
Answer Choices:
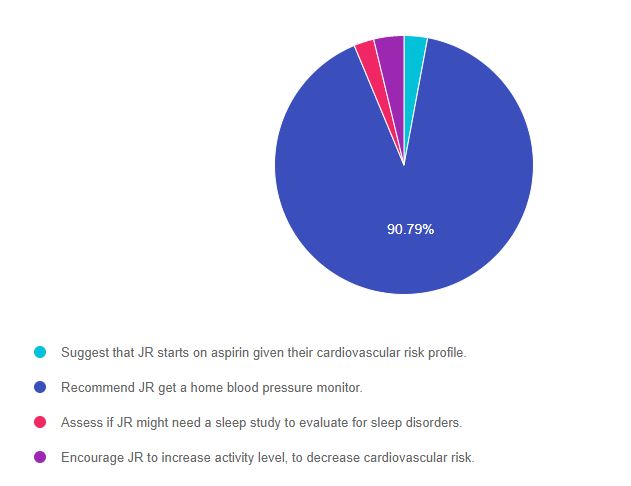
As shown above, the most common choice was option 3, the second most common answer was option 1, then option 2, and finally option 4.
If you are thinking about taking the certification exam, this practice test question will set you up for success. Test writers anticipate possible answers based on the details in the question. They will wave those “juicy answers” right under your nose. Your job is to weed through the particulars, pluck out the most important elements and choose the BEST answer.
Answer 1 is incorrect. 2.93% chose this answer, “Suggest that JR starts on aspirin given their cardiovascular risk profile.” Aspirin therapy is recommended for those 50 and older with existing or at risk for a cardiovascular event. Since JR is younger than 50, this is not the best answer.
Answer 2 is correct. 90.79% of you chose this answer, “Recommend JR get a home blood pressure monitor.” Yes, GREAT JOB. Most of you chose this best answer. Most likely, the dizziness is a result of lower blood pressure secondary to weight loss and treatment with an ACE Inhibitor (lisinopril). The ADA Standards recommend that people on blood pressure medications self-monitor their blood pressure at home to detect changes in pressure that warrant a reduction or intensification of anti-hypertensive therapy.
Answer 3 is incorrect. 2.51% of respondents chose this answer, “Assess if JR might need a sleep study to evaluate for sleep disorders.” While it is true that many people with diabetes have sleep disorders, in this case study there is not enough supporting clinical symptoms to support a sleep study. For example if JR was complaining of waking up tired or waking up gasping for air, plus they exhibit other risk factors, then further sleep evaluation might be warranted.
Finally, Answer 4 is incorrect. 3.77% chose this answer, “Encourage JR to increase activity level, to decrease cardiovascular risk.” Encouraging activity to improve health is an important part of self-care coaching. However, in this case, since JR is complaining of “dizziness”, for safety, we might even back off a little from recommending activity until we determine the cause of JRs dizziness.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Want to learn more about this topic and more?
Did you miss the live conference? No worries! You can register now to watch on-demand
Whether you are new to diabetes or a seasoned expert, you’ll benefit from this virtual conference with the latest research plus critical content that you can immediately apply to your clinical practice.
If you are seeking a state-of-the-art review of current diabetes care, this course is for you. Our team has been fine-tuning this course for over fifteen years, and we know what you need. This program can also be a great addition to your CDCES or BC-ADM exam study plan.
Team of expert faculty includes:
In addition to informative lectures, we also use group activities and case studies to highlight the essential knowledge, skills, and strategies needed to succeed in diabetes education today!
CEs: Includes over 30 CEs
Program Info: 2021 Diabetes Educator Course Flyer & Schedule (subject to change)
Speakers: View Conference Faculty.
Dates: Your registration fee includes access to FREE podcast and all recorded webinars for one year.
Two Registration Options
Virtual DiabetesEd Specialist Conference Deluxe | Oct. 6-8 | 30+ CEs
Deluxe Virtual Program for $459 includes:
+Plus Syllabus, Standards and Swag:
2021 Diabetes Educator Course Flyer & Schedule (subject to change)
Virtual DiabetesEd Specialist Conference Basic | Oct. 6-8 | 30+ CEs
Basic virtual program for $359 includes:
2021 Diabetes Educator Course Flyer & Schedule (subject to change)
Team of Experts: Our team of expert faculty has been fine-tuning this course for over fifteen years and we know what you need to succeed! In addition to informative lectures, we also use group activities and case studies to highlight the essential knowledge, skills, and strategies needed to succeed in diabetes education today!
