Subscribe
eNewsletter
Ready to get certified?
Free CDCES Coach App
eNewsletter
Free CDCES Coach App
Free Med Pocket Cards
For last week’s practice question, we quizzed participants on who needs to have a bone density evaluation according to the 2026 ADA Standards. 47% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below:

According to the 2026 ADA Standards of Care, what individuals should be recommended to have a bone density evaluation using dual-energy X-ray absorptiometry to evaluate for bone loss?
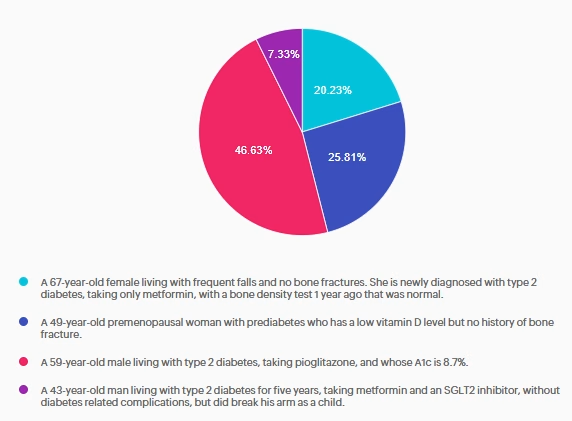
Answer A is incorrect: 20% chose this answer, “A 67-year-old female living with frequent falls and no bone fractures. She is newly diagnosed with type 2 diabetes, taking only metformin, with a bone density test 1 year ago that was normal.” This answer is tempting but incorrect. Per the 2026 ADA Standards of Care, she does meet criteria for assessing bone health due to her diagnosis of type 2 diabetes and risk factor of frequent falls, but she had a bone density test 1 year ago. Currently, the recommendation is to re-evaluate the bone density test in 2-3 years.
Answer B is incorrect: 26% chose this answer, “A 49-year-old premenopausal woman with prediabetes who has a low vitamin D level but no history of bone fracture.” This answer is incorrect. Per the 2026 ADA Standards of Care, it is recommended to assess bone health in postmenopausal women with other diabetes specific risk factors. This risk factor does not include low vitamin D levels.
Answer C is correct: 47% chose the correct answer, GREAT JOB. “A 59-year-old male living with type 2 diabetes, taking pioglitazone, and whose A1c is 8.7%.” Per the 2026 ADA Standards of Care, bone health needs to be assessed in men aged ≥50 years with type 2 diabetes and an A1c >8%. He is also on pioglitazone, a thiazolidinedione, which is another risk factor for low bone density.
Answer D is incorrect: 7% chose this answer, “A 43-year-old man living with type 2 diabetes for five years, taking metformin and an SGLT2 inhibitor, without diabetes related complications, but did break his arm as a child.” This answer is incorrect. Per the 2026 ADA Standards of Care, he has no diabetes-specific risk factors for bone loss. Diabetes duration is less than 10 years, he has no diabetes related complications such as peripheral or autonomic neuropathies, he is not on a high-risk medication for bone loss, and he has not had a bone fracture as an adult.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Course credits through AMA PRA Category 1 Credits™, ACPE, ANCC, and CDR!
Get exam-ready with confidence.
Our CDCES Boot Camp Online Prep Bundle is a comprehensive, high-impact program built specifically for healthcare professionals preparing for the Certified Diabetes Care and Education Specialist (CDCES) exam who want to level up their clinical knowledge and skills.

Course credits through AMA PRA Category 1 Credits™, ACPE, ANCC, and CDR!
Get exam-ready with confidence.
Our comprehensive BC-ADM Online Study Programs are specifically designed for advanced level healthcare professionals who are studying for the Board Certified in Advanced Diabetes Management (BC-ADM) exam.
Gain fresh insights, practical tools, and a deeper understanding of the latest in person-centered diabetes care. Our expert team brings the ADA Standards of Care to life—covering medications, behavior change, technology, and more!

Test your knowledge.
In diabetes care, what is the reported percentage
of patients who have missed or not returned for follow-up care due to feelings of shame, blame, or judgment?

All hours earned count toward your CDCES Accreditation Information
The use of DES products does not guarantee the successful passage of the certification exam. CBDCE and ADCES do not endorse any preparatory or review materials for the CDCES or BC-ADM exams, except for those published by CBDCE & ADCES.

