
Subscribe
eNewsletter
Ready to get certified?
Free CDCES Coach App
eNewsletter
Free CDCES Coach App
Which of the following are considered diabetes autonomic neuropathies?
Click here to test your knowledge!
Want to learn more about this topic? Enroll in our
Join us for our
Level 2 | Microvascular Complications, Eye Kidney, & Nerve Disease Standards | 1.5 CEs
This course provides you with the need-to-know information regarding the microvascular complications of diabetes. We start with a brief overview of the pathophysiology and clinical manifestations then sum up with prevention strategies and screening guidelines. This straight-forward program will provide you with information you can use in your clinical setting and also provides critical content for the diabetes educator exam.
Objectives:
Can’t make it live? All paid registrants are guaranteed access to the video presentation, handouts and podcasts.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.

For our August 3rd Question of the Week, 53% of respondents chose the best answer. We want to “take a closer look” at this question and determine strategies to choose the best response.
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer below: Answer Question
Question 1: JR is 53 years old with type 2 diabetes for the past 7 years. JR’s BMI is 32, GFR is more than 60, blood pressure is 128/76, Urinary Albumin Creatinine Ratio (UACR) is 17mg/g.
According to the ADA Standards, which of the following is the most accurate recommendation to continue to protect JR’s kidney function?
Answer Choices:
As shown above, the most common choice was option 2, the second most common answer was option 3, then option 4, and finally option 1.
If you are thinking about taking the certification exam, the content of this practice test question will set you up for success. Don’t forget to leverage your common sense and vast health care knowledge to get the best answer for these specialty topics like diabetes kidney disease. Be familiar with MNT guidelines and guidelines for best therapeutic intervention based on careful assessment of microvascular health. You got this, Coach Beverly
Answer 1 is incorrect, 32% chose this answer, “Initiate low dose ACE Inhibitor or ARB.” This is a juicy answer, however, based on the ADA Standards on Microvascular Complications, medication is not required.
Here are 3 reasons why JR does not need an ACE or ARB:
Since all three of these indicators are below target range, blood pressure medication is not warranted and could even cause unwanted side effects like orthostatic hypotension. About a decade ago, there was a recommendation to start people with type 1 on an ACE or ARB to protect the kidney function, but it is NO longer recommended because it did not improve outcomes.
Answer 2 is correct, 53% of you chose this answer, “Focus on lifestyle changes.” YES, GREAT job. To help JR to keep his vessels healthy and improve his overall nutrition, we are going to encourage regular activity and an evidence based nutrition approach (DASH diet, Mediterranean, Plant Based eating etc.). We will make sure JR has an appointment with a diabetes care and education specialist and RD/RDN. No medications needed for JR, just ongoing self-care support and encouragement.
Answer 3 is incorrect, 9% of you chose this answer, “Maintain protein intake to ~0.7 g/kg.” In the old days, we used to recommend restricting protein intake to less than 0.8g/kg for people with diabetes kidney disease. We no longer make this recommendation since it didn’t improve outcomes! Plus, JR’s kidney function is fine and there is no diabetes kidney disease based on the information provided.
Answer 4 is incorrect, 6% of you chose this answer “Reduce sodium intake to 1000 mg per day.” For people with diabetes, the sodium recommendation is 2,300 mg per day, regardless of their blood pressure, since there is no evidence that a lower sodium intake reduces risk of complications.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Want to learn more about this topic? Enroll in our
Join us for our
Level 2 | Microvascular Complications, Eye Kidney, & Nerve Disease Standards | 1.5 CEs
This course provides you with the need-to-know information regarding the microvascular complications of diabetes. We start with a brief overview of the pathophysiology and clinical manifestations then sum up with prevention strategies and screening guidelines. This straight-forward program will provide you with information you can use in your clinical setting and also provides critical content for the diabetes educator exam.
Objectives:
Can’t make it live? All paid registrants are guaranteed access to the video presentation, handouts and podcasts.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
AL is 24 with newly diagnosed type 1 diabetes. AL is very worried about going blind because an Aunt with Type 1 diabetes lost her vision due to living with type 1 diabetes.
Which of the following matches the ADA guidelines for diabetes eye care?
Click here to test your knowledge!
Want to learn more about this topic? Enroll in our
Join us for our
Level 2 | Microvascular Complications, Eye Kidney, & Nerve Disease Standards | 1.5 CEs
This course provides you with the need-to-know information regarding the microvascular complications of diabetes. We start with a brief overview of the pathophysiology and clinical manifestations then sum up with prevention strategies and screening guidelines. This straight-forward program will provide you with information you can use in your clinical setting and also provides critical content for the diabetes educator exam.
