Subscribe
eNewsletter
Ready to get certified?
Free CDCES Coach App
eNewsletter
Free CDCES Coach App
Free Med Pocket Cards
Featured Articles ___________________________ |
Upcoming Programs ___________________________
Upcoming FREE Webinars ___________________________ Pre-Order ADA Standards Book for 2026
|
Hi friends, we have two pieces of exciting news!
First, the 2026 ADA Standards of Care are here! This updated content is full of evidence-based guidelines and clinical pearls that you can bring back to your practice, prepare for certification exams, and, of course, advocate on behalf of people living with pre-diabetes and diabetes.
As a busy healthcare professional, we understand that you may not have time to read all 350+ pages! We have a solution.
Join Coach Bev on January 29th for a 2.5 CE Live Webinar that summarizes the critical content you need to know. If you can’t join us live, once you register, you have access to the recorded version for a full year.
You can relax as your expert guide, Coach Bev, leads you through a two hour journey highlighting updates to the ADA Standards. You will walk away feeling confident and focused on what’s most important for certification exams and your practice.
Second exciting announcement!
The New CDCES Coach App is NOW available on Apple and Google Play. Best part? It’s still FREE!
After 6 months of renovation (thanks, Bryanna), you are going to love our new and improved CDCES Coach App. Our older version is sunsetting at the end of the month, so download the new version today! Enjoy quick access to the ADA Standards, new sample test questions with rationales, cheat sheets, Question of the Week and more!
Coach Beverly, Bryanna, Astraea & Katarina

Our new, revitalized CDCES Coach app, will equip you with certification exam study tools and clinical resources- right at your fingertips!
✨ Fresh new design with easier navigation.
New Quizzes with Rationale for In-app Purchase Option
✨ 25 Practice Test Questions with Rationale – Only $9.99! ✨
📱 Register Today! To take advantage of all these enhanced features, you will need to sign up for the new CDCES Coach App! The old app sunsets on 12/31/2025.
You have been asking for these app improvements. We are happy to deliver new features while keeping your favorite resources at the ready!
📱 Works on mobile, tablet, and desktop-friendly!
For last week’s practice question, we quizzed participants on SJ having questions about their insulin pen, and what would be the best response. 41.72% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question

SJ is 52 years old with a 10-year history of type 2 diabetes. They recently started on insulin degludec U-100 Flex Touch pen 15 units per day. At a follow-up visit, SJ brings their insulin pen and mentions they have been keeping it in their work bag since starting therapy. They are unsure how long they can continue to use this same pen.
What is the best advice for SJ for insulin storage in this situation?
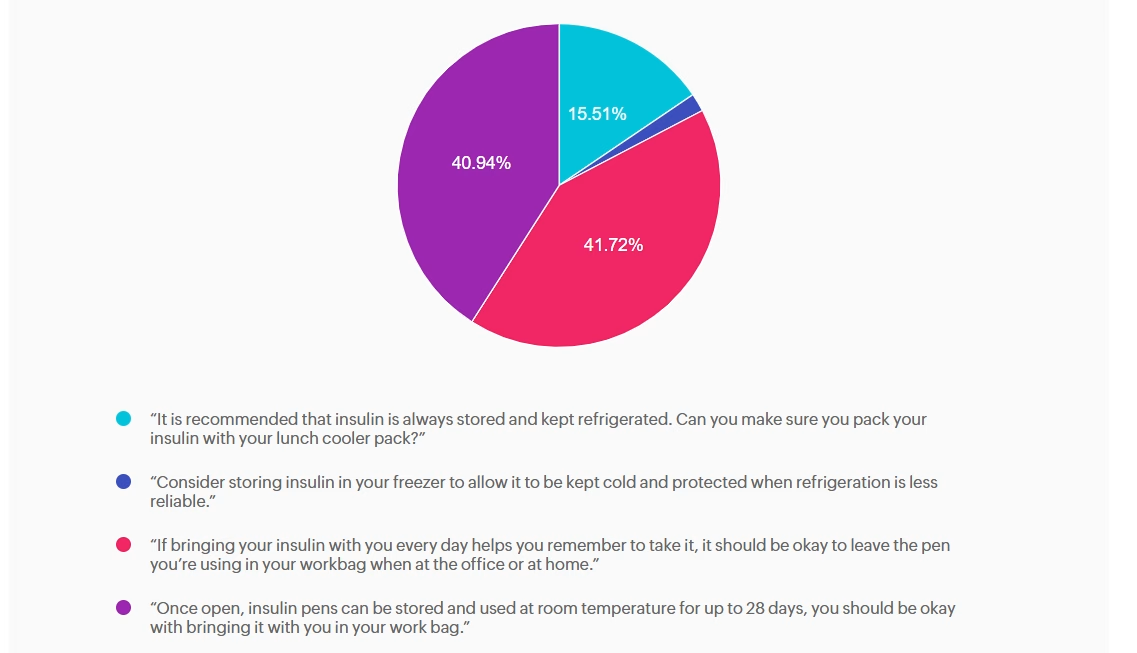
Answer A is incorrect: 15.51% chose this answer, “It is recommended that insulin is always stored and kept refrigerated. Can you make
sure you pack your insulin with your lunch cooler pack?” While refrigeration is ideal for insulin storage, insulin does not always need to be refrigerated. Once in use, most insulins, including degludec, are stable at room temperature (below 86F or 30 C). Advising refrigeration may create unnecessary barriers and does not reflect degludec’s stability profile.
Answer B is incorrect: 1.83% chose this answer, “Consider storing insulin in your freezer to allow it to be kept cold and protected when
refrigeration is less reliable.” Freezing damages insulin molecules, making the insulin ineffective and unsafe to use. This option contradicts manufacturer and clinical safety guidance.
Answer C is correct: 41.72% chose this answer, “If bringing your insulin with you every day helps you remember to take it, it should be
okay to leave the pen you’re using in your workbag when at the office or at home.” Insulin degludec is stable at room temperature below 86°F (30°C) for up to 56 days (8 weeks) once opened. If SJ’s work bag is not exposed to excessive heat or freezing, keeping the pen there is acceptable and may in fact support consistent dosing. We can also calculate SJ’s monthly insulin pen usage (15 units per day + 2 unit prime per injection = 510 units per month or 2 pens per month), knowing he will easily use more insulin than open insulin pen stability time window.
Answer D is incorrect: 40.94% chose this answer, “Once open, insulin pens can be stored and used at room temperature for up to 28 days, you should be okay with bringing it with you in your work bag.” While it is correct that insulin does not always require refrigeration once in use, the specific duration varies by insulin type; degludec lasts longer than 28 days.
To learn more, check out our Insulin Storage Cheat Sheet.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!