Q: What do you see as the most common misconceptions healthcare professionals have about people who don’t engage effectively with diabetes self-management behaviors?
A: The most common misconceptions are that people who don’t engage with diabetes management are unmotivated, not scared enough, and don’t care about their health.
We asked our favorite diabetes psychologist, Susan Guzman, PhD, to share her insights on how to engage most effectively when providing care to people with diabetes. Keep reading for more expert insights.
Q: How do these misconceptions lead to further problems for people with diabetes and further frustrations for the HCPs?
A: Not understanding the actual barriers to effective engagement leads to responses that don’t help. If you think someone is unmotivated, you might encourage someone to try harder or offer advice that doesn’t meet the person’s needs. If you think someone isn’t taking action because they must not be scared enough, you might try to warn them of all the terrible complications that could happen if they don’t make changes. If you believe someone doesn’t engage with diabetes self-management because they don’t care about their health, you may stop suggesting changes thinking they won’t do it anyway.
Because these are misconceptions, these corresponding tactics are ineffective, often leading people to feel more disengaged and misunderstood, immobilized with fear and hopelessness. In turn, HCPs too can end up feeling more frustrated and hopeless about helping patients reach treatment targets.
Q: What are some of the actual reasons people may not engage with diabetes self-management?
A: There are many common barriers that can result in someone seeing that needed changes as not worth the effort required or seem unachievable. When you begin to see the “good reasons” for people feeling disengaged from diabetes care, you can start to spot solutions that better fit the problem. For example, someone might actually feel doomed (scary complications and early death are unavoidable) and are hopeless that their efforts will have a positive impact. Instead of a scary lecture, this person could really benefit from some “evidence-based hope”, learning that there is good evidence that with targeted effort as a team to reach target, it is possible to have a long and healthy life with diabetes.
Q: Are there quick ways to identify these common barriers to effective diabetes management and brief interventions to help?
A: Yes! There are simple evidence-based ways to identify common behavioral obstacles and address them in routine clinical care. In our one-day workshop, “Engaging the Disengaged: Innovative Strategies for Behavior Change in Diabetes” we will help participants gain confidence in using these tools, having more productive conversations and collaborating with patients in generating more engaging and effective treatment plans.
Q: Are there any upcoming trainings available to explore these techniques and strategies?
A: Yes! Dr. William Polonsky and myself are facilitating a 6-hour conference in San Diego designed to bring these concepts life. This course isn’t a lecture — it’s an immersive, skills-building experience. Using a collaborative, person-centered approach, participants will practice real communication strategies that enhance motivation, build patient confidence, and make self-management feel doable. From diabetes distress to action planning to long-term adherence, every skill you gain is immediately applicable in your practice.
Sign-up today, since we are limiting enrollment to 50 people!

Dr. Susan Guzman is a clinical psychologist specializing in diabetes. In 2003, Dr. Guzman co-founded the Behavioral Diabetes Institute (BDI), the first non-profit organization devoted to the emotional and behavioral aspects of living with diabetes.
At BDI, she serves as the Director of Clinical Education, developing and leading programs for people with diabetes and healthcare professionals. She has helped develop and facilitate diabetes distress group interventions for two NIH-funded research studies for adults with type 1 diabetes.
Dr. Guzman is passionate about helping to change the conversations in diabetes away from shame, blame, and judgment to those based on facts, empathy, and engagement. She has been part of a joint ADA/ADCES effort to address problematic language and messages in diabetes.

Dr. William H. Polonsky, PhD, CDCES
In addition to being the Co-Founder of the Behavioral Diabetes Institute, Dr. Polonsky is Associate Clinical Professor in Medicine at the University of California San Diego.
A licensed clinical psychologist, certified diabetes care and educational specialist (CDCES), and highly-cited research scientist with more than 150 peer-reviewed publications in the field of behavioral diabetes.
His most recent research projects have focused on quality of life in diabetes, diabetes-related distress, hypoglycemic fear, glucose monitoring behavior and attitudes in people living with diabetes, group-based behavior change programs, the influence of continuous glucose monitoring on quality of life, and the development of new methods for enhancing diabetes education. In addition, he continues to maintain a small clinical practice where he works with his patients to help alleviate the stresses, strains and aggravations of living with diabetes.
Of note, he has authored several books for the lay audience (e.g., Diabetes Burnout: What to Do When You Can’t Take it Anymore) and co-edited several others for health care professionals (e.g., A CORE Curriculum for Diabetes Education).
Join national experts including Dr. Diana Isaacs (Cleveland Clinic), Beverly Thomassian (30+ years of experience), and Christine Craig for high-impact, virtual learning—no travel required.
✔ Learn from National Experts — Anywhere
Get the same expert-level instruction you’d receive in person, delivered live to your home or office.
✔ Interactive & Flexible
Walk away with tools you can apply immediately in clinical practice or while preparing for CDCES or BC-ADM exams. From insulin dosing protocols to behavior change strategies that work in the real world—this content bridges theory & practice.