Objectives:
Can’t make it live? All paid registrants are guaranteed access to the video presentation, handouts and podcasts.
Want to learn more about this topic? Enroll in our
Join us live on August 26th from 11:30 am to 1:00 pm for our
Level 2 | Setting up a Successful DSME Program Standards | 1.5 CEs

This course provides you with a succinct overview of the latest standards for Diabetes Self-Management Education (DSME) and Support Programs. If you are taking the CDCES Exam or considering setting up a DSME program, this program is designed for you. We review the 10 standards and provide strategies on implementation. In addition, we discuss Medicare Reimbursement and covered benefits. This course provides insights into the exam philosophy and also highlights critical content areas.
Objectives:
Can’t make it live? All paid registrants are guaranteed access to the video presentation, handouts and podcasts.
Can’t make it live? All paid registrants are guaranteed access to the video presentation, handouts and podcasts.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
As a child, LR lived with neglect and mistreatment by their parents. Escaping home as a teenager, LR couch surfed at friends but finally ending up living in their car. At the age of 23, LR showed up at our local community clinic with dysregulation, depression, and anxiety coupled with a new diagnosis of type 2 diabetes and elevated triglycerides. LR had limited access to healthy food and carried a BMI of over 35.
After a few months of getting comfortable with the clinic staff, our counselor asked LR to complete the Adverse Childhood Experiences (ACE) screening assessment. After LR finished checking off their adverse childhood experiences, they looked up with tears and said, “I scored a 9 out of 10”.

Adverse Childhood Experiences (ACEs) are common. At least two-thirds of people living in the U.S. have experienced one ACE and over 15% have experienced 4 or more.
Furthermore, a dose-response relationship exists: as the number of adverse experiences increases so does the risk of problems from childhood through adulthood.
These childhood traumas can lead to toxic stress which, over time, can change the biology of our bodiy.
People with elevated ACE scores are more likely to experience a variety of mental health issues, which is not surprising given their painful, confusing, and unsafe childhoods. Based on sound research by the CDC and Kaiser, they are also more likely to suffer from physical diseases, like heart attack and stroke, diabetes, and cancer. They are more likely to break bones and experience unintended pregnancies.
The Impact of Adverse Childhood Experiences on Health: A Personal Story of Resilience and Hope with Coach Beverly
ADCES National Virtual Meeting – Ready for Viewing
California Coordinating ADCES Chapter – September 30, 2021 at 4:45pm PST
Diabetes Ed Services Webinars – airs October 27th at 11:30 am PST
Research shows that ACEs can lead to a cycle of toxic stress and cellular inflammation. This heightened adrenal-mediated “flight or fight” response over time, can lead to neuroendocrine dysregulation, altered immune response, affect DNA packaging and activate epigenetic tags that can alter genetic makeup.
The CDC Morbidity and Mortality Weekly 2019 report tell us that preventing ACEs could reduce:
The first Surgeon General of California, Nadine Burke Harris, MD, MPH, has made it her mission to increase awareness, identify and address ACEs with parents, children, and adults so that we can break the cycle.
Health care professionals at risk for ACEs
People who enter healing professions may be experiencing toxic stress from childhood or current trauma. They may be dealing with burnout, fear, or feelings of deep pain with their past coupled with all the intensity of providing care during the COVID pandemic. This chronic and toxic stress can lead to dysregulation while impairing our ability to cope and care for others. You are not alone.
My own personal journey of experiencing childhood trauma and holding myself together until I ended up in the hospital, has compelled me to share my story with you. And offer a message of hope.
Coach Beverly
As I work on healing and integrating the different aspects of myself, I now feel more attuned to others who have weathered and survived childhood trauma. This awareness has significantly changed the way I hear what people with diabetes are saying and interpret what they are doing. For example, knowing that LR had a very high ACE score, I was able to adjust my expectations and focus on behavior changes that support self-care and self-regulation. When LR doesn’t take their diabetes medications for a few weeks, I provide gentle strength-based coaching to help LR get back on track. I make sure LR knows that they are safe sharing the truth of their story, no matter what.
In your hospital setting, do you have a person who keeps getting readmitted to the hospital in a diabetes crisis? In your outpatient setting, do you experience frequent no-shows or situations where people aren’t able to make changes in self-care? Maybe, they are struggling with the emotional impact of toxic stress.
Adults who have experienced trauma as children may exhibit the following behaviors:
As Diabetes Care and Education Specialists, if we recognize these behaviors as a response to dysregulation due to toxic stress, we can provide a therapeutic response to start the healing process.