When you register for our Virtual Course, you have immediate access to these Bonus DiabetesEd University Online Courses – for FREE!
2021 Diabetes Educator Course Flyer & Schedule (subject to change)
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]
Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
Our August 24th Question of the week quizzed test takers on thick calluses coupled with leg pain. 61% of respondents chose the correct answer. We thought that this was an important topic to discuss further, so we can pass on correct info to people living with diabetes.
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer below: Answer Question
Question: JR has lived with type 1 diabetes for over twenty years. JR arrived in the clinic with thick calluses on both feet and complaints of calf pain when walking for more than 10 minutes. JR’s pulses are difficult to palpate.
What diagnosis best matches JR’s presentation?
Answer Choices:
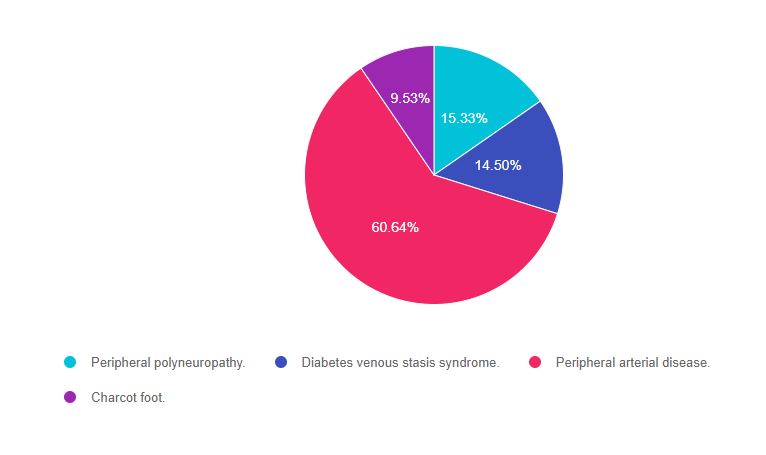
As shown above, the most common choice was option 3, the second most common answer was option 1, then option 2, and finally option 4.
If you are thinking about taking the certification exam, this practice test question will set you up for success. Test writers anticipate possible answers based on the details in the question. They will wave those “juicy answers” right under your nose. Your job is to weed through the particulars, pluck out the most important elements and choose the BEST answer. If you want to learn more about lower extremities, we invite you to join our Virtual Course or check out our Level 2 Online Courses.
Answer 1 is incorrect. 15.33% chose this answer, “Peripheral polyneuropathy.” This juicy answer is tempting, however it does not match the symptoms detailed by JR. A person with peripheral polyneuropathy will typically complain of numbness, tingling and leg pain at night. They may also have thick calluses. However, there are two clues that indicate a mismatch between question and answer. JR is “complaining of calf pain when walking for more than 10 minutes with difficulty locating pulses.” These chief complaints indicate a different pathology. Keep reading to find out more.
Answer 2 is incorrect. 14.50% of you chose this answer, “Diabetes venous stasis syndrome.” This is another juicy answer with a made up condition that is designed to sound familiar. In general, with venous disease, pulses are still palpable since there is adequate blood flow to lower extremities. There are two clues that indicate a mismatch between question and answer. “JR is complaining of calf pain when walking for more than 10 minutes with difficulty locating pulses.” These chief complaints indicate a different pathology. Keep reading to find out more.
Answer 3 is correct. 60.64% of respondents chose this answer, “Peripheral arterial disease.” YES, this is the BEST answer. Great job. JR is exhibiting the classic signs of inadequate arterial blood flow to the lower extremities, or peripheral arterial disease. JR’s complaints of “calf pain when walking for more than 10 minutes with difficulty locating pulses” indicate poor arterial circulation and warrant referral to a provider for complete CV risk assessment.