For last week’s practice question, we quizzed participants on JR wanting treatment for pancreatic parasites, and what would be the best response. We share the scoop on pancreatic parasites below. 94.8% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
JR is hospitalized with influenza. They have a history of prediabetes but now have persistent glucose readings between 220–260 mg/dL and are started on basal-bolus insulin.
JR is upset and states: “I’ve been reading that pancreatic parasites can cause of diabetes. No one is treating my infection.”
What is the BEST response?
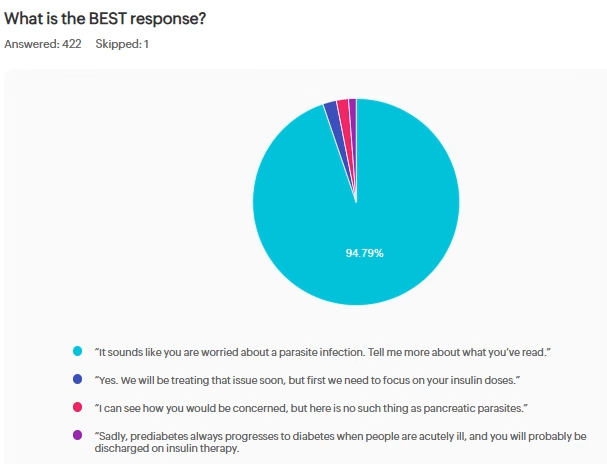
Answer A is correct: 94% chose this answer, “It sounds like you are worried about a parasite infection. Tell me more about what you’ve read.” Great job. A is the best answer because it uses person-centered, nonjudgmental communication, as recommended by the ADA. It avoids dismissive language and explores misinformation respectfully. It preserves the therapeutic alliance.
Since many of you mentioned that patients are asking about parasites causing diabetes – here is the scoop. This false rumor is based on a video from a scientist named Hulda Clark that has since been debunked. Clark falsely claimed that most diseases, including AIDS, Cancer and diabetes, were caused by different parasites and could be cured with an electric “zapper.” Authorities took action against Clark’s “zapper” and other examples of her unproven treatments that she claimed could “cure all diseases” both before and after her death. Read more here
John Buse, MD a professor at the University of North Carolina School of Medicine, said there is a long-standing theory that infection by certain viruses could trigger the body’s immune response that leads to type 1 diabetes, but that no link has been established between a parasitic infection and any type of diabetes. He also said there is no evidence that methanol (another proposed false claim) — a poison — would have any different effect on someone with diabetes than on a person without high blood sugar.
Answer B is incorrect: 3% chose this answer, “Yes. We will be treating that issue soon, but first we need to focus on your insulin doses.” Option B offers a false narrative saying that they are going to treat the parasitic infection then shifts focus to the blood glucose, without recognizing JR’s emotional distress.
Answer C is incorrect: 2% chose this answer, “I can see how you would be concerned, but here is no such thing as pancreatic parasites.” Option C does initially recognize the emotions but then ends with a dismissive tone, that may make JR feel defensive and unheard.
Answer D is incorrect: 1% chose this answer, “Sadly, prediabetes always progresses to diabetes when people are acutely ill, and you will probably be discharged on insulin therapy.” Option D completely ignores the emotional distress in addition to making assumptions that may not be true.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Get exam-ready with confidence.
Course credits through AMA PRA Category 1 Credits™, ACPE, ANCC, and CDR!
Full accreditation details are available on the registration page
Our CDCES Boot Camp Online Prep Bundle is a comprehensive, high-impact program built specifically for healthcare professionals preparing for the Certified Diabetes Care and Education Specialist (CDCES) exam who want to level up their clinical knowledge and skills.
This evidence-based study bundle is a comprehensive BC-ADM Boot Camp designed for advanced-level healthcare professionals preparing for the Board Certified in Advanced Diabetes Management (BC-ADM) exam and will also provide you with state-of-the-art information to level up your clinical practice.
Join national experts including Dr. Diana Isaacs (Cleveland Clinic), Beverly Thomassian (30+ years of experience), and Christine Craig for high-impact, virtual learning—no travel required.
✔ Learn from National Experts — Anywhere
Get the same expert-level instruction you’d receive in person, delivered live to your home or office.
✔ Interactive & Flexible
Walk away with tools you can apply immediately in clinical practice or while preparing for CDCES or BC-ADM exams. From insulin dosing protocols to behavior change strategies that work in the real world—this content bridges theory and practice.
Have you ever left a medical appointment thinking, “I wish I had asked that question,” or “I wish someone really understood what this feels like”?
Managing type 2 diabetes is not just about numbers. It is about decisions. Emotions. Responsibilities. Fatigue. Food. Family. And sometimes feeling like you are carrying all of it alone.
That is why Coach Beverly and DiabetesSisters are proud to launch a new chapter in diabetes support on the West Coast!
Coach Beverly has been a nurse for 40 years and a diabetes specialist for 30. For two decades, she led a hospital-based diabetes support group that became a trusted space for women to gather, learn, and feel understood.
Now, she is bringing that experience to a new West Coast Type 2 Diabetes Support Group with DiabetesSisters.
What drew her to diabetes care was not only the science but the opportunity to make a difference in how women experience living with this condition.
She noticed that many conversations focused on what was not working. Very few recognized the daily effort required to manage a condition no one asked for.
She believes women deserve more than instruction. They deserve encouragement.
As she often reminds participants:
You are already doing more than you think.

