
Subscribe
eNewsletter
Ready to get certified?
Free CDCES Coach App
eNewsletter
Free CDCES Coach App
 As you have heard on the news, the town of Paradise and surrounding areas have been completely devastated.
As you have heard on the news, the town of Paradise and surrounding areas have been completely devastated.
Most of the homes and businesses are gone, leaving thousands of people and families searching for shelter.
What is needed now is donations to emergency relief funds so people can start rebuilding their lives.
So many have reached out to check in on us and we appreciate your outpouring of love and support.
Coach Beverly and Anne are determined to keep moving our company forward while supporting the evacuees of Paradise and surrounding communities
SALVATION ARMY Camp Fire Response Center opened a distribution center at 1100 Marauder Street in Chico to serve the needs of individuals affected by the Camp Fire and we are still serving at 8 shelter locations. The warehouse will be a site to collect in-kind donations and to distribute items to fire survivors. Click this link to view needed items and contact info.
Salvation army volunteer sign up here The Salvation Army needs volunteers to help fire survivors get needed supplies and restock the warehouse. Lots of volunteer opportunities available.
Here are a few reputable organizations that you can feel good contributing to knowing that the funds will get to the people who need it most.
Thank you again for all your kindness and concern!
If disaster hits, people with diabetes may need emergency supplies and help fast.
THE DIABETES DISASTER RESPONSE COALITION (DDRC) FORMED IN 2017 IN RESPONSE TO A SUCCESSION OF DEVASTATING ATLANTIC HURRICANES THAT IMPACTED THE MAINLAND US AND TERRITORIES. THE DDRC (FORMERLY KNOWN AS DERC) IS A NATIONAL COALITION OF NONPROFIT AND FOR-PROFIT STAKEHOLDER ORGANIZATIONS DEDICATED TO SERVING THE NEEDS OF THE DIABETES COMMUNITY AND/OR WHO HAVE A ROLE IN PLANNING AND EXECUTING SUPPLY CHAINS, PUBLIC AWARENESS AND HEALTH CARE SERVICES DURING TIMES OF DISASTERS.
Please check out their website at https://www.diabetesdisasterresponse.org/contact/ if you are a diabetes healthcare provider and are requesting information about diabetes supplies during disasters.
Hello Wonderful Community Members,
Many of us want to help, but we are not sure how.
I have put together of volunteer and donation opportunities. If you have more to add let me know and I will keep growing the list.
Thanks – Beverly
SALVATION ARMY Camp Fire Response Center opened a distribution center at 1100 Marauder Street in Chico to serve the needs of individuals affected by the Camp Fire and we are still serving at 8 shelter locations. The warehouse will be a site to collect in-kind donations and to distribute items to fire survivors. Click this link to view needed items and contact info.
Salvation army volunteer sign up here The Salvation Army needs volunteers to help fire survivors get needed supplies and restock the warehouse. Lots of volunteer opportunities available.
Here are a few reputable organizations that you can feel good contributing to knowing that the funds will get to the people who need it most.
Thank you again for all your kindness and concern!

The Camp Fire has deeply affected our sister community of Paradise and beyond. As we sit down in our homes for Thanksgiving dinner, we realize that many of our colleagues, friends and patients with diabetes, will celebrate Thanksgiving in a shelter, facing an uncertain future.
World Central Kitchen is making and serving 15,000 Thanksgiving meals as a gesture of love and community to those displaced by the fire. Bev and her boys volunteered at the World Central Kitchen to make over 500 sandwiches for the first responders and meals for local shelters. But, when an entire town is destroyed, there is so much more to be done.
Coach Beverly and Anne are donating $5,000 to local Camp Fire Organizations through our Online University sales. It’s our message of hope to those struggling through this crisis that, “we believe in you.”
If you are interested in contributing, here is a listing of Camp Fire Organizations.
A heartfelt thanks to all of you who have reached out to us and contributed funds or asked how to help. We love and appreciate our diabetes community. You are AWESOME.