Finally, Answer 4 is incorrect. 9.53% chose this answer, “Charcot foot.” This answer is tempting. Charcot foot is characterized by severe foot inflammation and structural collapse. Since JR is “complaining of calf pain when walking for more than 10 minutes with difficulty locating pulses”, these symptoms do not match the usual complaints associated with Charcot foot. Good try, see answer 3 for more info.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Want to learn more about this topic and more?
Did you miss the live conference? No worries! You can register now to watch on-demand
Whether you are new to diabetes or a seasoned expert, you’ll benefit from this virtual conference with the latest research plus critical content that you can immediately apply to your clinical practice.
If you are seeking a state-of-the-art review of current diabetes care, this course is for you. Our team has been fine-tuning this course for over fifteen years, and we know what you need. This program can also be a great addition to your CDCES or BC-ADM exam study plan.
Team of expert faculty includes:
In addition to informative lectures, we also use group activities and case studies to highlight the essential knowledge, skills, and strategies needed to succeed in diabetes education today!
CEs: Includes over 30 CEs
Program Info: 2021 Diabetes Educator Course Flyer & Schedule (subject to change)
Speakers: View Conference Faculty.
Dates: Your registration fee includes access to FREE podcast and all recorded webinars for one year.
Two Registration Options
Virtual DiabetesEd Specialist Conference Deluxe | Oct. 6-8 | 30+ CEs
Deluxe Virtual Program for $459 includes:
+Plus Syllabus, Standards and Swag:
2021 Diabetes Educator Course Flyer & Schedule (subject to change)
Virtual DiabetesEd Specialist Conference Basic | Oct. 6-8 | 30+ CEs
Basic virtual program for $359 includes:
2021 Diabetes Educator Course Flyer & Schedule (subject to change)
Team of Experts: Our team of expert faculty has been fine-tuning this course for over fifteen years and we know what you need to succeed! In addition to informative lectures, we also use group activities and case studies to highlight the essential knowledge, skills, and strategies needed to succeed in diabetes education today!
When you register for our Virtual Course, you have immediate access to these Bonus DiabetesEd University Online Courses – for FREE!
2021 Diabetes Educator Course Flyer & Schedule (subject to change)
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]
Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
For our August 17th Question of the Week, 39% of respondents chose the best answer. This is due in part to our error. We mis-keyed the best answer for the first 96 respondents (we quickly fixed it as soon as we discovered the error). So, you may want to retake this question before you read on to discover the answer. Coach Bev sincerely apologizes if this caused any of you distress! But today, we are making it right. Thanks for your patience and ongoing participation!
Before we start, if you don’t want any spoilers and you tried the question on Tuesday morning, you can answer below: Answer Question
Question 1: Which of the following are considered diabetes autonomic neuropathies?
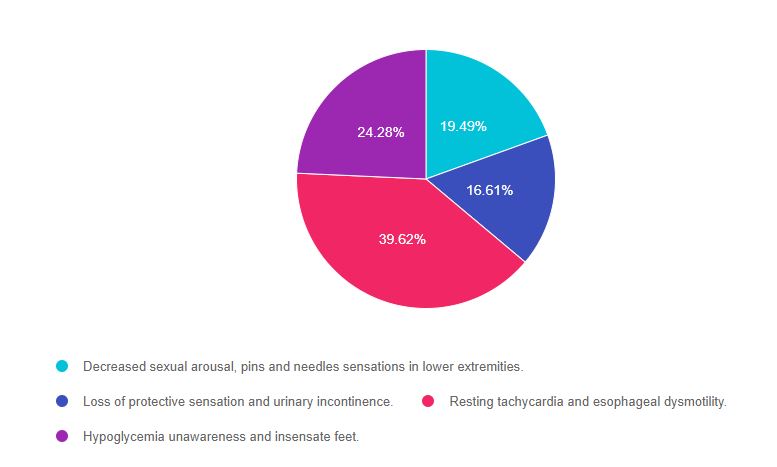
As shown above, the most common choice was option 3, the second most common answer was option 4, then option 1, and finally option 2.