Helpful provider responses when you suspect that participants are not engaging in care due to childhood trauma and toxic stress:
Diabetes Care and Education Specialists recognize that the mind and body are a deeply connected, dynamic, and powerful force when they are working together in harmony. When trauma and toxic stress are not recognized or treated, there can be devastating health consequences. We can make a difference in preventing, recognizing, and helping people heal from adverse childhood experiences.
Want to learn more about the ACEs and Healing?
The Impact of Adverse Childhood Experiences on Health:
A Personal Story of Resilience and Hope with Coach Beverly
ADCES National Virtual Meeting – Ready for Viewing
California Coordinating ADCES Chapter – September 30, 2021 at 4:45pm PST
Diabetes Ed Services Webinars – airs October 27th at 11:30 am PST
ACE Screening Tool and Resilience Inventory
Becoming ACE-Aware Training Program
Nadine Burke Harris, MD TED Talk on How Childhood Trauma affects health
NPR Article – Take the ACE Score and Learn what it does and doesn’t mean
Trauma-Informed Care Fact Sheet
Why should I care about my number?
CDC Vital Signs – Impact of ACES
CDC Mortality and Morbidity Weekly Report on ACEs – 2019
What happened to you? Conversations on Trauma, Resilience, and Healing – authors Oprah Winfrey and Bruce D. Perry, M.D., Ph.D.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
We have some heartwarming news to share!
We have awarded 3 DiabetesEd Scholarships to trailblazers who are delivering above and beyond diabetes care to under-resourced individuals and communities across the U.S.
We couldn’t be more proud of these three scholars who have volunteered, innovated and worked hard to make sure their communities get the resources and care needed to thrive with prediabetes and diabetes. If you need some inspiration, please take a moment to read their stories below.
We also take a deep breath and investigate the impact of Adverse Childhood Experiences (ACEs) on the health of all people including those living with diabetes.
Beverly shares her personal experience with ACEs and offers approaches to reaching out to participants and providers living with toxic stress and trauma. We hope you can join us in learning more about this critical topic.
Coach Beverly also interviewed Dr. Ashby Walker to discover why more people with type 1 diabetes aren’t using insulin pumps and CGMs. It turns out that lack of access isn’t the biggest barrier. We take a closer look at the importance of recognizing the expertise of people living with type 1 and the provision of truly collaborative care.
Lastly, just like the Olympians who are boldly working to be their best, but sometimes find themselves with the “twisties”, we keep working toward being the best versions of ourselves as we deliver diabetes care and provide meaningful coaching to each individual.
Keep cool everyone,
Coach Beverly, Bryanna, Jackson, and Robert
Click here to read our full August 2021 newsletter.
Featured Blogs
Upcoming Events & Resources
For our July 27th Question of the Week, 72% of respondents chose the best answer. GREAT JOB! We want to “take a closer look” at this question and determine strategies to choose the best response.
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer below: Answer Question
Question 1: JR has type 2 diabetes and is trying to lose weight by eating less and moving more. JR asks your advice about drinking diet sodas.
Based on the recommendations in the ADA Standards of Care, what is the best response?
Answer Choices:
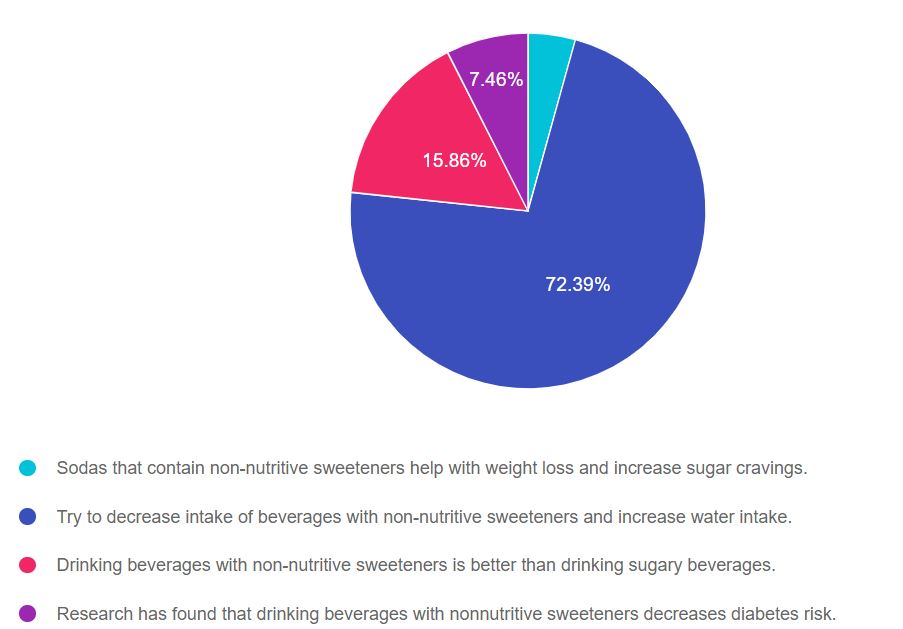
As shown above, the most common choice was option 2, the second most common answer was option 3, then option 4, and finally option 1.