This new diabetes support program on the West Coast is built around something simple and powerful: connection.
When women gather in Coach Beverly’s group, they talk about the realities of living with type 2 diabetes, including:
One woman shares something she has never said out loud. Another nods in recognition. And just like that, isolation begins to soften.
Peer support has been shown to strengthen confidence and encourage meaningful behavior change. Our 2024 survey data show that 90 percent of participants felt confident making behavioral changes, and 88 percent felt confident taking steps to support their diabetes management.
But beyond the numbers, there is something deeply human about being seen.
As one participant shared: “I feel so much more connected and less alone in my diabetes journey through the monthly meetings. DiabetesSisters is an amazing resource and community.”
That is the experience this new West Coast program is creating.
Because this is a new program on the West Coast, you have the opportunity to join from the very beginning.
At your first session, you can expect:
At the end of each meeting, you may choose one small, realistic commitment to focus on before the next session. Not a complete life overhaul. Just one doable step.
This is not about perfection. It is about progress. It is about living well while managing diabetes.
If you are a healthcare professional, this new diabetes support program on the West Coast offers an additional layer of care for women living with diabetes.
Diabetes management does not end in the exam room. Women benefit from structured peer support that addresses emotional health, daily decision-making, and lived experience.
Coach Beverly’s group complements clinical care and reinforces self-management behaviors. We welcome referrals for women living with type 2 diabetes who may benefit from additional support.

If you are living with type 2 diabetes and wondering whether this new group is for you, Coach Beverly has a simple invitation:
Come once.
And there is a seat waiting for you.
Join national experts including Dr. Diana Isaacs (Cleveland Clinic), Beverly Thomassian (30+ years of experience), and Christine Craig for high-impact, virtual learning—no travel required.
✔ Learn from National Experts — Anywhere
Get the same expert-level instruction you’d receive in person, delivered live to your home or office.
✔ Interactive & Flexible
Walk away with tools you can apply immediately in clinical practice or while preparing for CDCES or BC-ADM exams. From insulin dosing protocols to behavior change strategies that work in the real world—this content bridges theory & practice.
According to the 2026 ADA Standards of Care, what individuals should be recommended to have a bone density evaluation using dual-energy X-ray absorptiometry to evaluate for bone loss?
Join national experts including Dr. Diana Isaacs (Cleveland Clinic), Beverly Thomassian (30+ years of experience), and Christine Craig for high-impact, virtual learning—no travel required.
✔ Learn from National Experts — Anywhere
Get the same expert-level instruction you’d receive in person, delivered live to your home or office.
✔ Interactive & Flexible
Walk away with tools you can apply immediately in clinical practice or while preparing for CDCES or BC-ADM exams. From insulin dosing protocols to behavior change strategies that work in the real world—this content bridges theory and practice.
Complete Levels 1-3 by April 30th!**
You are going to love the CDCES Boot Camp Online Prep Bundle. We update this comprehensive, high-impact program each year with new material, aimed specifically for healthcare professionals preparing to pass the Certified Diabetes Care and Education Specialist (CDCES) exam and level-up their knowledge.
Complete Levels 2-4 by June 30th!**
You can kick-start your dream of achieving your BC-ADM starting today. Our evidence-based study bundle is a comprehensive BC-ADM Boot Camp designed for advanced-level healthcare professionals preparing for the Board Certified in Advanced Diabetes Management exam. The content also provide you with state-of-the-art information to level up your clinical practice.
**Upon bundle purchase, you have instant access to all of the recorded 2025 content. PLUS you are invited to join the live webinar updates.