If you are thinking about taking the certification exam, the content of this practice test question will set you up for success. Don’t forget to leverage your common sense and vast health care knowledge to get the best answer for specialty topics like microvascular disease. Be familiar with nerve disease presentation and screening as listed in the ADA Standards of Care on Microvascular health and treatment options. We also invite you to join our webinar (see below). Also, the tests will often provide a 2 part answer, one part being correct and the other part incorrect. Of course, if any part of the answer is incorrect, it is not the best answer. A great test taking tip to hold onto to when your sympathetic nervous system is in full gear. You got this, Coach Beverly
A note on Autonomic Neuropathy. This condition causes nerve damage to the autonomic nervous system which is in charge of digestion, sexual function, heart rate, and the adrenergic flight or fight response. The autonomic nervous system also “oversees” the energy-conserving parasympathetic response including bladder control, heart rate slowing, eye pupil constriction, and more.
Answer 1 is incorrect, 19.49% chose this answer, “Decreased sexual arousal, pins and needles sensations in lower extremities.” This is a juicy answer. Autonomic dysfunction can affect sexual function, but it doesn’t affect libido or sexual desire. In addition, the pins and needles sensation is due to the nerve damage associated with peripheral neuropathy. Since both parts of this answer aren’t correct, this answer is false.
Answer 2 is incorrect, 16.61% of you chose this answer, “Loss of protective sensation and urinary incontinence.” Loss of protective sensation is associated with peripheral neuropathy. However, urinary incontinence is often a result of autonomic neuropathy. Since both parts of this answer aren’t correct, this answer is false.
Answer 3 is correct, 39.62% of you chose this answer, GREAT JOB! “Resting tachycardia and esophageal dysmotility.” Elevated heart rate while resting is a concerning sign and is often associated with cardiac autonomic neuropathy and increased risk of a cardiac event. Autonomic neuropathy can affect the motility of the entire GI track, including the esophagus. The more commonly recognized GI autonomic neuropathy is gastroparesis. Since both conditions, resting tachycardia and esophageal dysmotility, are associated with autonomic neuropathy, this is the best answer.
Answer 4 is incorrect, 24.28% of you chose this juicy answer “Hypoglycemia unawareness and insensate feet.” Since hypoglycemia unawareness is associated with a diminished adrenergic response to low blood glucose levels, it is considered an autonomic neuropathy. However, insensate feet are due to peripheral nerve damage associated with ongoing hyperglycemia. Since both parts aren’t correct, this answer is false.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Want to learn more about this topic?
Join us for our
This course provides you with the need-to-know information regarding the microvascular complications of diabetes. We start with a brief overview of the pathophysiology and clinical manifestations then sum up with prevention strategies and screening guidelines. This straight-forward program will provide you with information you can use in your clinical setting and also provides critical content for the diabetes educator exam.
Objectives:
Can’t make it live? All paid registrants are guaranteed access to the video presentation, handouts and podcasts.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]
Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
For our August 10th Question of the Week, 37% of respondents chose the best answer. We want to “take a closer look” at this question and determine strategies to choose the best response.
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer below: Answer Question
Question 1: AL is 24 with newly diagnosed type 1 diabetes. AL is very worried about going blind because an Aunt with Type 1 diabetes lost her vision due to living with type 1 diabetes.
Which of the following matches the ADA guidelines for diabetes eye care?
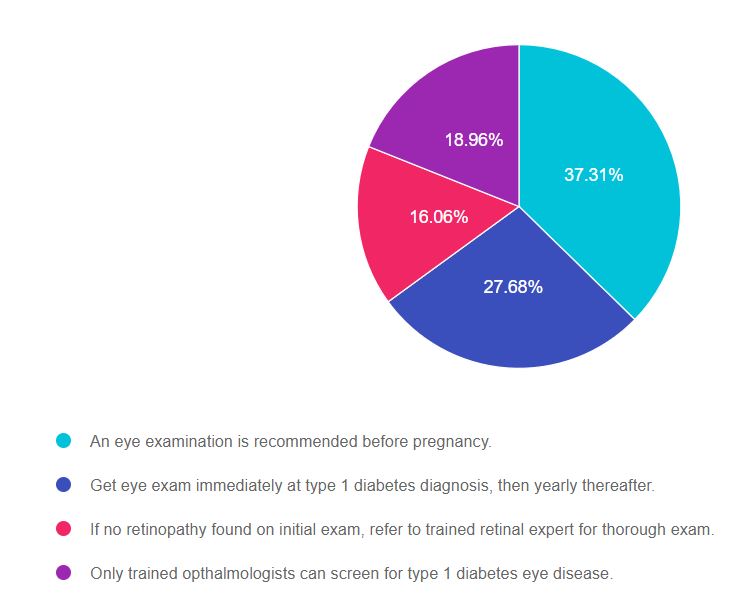
As shown above, the most common choice was option 1, the second most common answer was option 2, then option 4, and finally option 3.