Medical Nutrition Therapy (MNT) is effective because it is both
personalized and evidence-based. It can adapt to an individual while being guided by care standards. MNT is defined as a nutrition-based treatment delivered by a Registered Dietitian Nutritionist (or other qualified health professional) for the prevention, treatment and management of medical conditions. It includes nutrition assessment, diagnosis, therapeutic and counseling interventions, monitoring of outcomes, and coordination with care teams. ¹
The nutrition care process can be applied across a wide range of settings, from community, outpatient clinics, hospitals, private practice, long‐term care, telehealth, and more. A recent position paper ², released before publication in the Journal of the Academy of Nutrition and Dietetics, highlighted the effectiveness of MNT in the Prevention and Treatment of Chronic Diseases. They found that despite evidence of the benefit of RDN-delivered nutrition interventions for many chronic conditions, significant
barriers remain in reimbursement, referral processes, and access to care.
Coverage for MNT in the United States varies considerably by payer type. Federally, for Medicare Part B, MNT is covered when a beneficiary has diabetes, non-dialysis chronic kidney disease (stage 3-5), or has had a kidney transplant within the past 36 months. A Medicare-enrolled RDN can schedule and bill for services after obtaining a physician signed (MD or DO) referral, at this time mid-level providers currently do not qualify to sign MNT referrals for Medicare benefit. Medicare provides for up to three hours of MNT in the first year of referral and up to two hours in each subsequent year (with allowance for additional hours if deemed medically necessary). ³ As of January 2025, RDNs can also bill for Direct Training Caregiver Services, which means they can provide education and training to unpaid caregivers who help with tasks like meal preparation and wound care. ²
Medicaid programs are financed by both the state and federal governments, but each state can determine its own coverage and
reimbursement for specific services. State Medicaid programs exhibit significant variability in their coverage and reimbursement rates for MNT services. A recent mapping project by the Academy of Nutrition and Dietetics 4 found that while 37 states recognize MNT billing codes, in only 26 states can RDNs enroll as Medicaid providers (one additional state for pediatric services only), and in only 23 states can RDNs bill independently (others can bill incident-to services). Coverage for MNT services also varies, with some limiting depending on the diagnosis to other states providing reimbursement for a broad range of preventive and medical nutrition therapy. 5
Commercial insurance plans also vary widely in their benefit structure, with some limiting coverage while others extending beyond Medicare-covered diabetes and CKD to also include pre-diabetes, obesity, malnutrition, cardiovascular disease (including hypertension and dyslipidemia), cancer, eating disorders, gastrointestinal conditions, and more.
Although some plans have expanded their coverage, it is not universal and understanding coverage requires knowing an individual’s insurance plan benefits, the RDN network status, diagnosis and referral requirements, the number of covered visits/hours/units, medical or preventive benefit coverage, and, if applicable, telehealth eligibility. Benefits can change annually, and reimbursement rates can also vary widely depending on the state and payer.
When the Affordable Care Act was implemented in 2010 it help provide premium subsidies and increased coverage of preventive and chronic disease services. This led to an increase in MNT coverage expectation and waived share-of-cost for individuals receiving MNT. However, in practice, coverage remains patchwork, with substantial variability in approved diagnoses, covered hours, cost-sharing requirements, and provider networks across plans.
Coordinated care and collaboration are essential for managing chronic conditions, and timely referrals to MNT play a key role in this process. Deciding when to refer should follow disease or area-specific screening criteria (such as validated malnutrition screenings) or as per the Standards of Care in Diabetes, should occur at diagnosis, annually, and whenever treatment goals are unmet, complications develop, or significant life transitions take place. 6
While referral protocols can streamline MNT referrals, access to RDNs remains a challenge in many communities and is further complicated by the need to understand differences in Medicare, Medicaid, and commercial payer coverage so individuals can fully benefit from available services.
Healthcare providers can support individuals receiving care by helping them interpret their plan’s benefits, identify coverage barriers (including limited preventive coverage within Medicare and some Medicaid and commercial plans), and connect them to alternative or complementary resources such as Diabetes Prevention or DSMES programs, community health initiatives, or sliding-scale RDN services when MNT is not covered. Providers can also increase their awareness of policy and advocacy efforts to expand MNT benefit eligibility. ⁷ By working together, the entire care team can strengthen care coordination, enhance access to nutrition services, and support the implementation of MNT to improve our population’s health.
Christine Craig, MS, RDN, CDCES
Founder: Nutrition for Daily Living
References:

JR has been diligently studying to take their CDCES exam at the end of January 2026. They are wondering if they should study the 2025 or 2026 ADA Standards of Care.
As a mentor to healthcare professionals entering the field of diabetes, what do you recommend?
SJ is 52 years old with a 10-year history of type 2 diabetes. They recently started on insulin degludec U-100 Flex Touch pen 15 units per day. At a follow-up visit, SJ brings their insulin pen and mentions they have been keeping it in their work bag since starting therapy. They are unsure how long they can continue to use this same pen.
What is the best advice for SJ for insulin storage in this situation?
The holiday season can bring joy—but also stress, disrupted routines, late nights, and rich meals that may affect blood glucose levels and emotional well-being. For people with diabetes, this time of year can stir feelings of self-doubt and distress, especially if glucose levels veer outside their usual target range.
To help you and your community feel more grounded, we’ve created two helpful resources:
🎁 Holiday Survival Guide
This handout offers 10 practical strategies to stay balanced and navigate holiday gatherings with confidence. Even trying just one or two of the suggestions can make a big difference.
💡 Reframe & Reset: Coping with Diabetes Distress
This companion sheet provides tools to recognize, reframe, and release feelings of shame, guilt, or overwhelm that can surface during the holidays—and beyond.
These printable Cheat Sheets are designed for easy sharing with your friends, clients, and colleagues. Feel free to distribute widely—they’re full of tips to promote self-compassion, support balanced choices, and bring more ease to the season.


1. Be a sleep warrior – People living in the United States are chronically underslept. Not getting enough sleep is associated with increased hunger, higher blood sugars, poor concentration, frequent illness, and impaired problem-solving. Make sure to give yourself the gift of at least 7 hours of sleep a night. This sleep will help you make the best choices for your health and will protect against illness and fatigue. You got this.
Goal: Get at least 7 hours of sleep a night. You deserve it.
2. Keep active – Holidays can put our exercise plans to the test, but we have a few ideas for you. Take an after-meal stroll instead of plopping on the couch. After meal walks lower post-meal blood sugars and increases energy by getting muscles activated. Just 10 minutes of walking after meals can make a big difference. You can even put music on and have a small dance session, anything to get your body moving.
Goal: Work toward 30 minutes of activity a day.