This Thanksgiving, we are especially thankful for all our colleagues and friends who are dedicated to improving the lives of those living with diabetes.
We wish you all love, laughter and the gift of deep connection at your holiday gathering this year!

 Join the Juvenile Diabetes Research Foundation (JDRF) this month as they raise awareness about type 1 diabetes!
Join the Juvenile Diabetes Research Foundation (JDRF) this month as they raise awareness about type 1 diabetes!
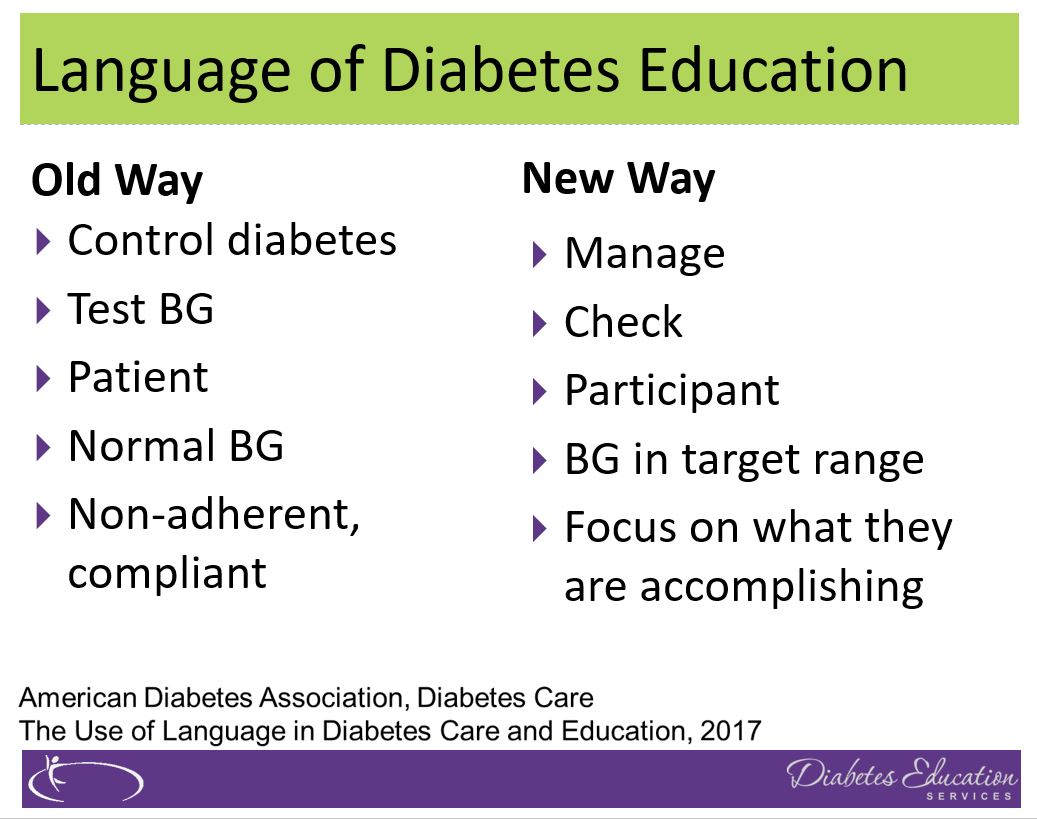
Starting in November, JDRF kicked off Diabetes Awareness Month by sharing personal stories of adversity and perseverance. They are launching a campaign to remind communities that people are not defined by their type 1 diabetes. Here is a brief list of some updated terms to use when talking about diabetes.
They have jazzed up their website so users can access fun and informative quizzes on the JDRF website to test your knowledge of type 1 diabetes.
Plus, on the site, users can also create their own “#ImTheTpye” profile to join the community and spread awareness of type 1 diabetes, like this adorable teenager in the photo. JDRF will also be taking steps to increase research funding as well as guaranteeing that all individuals have access to proper diabetes care.
Make sure to check the JDRF Website after World Diabetes Day on November 14 for more personal stories and blog posts!