If you are thinking about taking the certification exam, the content of this practice test question will set you up for success. Don’t forget to leverage your common sense and vast health care knowledge to get the best answer for specialty topics like microvascular disease. Be familiar with screening guidelines for eye disease as listed in the ADA Standards of Care on Microvascular health and treatment options. We also invite you to join our webinar (see below). You got this, Coach Beverly
Answer 1 is correct, 37.31% chose this answer, “An eye examination is recommended before pregnancy.” Great Job! Yes, this is the best answer. All people living with diabetes considering pregnancy need to get a baseline eye exam to evaluate retinal health. In addition, the ADA Standards recommend eye exams each trimester of pregnancy and after birth to monitor retinal changes.
Answer 2 is incorrect, 27.68% of you chose this answer, “Get eye exam immediately at type 1 diabetes diagnosis, then yearly thereafter.” This is the juicy answer. According to the ADA Standards for people with type 1 diabetes, they need an eye exam within in 5 years of diagnosis, then an eye exam every 1-2 years. The reason they don’t require an immediate eye exam is because type 1 diabetes is quickly identified and this short span of hyperglycemia does not increase risk of retinopathy. The reason we check people with type 2 eyes immediately, is because they could have had diabetes for an average of 6 years before diagnosis, allowing for the possibility of undetected eye damage.
Answer 3 is incorrect, 16.06% of you chose this answer, “If no retinopathy found on initial exam, refer to trained retinal expert for thorough exam.” ‘All people with diabetes do not need to be referred to a retinal expert. An ophthalmologist or optometrist can screen for type 1 diabetes eye disease. If retinopathy is discovered, depending on the severity, they may advise referral to a retinal specialist as needed.
Answer 4 is incorrect, 18.96% of you chose this answer “Only a trained ophthalmologists can screen for type 1 diabetes eye disease.” An ophthalmologist or optometrist can screen for type 1 diabetes eye disease. Programs that use retinal photography (with remote reading or use of a validated assessment tool) are also appropriate screening strategies for diabetes retinopathy. Such programs need to provide pathways for timely referral for a comprehensive eye examination when indicated.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Want to learn more about this topic?
Join us for our
This course provides you with the need-to-know information regarding the microvascular complications of diabetes. We start with a brief overview of the pathophysiology and clinical manifestations then sum up with prevention strategies and screening guidelines. This straight-forward program will provide you with information you can use in your clinical setting and also provides critical content for the diabetes educator exam.
Objectives:
Level 2 | Setting up a Successful DSME Program Standards | 1.5 CEs

This course provides you with a succinct overview of the latest standards for Diabetes Self-Management Education (DSME) and Support Programs. If you are taking the CDCES Exam or considering setting up a DSME program, this program is designed for you. We review the 10 standards and provide strategies on implementation. In addition, we discuss Medicare Reimbursement and covered benefits. This course provides insights into the exam philosophy and also highlights critical content areas.
Objectives:
Can’t make it live? All paid registrants are guaranteed access to the video presentation, handouts and podcasts.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]
Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
For our August 3rd Question of the Week, 53% of respondents chose the best answer. We want to “take a closer look” at this question and determine strategies to choose the best response.
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer below: Answer Question
Question 1: JR is 53 years old with type 2 diabetes for the past 7 years. JR’s BMI is 32, GFR is more than 60, blood pressure is 128/76, Urinary Albumin Creatinine Ratio (UACR) is 17mg/g.
According to the ADA Standards, which of the following is the most accurate recommendation to continue to protect JR’s kidney function?
Answer Choices:
As shown above, the most common choice was option 2, the second most common answer was option 3, then option 4, and finally option 1.