If you are thinking about taking the certification exam, the content of this practice test question will set you up for success. Since medical nutrition therapy (MNT) is an integral part of providing diabetes care, regardless of profession, it will be helpful to be familiar with the MNT guidelines in the ADA Standards of Care 5. Thanks much, Coach Beverly
Answer 1 is incorrect, 4.29% chose this answer, “Sodas that contain non-nutritive sweeteners help with weight loss and increase sugar cravings.” According to the ADA “The addition of nonnutritive sweeteners to diets poses no benefit for weight loss or reduced weight gain without energy restriction.” The ADA Standards makes no comment on sugar cravings associated with non-nutritive sweeteners, so the first and second part of this answer are not based on evidence, which makes this answer false.
Answer 2 is correct, 72.39% of you chose this answer, “Try to decrease intake of beverages with non-nutritive sweeteners and increase water intake.” Yes, this is the best evidence based recommendation for fluid intake, health and diabetes management. I recommend flavored sparkly waters or adding a slice of cucumber, lemon or a fresh strawberry to your glass of H2O and calling it spa water.
Answer 3 is incorrect, 15.86% of you chose this juicy answer, “Drinking beverages with non-nutritive sweeteners is better than drinking sugary beverages.” According to the ADA Standards, “some people with diabetes who are accustomed to regularly consuming sugar-sweetened products, nonnutritive sweeteners (containing few or no calories) may be an acceptable substitute for nutritive sweeteners (those containing calories, such as sugar, honey, and agave syrup) when consumed in moderation.” Clearly, the ADA Standards do not say that beverages with non-nutritive sweeteners are better than sugary beverages, so this answer is juicy answer is false.
Answer 4 is incorrect, 7.46% of you chose this answer “Research has found that drinking beverages with nonnutritive sweeteners decreases diabetes risk.” According to the ADA, some research has found that higher nonnutritive-sweetened beverage and sugar-sweetened beverage consumption may be positively associated with the development of type 2 diabetes.”
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Want to learn more about this topic?
Enroll in our Virtual DiabetesEd Specialist Program!

These courses with Ashley LaBrier, MS, RD, CDCES who is passionate about providing person-centered education to empower those who live with diabetes. Having been diagnosed with type 1 diabetes herself nearly 20 years ago, she combines her professional knowledge with personal experience and understanding.
These courses review the latest national nutrition guidelines and provide strategies to translate this information to an individual living with diabetes. Included is a discussion on different approaches to meal planning and the benefits and limitations of each, meal planning, and the importance of activity with nutrition.
Topics include:
Can’t make it live? All paid registrants are guaranteed access to the video presentation, handouts and podcasts.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
JR is 53 years old with type 2 diabetes for the past 7 years. JR’s BMI is 32, GFR is more than 60, blood pressure is 128/76, Urinary Albumin Creatinine Ratio (UACR) is 17mg/g.
According to the ADA Standards, which of the following is the most accurate recommendation to continue to protect JR’s kidney function?
Click here to test your knowledge!
Want to learn more about this topic? Enroll in our
Level 2 | Microvascular Complications, Eye Kidney, & Nerve Disease Standards | 1.5 CEs
This course provides you with the need-to-know information regarding the microvascular complications of diabetes. We start with a brief overview of the pathophysiology and clinical manifestations then sum up with prevention strategies and screening guidelines. This straight-forward program will provide you with information you can use in your clinical setting and also provides critical content for the diabetes educator exam.
Objectives:
Can’t make it live? All paid registrants are guaranteed access to the video presentation, handouts and podcasts.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
For our July 20th Question of the Week, 78% of respondents chose the best answer. GREAT JOB! We want to “take a closer look” at this question and determine strategies to choose the best response.
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer below: Answer Question
Question 1: LS is 26 weeks pregnant and just discovered she has gestational diabetes. LS asks you what type of meal planning approach will help keep her and the baby healthy.
According to the ADA Standards of Care, what is the most accurate response?