3. Don’t forget the Fiber – With all the snacks and tempting foods, whole healthy foods may take a back seat. Enjoy the abundance of seasonal vegetables, fruits, nuts, and grains that are fiber-rich and that decrease inflammation. Examples include; yams, squash, mandarin oranges, almonds, pistachios, quinoa, kale, brown rice, warm oatmeal, salads, and broth-based soups.
Goal: Strive to eat at least 25gms of fiber a day.

4. Enjoy the ultimate beverage – H20. Water is the perfect way to keep hydrated, replenished, and keeps appetite in check. Add a splash of flavor with a jigger of fruit juice or fresh cucumbers, lime slices, or a sprig of rosemary. Be creative. Sparkling waters come in a vast variety of flavors, are calorie-free, and contain no artificial sweeteners.
Goal: Keep hydrated by enjoying plenty of water.
5. Keep an eye on alcohol – While it’s true that red wine offers a beneficial anti-inflammatory compound called resveratrol, drinking too much alcohol can lead to unintended outcomes. Studies show that we make poorer food choices if alcohol is on board. This can offer special challenges in party settings, where temptations are abundant. A drink of alcohol contains about 100 calories and mixed drinks have even more. In addition, alcohol can lead to low blood sugars, especially for those taking insulin or sulfonylureas.
Goal: Limit alcohol to one drink a day for women, two drinks a day for men.

6. You are already sweet enough – Holidays and sugar go hand in hand. If possible, try and eat less than 6 teaspoons of added sugar (does not include natural sugars found in fruit and milk). This goal may not be realistic on all days, but aim for success most of the time. Excess sugar intake can cause inflammation and buildup of fat in the liver. One strategy is to limit sugar intake during the day and save your 6 teaspoons for that special dessert or parties. When looking at labels, it is helpful to know that 1 teaspoon equals 4 gms of sugar.
Goal: Limit sugar to 6 teaspoons a day.

7. Your teeth need extra special attention – Taking care of our teeth and gums improves health. Gum inflammation is associated with blood vessel inflammation. Swollen gums can also lead to an increase in blood sugars. During the holidays, find time for regular oral hygiene. Your mouth (and dental team) will thank you.
Goal: Brush teeth at twice daily and floss at least once daily.
8. Keep connected to friends and family who love you just the way you are! – As enjoyable as holidays can be, reuniting with family can also cause stress and stir-up emotions. Feeling out of sorts can lead to stress eating and decrease self-care. If possible, reach out to a trusted friend to share your feelings or keep a holiday journal. Consider bringing a favorite book along during your travels that you find inspiring and comforting. Give yourself permission to steal away for some quiet time.
Goal: Self-care is important during the holidays.
9. Enjoy an Oxygen Cocktail – Studies show that when humans venture into natural outdoor settings, heart rate and blood pressure improve. Take a moment to appreciate the feeling of the air on your skin, take a deep breath of fresh air, try to find nests in leafless trees, listen to the animal sounds and bird songs and just enjoy that moment.
Goal: Step into nature daily.
10. Take inventory of things that you are grateful for – Find a moment each day to reflect on a few things that brought you joy or good feelings. Maybe it was your cousin who lent you her favorite sweater. Or an Aunt who gave you the best hug. Special moments with a best friend or an after-dinner walk enjoying the fall leaves. These small moments of connection and beauty are one of the most treasured gifts of the holiday season that linger in our hearts and memory long after we say our goodbyes.
Goal: Take note of special moments.

I love this time of year because we get to celebrate you, the hard-working and dedicated diabetes healthcare professionals.
To allow more healthcare professionals to join the Diabetes Education and Care Specialist community, we have expanded our accreditation.
With our evidence-based courses, we are now providing CEs for physicians, nurses, dietitians, and pharmacists. We want to make sure that anyone who wants to enter the field of diabetes has ample opportunity.
Thank you so much for the lives you touch every day.
Coach Beverly, Bryanna, Astraea & Katarina
Grace is a 38-year-old female who has lived with type 1 diabetes for 20 years. She is a nurse and works variable shifts. She voices concern today about her hemoglobin A1c being elevated at 8.4% over the past 6 months. She is doing everything she can to manage her diet, daily exercise routine, and reports rarely missing insulin doses. She is currently using a Dexcom G7 CGM.
She has never pursued insulin pump therapy because she was fearful that she would no longer be in control of her diabetes if she used a pump. She is now interested in an automated insulin delivery system and asks you which pump is “best” for controlling blood sugar.
What is the best way to answer this question?