If you are thinking about taking the certification exam, the content of this practice test question will set you up for success. Don’t forget to leverage your common sense and vast health care knowledge to get the best answer for these specialty topics like diabetes kidney disease. Be familiar with MNT guidelines and guidelines for best therapeutic intervention based on careful assessment of microvascular health. You got this, Coach Beverly
Answer 1 is incorrect, 32% chose this answer, “Initiate low dose ACE Inhibitor or ARB.” This is a juicy answer, however, based on the ADA Standards on Microvascular Complications, medication is not required.
Here are 3 reasons why JR does not need an ACE or ARB:
Since all three of these indicators are below target range, blood pressure medication is not warranted and could even cause unwanted side effects like orthostatic hypotension. About a decade ago, there was a recommendation to start people with type 1 on an ACE or ARB to protect the kidney function, but it is NO longer recommended because it did not improve outcomes.
Answer 2 is correct, 53% of you chose this answer, “Focus on lifestyle changes.” YES, GREAT job. To help JR to keep his vessels healthy and improve his overall nutrition, we are going to encourage regular activity and an evidence based nutrition approach (DASH diet, Mediterranean, Plant Based eating etc.). We will make sure JR has an appointment with a diabetes care and education specialist and RD/RDN. No medications needed for JR, just ongoing self-care support and encouragement.
Answer 3 is incorrect, 9% of you chose this answer, “Maintain protein intake to ~0.7 g/kg.” In the old days, we used to recommend restricting protein intake to less than 0.8g/kg for people with diabetes kidney disease. We no longer make this recommendation since it didn’t improve outcomes! Plus, JR’s kidney function is fine and there is no diabetes kidney disease based on the information provided.
Answer 4 is incorrect, 6% of you chose this answer “Reduce sodium intake to 1000 mg per day.” For people with diabetes, the sodium recommendation is 2,300 mg per day, regardless of their blood pressure, since there is no evidence that a lower sodium intake reduces risk of complications.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Want to learn more about this topic? Enroll in our
Join us for our
Level 2 | Microvascular Complications, Eye Kidney, & Nerve Disease Standards | 1.5 CEs
This course provides you with the need-to-know information regarding the microvascular complications of diabetes. We start with a brief overview of the pathophysiology and clinical manifestations then sum up with prevention strategies and screening guidelines. This straight-forward program will provide you with information you can use in your clinical setting and also provides critical content for the diabetes educator exam.
Objectives:
Can’t make it live? All paid registrants are guaranteed access to the video presentation, handouts and podcasts.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]
Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
For our July 27th Question of the Week, 72% of respondents chose the best answer. GREAT JOB! We want to “take a closer look” at this question and determine strategies to choose the best response.
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer below: Answer Question
Question 1: JR has type 2 diabetes and is trying to lose weight by eating less and moving more. JR asks your advice about drinking diet sodas.
Based on the recommendations in the ADA Standards of Care, what is the best response?
Answer Choices:
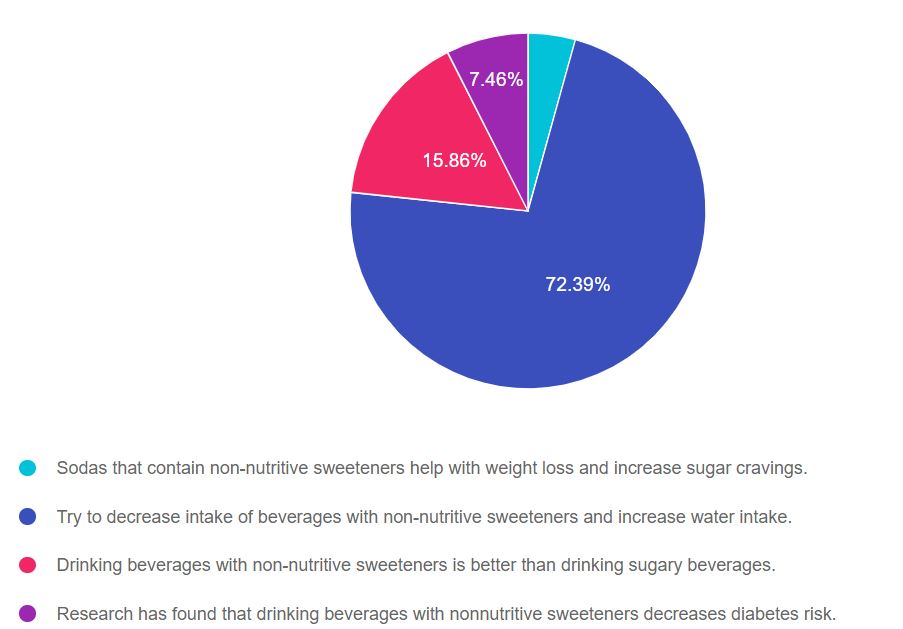
As shown above, the most common choice was option 2, the second most common answer was option 3, then option 4, and finally option 1.