Answer Choices:
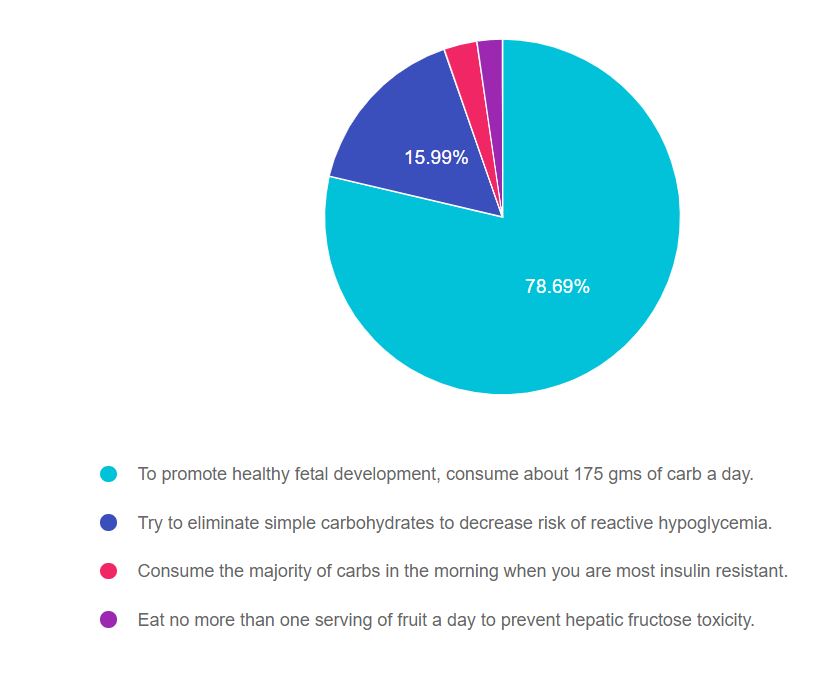
As shown above, the most common choice was option 1, the second most common answer was option 2, then option 3, and finally option 4.
If you are thinking about taking the certification exam, the content of this practice test question will set you up for success. Being familiar with diabetes self-management guidelines and considerations during pregnancy is critical for exam success. If you don’t work with people with diabetes during pregnancy, I encourage you to be familiar with the ADA Standard on Diabetes and Pregnancy and to consider joining our online course for a 1.5 hour painless summary of this standard (see below). Lastly, don’t forget to leverage your common sense and vast health care knowledge to get to the best answer for these specialty topics. Coach Beverly
Answer 1 is correct, 78.69% chose this answer, “To promote healthy fetal development, consume about 175 gms of carb a day.” GREAT JOB. According to the ADA Standard on Diabetes and Pregnancy, the food plan during pregnancy is individualized based on a nutrition assessment with guidance from the Dietary Reference Intakes (DRI). The DRI during pregnancy recommends a minimum of 175 g of carbohydrate, a minimum of 71 g of protein, and 28 g of fiber, with an emphasis on monounsaturated and polyunsaturated fats while limiting saturated fats and avoiding trans fats. All people with diabetes during pregnancy need to meet with a RD/RDN for specific guidance and recommendations.
Answer 2 is incorrect, 15.99% of you chose this answer, “Try to eliminate simple carbohydrates to decrease the risk of reactive hypoglycemia.” This is a juicy answer. It is true that eating less simple carbs, including processed foods and beverages, is a good idea before, during and after pregnancy. However, the second part of the answer makes this response incorrect for two reasons; the term “reactive hypoglycemia” is not a generally accepted diabetes term in this context and eliminating simple carbs would potentially increase the risk of hypoglycemia.
Answer 3 is incorrect, 3.02% of you chose this answer, “Consume the majority of carbs in the morning when you are most insulin resistant.” Part of this answer is correct. During pregnancy, many people are more insulin resistant in the morning. But, if a person is more insulin resistant in the morning, they would decrease the consumption of morning carbs to prevent post breakfast spikes.
Answer 4 is incorrect, 2.31% of you chose this answer “Eat no more than one serving of fruit a day to prevent hepatic fructose toxicity.” During pregnancy, incorporating a variety of fruits in the meal plan is a great idea, since they are packed with micronutrients, vitamins and fiber. They are carbohydrates and will increase blood sugars, so portion size and timing are important to consider when working them into the meal plan.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Want to learn more about this topic? Enroll in our

People living with diabetes who are pregnant are confronted with a variety of issues that require special attention, education, and understanding.
This course reviews those special needs while focusing on Gestational Diabetes and Pre-Existing Diabetes. Included are the most recent diagnostic criteria, management goals, and prevention of complications during pregnancy. A helpful review for the CDCES Exam and for those who want more information on people who are pregnant and live with Diabetes.
Topics include:
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.