Featured Articles & Announcements ___________________________ |
Webinars & Programs
___________________________
March is National Nutrition Month, and I love the core of this year’s theme, “Discover the Power of Nutrition.” Nutrition does have the power to help individuals and communities thrive, especially our cherished community of people with prediabetes and diabetes.
This month, we recognize the impact that nutrition and Registered Dietitian Nutritionists (RDNs) make on people’s lives. All of us have been asked, “Just tell me what I can eat.” We share the basics with our clients and then refer them to our trusted and knowledgeable RDN colleagues, who expertly guide them through medical nutrition therapy and create customized meal plans that encourage folks to “maintain the pleasure of eating”.
In our first article, Christine Craig, MS, RDN, CDCES, explores the role and real impact of RDNs in a variety of settings. Ms. Craig also recognizes that we need to keep inviting people with diabetes to meet with dietitians, as MNT can lower A1C levels by 0.3 – 2%.
Explore our Carb Counting Made Easy Resource Page, featuring handouts, links, and our most frequently requested resources.
Coach Bev provides straightforward strategies (and a New Worksheet) that outline the steps to provide judgment-free coaching to the people in your care. Please, share this worksheet with your colleagues and let us know what you think!
Have you had people with diabetes ask you if those glucose watches really work? Me too! Dr. Beattie discusses which devices are approved for glucose sensing and which are not.
Diabetes Sisters and Coach Bev have teamed up to offer a virtual support group on the West Coast. Thank you in advance for sharing this resource with your clients.
Test your knowledge with a quiz that boldly broaches the topic of Pancreatic Parasites.
Lastly, we heard you! We moved up the dates of our CDCES and BC-ADM Bundles, so you have more time to prepare for exam success.
Celebrating the power of nutrition and RDNs!
Coach Beverly, Bryanna, Astraea & Katarina
Join national experts including Dr. Diana Isaacs (Cleveland Clinic), Beverly Thomassian (30+ years of experience), and Christine Craig for high-impact, 🖥️ virtual learning—no travel required.
✔ Learn from National Experts — Anywhere
Get the same expert-level instruction you’d receive in person, delivered live to your home or office.
✔ Interactive & Flexible
Walk away with tools you can apply immediately in clinical practice or while preparing for CDCES or BC-ADM exams. From insulin dosing 💉 protocols to behavior change strategies that work in the real world—this content bridges theory and practice. 🏫
Set Yourself Up For Certification Success!
Course credits through AMA PRA Category 1 Credits™, ACPE, ANCC, and CDR!
Full accreditation details are available on the registration page
You are going to love the CDCES Boot Camp Online Prep Bundle. We update this comprehensive, high-impact program each year with new material, aimed specifically for healthcare professionals preparing to pass the Certified Diabetes Care and Education Specialist (CDCES) exam and level-up their knowledge.
You can kick-start your dream of achieving your BC-ADM starting today. Our evidence-based study bundle is a comprehensive BC-ADM Boot Camp designed for advanced-level healthcare professionals preparing for the Board Certified in Advanced Diabetes Management exam. The content also provide you with state-of-the-art information to level up your clinical practice.
For last week’s practice question, we quizzed participants on which of the following would NOT justify providing individual DSMES instead of group DSMES. 55.1% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