If you are thinking about taking the certification exam, the content of this practice test question will set you up for success. Since medical nutrition therapy (MNT) is an integral part of providing diabetes care, regardless of profession, it will be helpful to be familiar with the MNT guidelines in the ADA Standards of Care 5. Thanks much, Coach Beverly
Answer 1 is incorrect, 4.29% chose this answer, “Sodas that contain non-nutritive sweeteners help with weight loss and increase sugar cravings.” According to the ADA “The addition of nonnutritive sweeteners to diets poses no benefit for weight loss or reduced weight gain without energy restriction.” The ADA Standards makes no comment on sugar cravings associated with non-nutritive sweeteners, so the first and second part of this answer are not based on evidence, which makes this answer false.
Answer 2 is correct, 72.39% of you chose this answer, “Try to decrease intake of beverages with non-nutritive sweeteners and increase water intake.” Yes, this is the best evidence based recommendation for fluid intake, health and diabetes management. I recommend flavored sparkly waters or adding a slice of cucumber, lemon or a fresh strawberry to your glass of H2O and calling it spa water.
Answer 3 is incorrect, 15.86% of you chose this juicy answer, “Drinking beverages with non-nutritive sweeteners is better than drinking sugary beverages.” According to the ADA Standards, “some people with diabetes who are accustomed to regularly consuming sugar-sweetened products, nonnutritive sweeteners (containing few or no calories) may be an acceptable substitute for nutritive sweeteners (those containing calories, such as sugar, honey, and agave syrup) when consumed in moderation.” Clearly, the ADA Standards do not say that beverages with non-nutritive sweeteners are better than sugary beverages, so this answer is juicy answer is false.
Answer 4 is incorrect, 7.46% of you chose this answer “Research has found that drinking beverages with nonnutritive sweeteners decreases diabetes risk.” According to the ADA, some research has found that higher nonnutritive-sweetened beverage and sugar-sweetened beverage consumption may be positively associated with the development of type 2 diabetes.”
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Want to learn more about this topic?
Enroll in our Virtual DiabetesEd Specialist Program!

These courses with Ashley LaBrier, MS, RD, CDCES who is passionate about providing person-centered education to empower those who live with diabetes. Having been diagnosed with type 1 diabetes herself nearly 20 years ago, she combines her professional knowledge with personal experience and understanding.
These courses review the latest national nutrition guidelines and provide strategies to translate this information to an individual living with diabetes. Included is a discussion on different approaches to meal planning and the benefits and limitations of each, meal planning, and the importance of activity with nutrition.
Topics include:
Can’t make it live? All paid registrants are guaranteed access to the video presentation, handouts and podcasts.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]
Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
For our July 20th Question of the Week, 78% of respondents chose the best answer. GREAT JOB! We want to “take a closer look” at this question and determine strategies to choose the best response.
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer below: Answer Question
Question 1: LS is 26 weeks pregnant and just discovered she has gestational diabetes. LS asks you what type of meal planning approach will help keep her and the baby healthy.
According to the ADA Standards of Care, what is the most accurate response?