After the initial assessment JM is scheduled for an individual visit instead of a group DSMES class.
According to Medicare guidelines, which of the following would NOT justify providing individual DSMES instead of group DSMES?
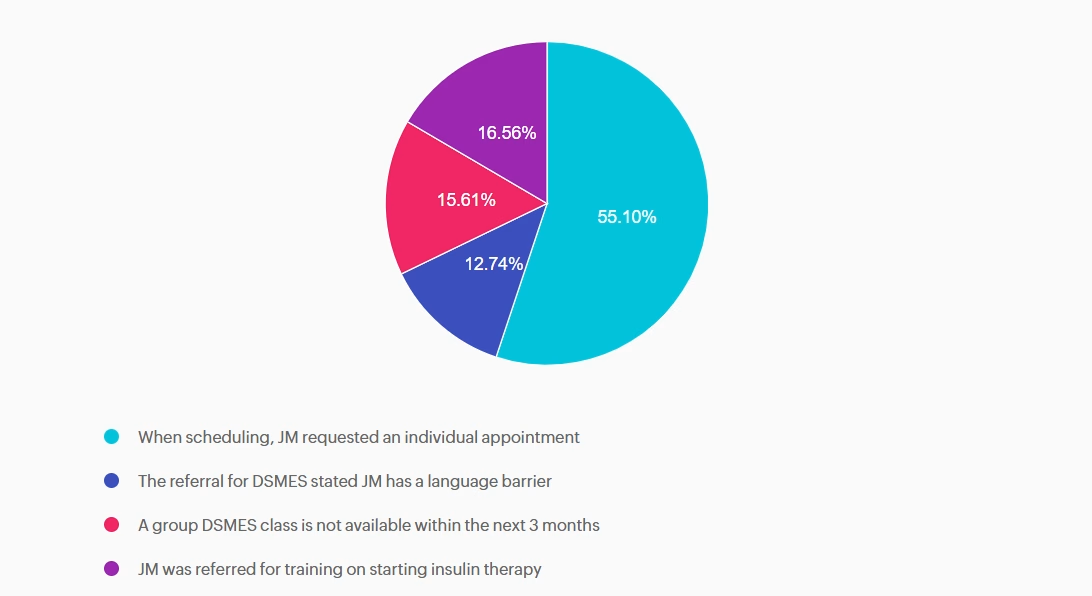
Answer A is correct: 55.1% chose this answer, “When scheduling, JM requested an individual appointment” Answer A is correct; it does NOT justify individual DSMES. Although diabetes care should be patient-centered, patient preference alone does not meet Medicare criteria for individual DSMES. Medicare requires the referring provider document justification of barriers to group learning which can include clinical, educational, or psychosocial need.
Answer B is incorrect: 12.74% chose this answer, “The referral for DSMES stated JM has a language barrier” Answer B is incorrect and does justify individual DSMES. Language barriers can significantly limit participation in group DSMES. Medicare recognizes a referral with stated language and communication needs as valid justification for an individual visit.
Answer C is incorrect: 15.61% chose this answer, “A group DSMES class is not available within the next 3 months” Answer C is incorrect and does justify individual DSMES. Medicare will approve individual DSMES if no group class is available for two months or longer from the date on the referral.
Answer D is incorrect: 16.56% chose this answer, “JM was referred for training on starting insulin therapy” Answer D is incorrect and does justify individual DSMES. A referral for initiation of insulin therapy requires individualized instruction. This can include injection technique, dose adjustment, hypoglycemia prevention, and problem-solving. Medicare considers this
an appropriate reason for individual DSMES.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Course credits through AMA PRA Category 1 Credits™, ACPE, ANCC, and CDR!
Get exam-ready with confidence.
Our CDCES Boot Camp Online Prep Bundle is a comprehensive, high-impact program built specifically for healthcare professionals preparing for the Certified Diabetes Care and Education Specialist (CDCES) exam who want to level-up their clinical knowledge and skills.
✔ Learn at your pace with expert-led, exam-focused content
✔ Everything you need—organized, practical, and in one place
✔ Perfect for self-directed learners who want complete, person-centered content for clinical practice and exam prep.
✔ Build knowledge, sharpen test-taking skills, and prepare with confidence—on your schedule.
Focused. Flexible. Proven.
Basic & e-Deluxe CDCES Boot Camp Bundle Includes:
Course credits through AMA PRA Category 1 Credits™, ACPE, ANCC, and CDR!
Get exam-ready with confidence.
Our comprehensive BC-ADM Online Study Programs are specifically designed for healthcare professionals who are studying for the Board Certified in Advanced Diabetes Management (BC-ADM) exam.
✔ Learn at your pace with expert-led, exam-focused content
✔ Everything you need—organized, practical, and in one place
✔ Perfect for self-directed learners who want complete, person-centered content for clinical practice and exam prep.
✔ Build knowledge, sharpen test-taking skills, and prepare with confidence—on your schedule.
Focused. Flexible. Proven.
Basic & e-Deluxe BC-ADM Boot Camp Bundle include:
Gain fresh insights, practical tools, and a deeper understanding of the latest in person-centered diabetes care. Our expert team brings the ADA Standards of Care to life—covering medications, behavior change, technology, and more!