Answer Choices:
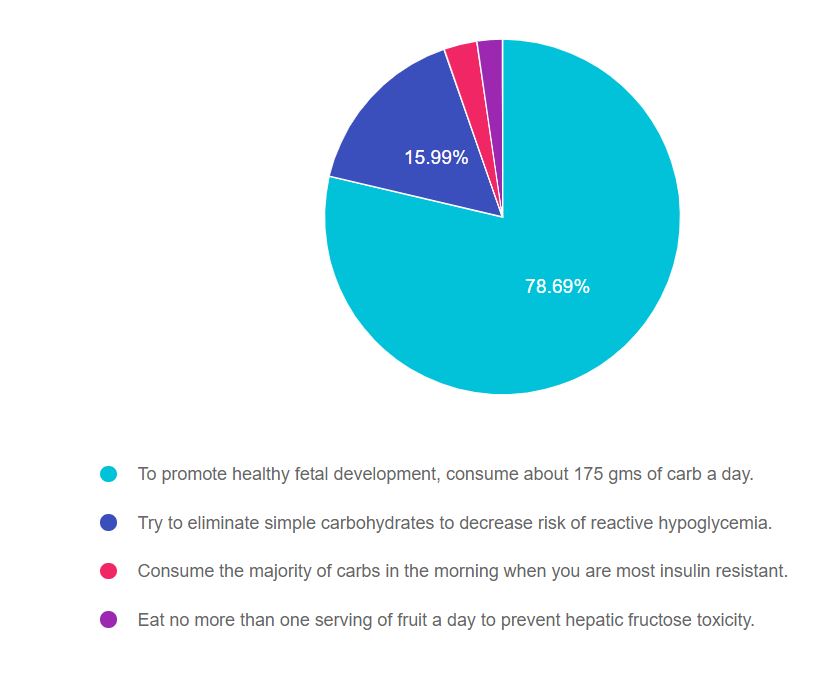
As shown above, the most common choice was option 1, the second most common answer was option 2, then option 3, and finally option 4.
If you are thinking about taking the certification exam, the content of this practice test question will set you up for success. Being familiar with diabetes self-management guidelines and considerations during pregnancy is critical for exam success. If you don’t work with people with diabetes during pregnancy, I encourage you to be familiar with the ADA Standard on Diabetes and Pregnancy and to consider joining our online course for a 1.5 hour painless summary of this standard (see below). Lastly, don’t forget to leverage your common sense and vast health care knowledge to get to the best answer for these specialty topics. Coach Beverly
Answer 1 is correct, 78.69% chose this answer, “To promote healthy fetal development, consume about 175 gms of carb a day.” GREAT JOB. According to the ADA Standard on Diabetes and Pregnancy, the food plan during pregnancy is individualized based on a nutrition assessment with guidance from the Dietary Reference Intakes (DRI). The DRI during pregnancy recommends a minimum of 175 g of carbohydrate, a minimum of 71 g of protein, and 28 g of fiber, with an emphasis on monounsaturated and polyunsaturated fats while limiting saturated fats and avoiding trans fats. All people with diabetes during pregnancy need to meet with a RD/RDN for specific guidance and recommendations.
Answer 2 is incorrect, 15.99% of you chose this answer, “Try to eliminate simple carbohydrates to decrease the risk of reactive hypoglycemia.” This is a juicy answer. It is true that eating less simple carbs, including processed foods and beverages, is a good idea before, during and after pregnancy. However, the second part of the answer makes this response incorrect for two reasons; the term “reactive hypoglycemia” is not a generally accepted diabetes term in this context and eliminating simple carbs would potentially increase the risk of hypoglycemia.
Answer 3 is incorrect, 3.02% of you chose this answer, “Consume the majority of carbs in the morning when you are most insulin resistant.” Part of this answer is correct. During pregnancy, many people are more insulin resistant in the morning. But, if a person is more insulin resistant in the morning, they would decrease the consumption of morning carbs to prevent post breakfast spikes.
Answer 4 is incorrect, 2.31% of you chose this answer “Eat no more than one serving of fruit a day to prevent hepatic fructose toxicity.” During pregnancy, incorporating a variety of fruits in the meal plan is a great idea, since they are packed with micronutrients, vitamins and fiber. They are carbohydrates and will increase blood sugars, so portion size and timing are important to consider when working them into the meal plan.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Want to learn more about this topic? Enroll in our

People living with diabetes who are pregnant are confronted with a variety of issues that require special attention, education, and understanding.
This course reviews those special needs while focusing on Gestational Diabetes and Pre-Existing Diabetes. Included are the most recent diagnostic criteria, management goals, and prevention of complications during pregnancy. A helpful review for the CDCES Exam and for those who want more information on people who are pregnant and live with Diabetes.
Topics include:
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]
Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.