Even when everything goes according to plan, the holiday season can be stressful. We get out of our usual rhythms of sleep and work. There are travel negotiations, eating out, parties, counters filled with treats, kids on vacation and visitors.
What can we do to make it through the holiday season and be ready to embark on the new year feeling our best? We have ten strategies for you and your patients. And even if you can’t do all ten, just pick one or a few that you feel you can commit to and succeed with most of the time.
1. Be a sleep warrior – Americans are 
Goal: Get at least 7 hours of sleep a night. You deserve it.
2.
Goal: Work toward 30 minutes of activity a day.
3. Don’t forget the Fiber – With all the snacks and tempting foods, whole healthy foods may take a back seat. Enjoy the abundance of seasonal vegetables, fruits, nuts and grains that are fiber rich and that decrease inflammation. Examples include; yams, squash, mandarin oranges, almonds, pistachios, quinoa, kale, brown rice, warm oatmeal, salads and broth based soups.
Goal: Strive to eat at least 25gms of fiber a day.

Goal: Keep hydrated by enjoying plenty of water.
5. Keep an eye on alcohol – While it’s true that red wine offers a beneficial anti-inflammatory 
Goal: Limit alcohol to one drink a day women, two drinks a day for men.
6. You are already sweet enough – Holidays and sugar go hand in hand. If possible, try and eat less than 6 teaspoons of added sugar (does not include natural sugars found in fruit and milk). This goal may not be realistic on all days, but aim for success 80% of the time. Excess sugar intake can cause inflammation and buildup of fat in the liver. One strategy is to limit sugar intake during the day and save your 6 teaspoons for that special desert or parties. When looking at labels, it is helpful to know that 1 teaspoon equals 4 gms of sugar.
Goal: Limit sugar to 6 teaspoons a day.
7. Your teeth need extra special attention – Taking care of our 
Goal: Brush teeth at twice daily and floss at least one daily.
8. Keep connected to friends and family who love you just the way you are! – As enjoyable as holidays can be, reuniting with family can also cause stress and stir-up emotions. Feeling out of sorts can lead to stress eating and decrease self-care. If possible, reach out to a trusted friend to share your feelings or keep a holiday journal. Consider bringing a favorite book along during your travels that you find inspiring and comforting. Give yourself permission to steal away for some quiet time.
Goal: Self-care is important during the holidays.
9. Enjoy an Oxygen Cocktail – Studies show that when humans venture into natural outdoor settings, heart rate and blood pressure improve. Take a moment to appreciate the feeling of the air on your skin, take a deep breath of fresh air, try to find nests in leafless trees, listen to the animal sounds and bird songs and just enjoy that moment.
Goal: Step into nature daily.
10. Take inventory of things that you are grateful for – 
Goal: Take note of special moments.
10 Steps to Survive the Holidays PDF – a great handout that includes the info above to print and share with your friends, patients and colleagues!
This one-hour complimentary journey will expand your view of how trillions of bacterial hitchhikers profoundly influence our health. We will discuss how foods, the environment and our medical practices have impacted our gut bacteria over time and strategies we can take to protect these old friends. You can either view the webinar for free, or to receive additional CEs, purchase the webinar.
View the webinar now:
This webinar is free and you can view at any time, on any device.
 Giving back to those displaced by the Fire in Paradise, CA
Giving back to those displaced by the Fire in Paradise, CAIf you purchase the Gut Microbiome Online Course, (1.0 CE for $19), all proceeds will be donated to those displaced by the fire. Now through 11/30/2018.
![]()
Or, click this link to see other giving options. Every dollar helps.
FREE Live Webinar November 14th, 20 19 at 11:30 a.m. PST
19 at 11:30 a.m. PST
![]()
New content and exciting research findings!
Join the wonderment as we explore the role of our Microbiome.
This one-hour complimentary journey will expand your view of how trillions of bacterial hitchhikers profoundly influence our health. We will discuss how foods, the environment and our medical practices have impacted our gut bacteria over time and strategies we can take to protect these old friends. Join us!
Webinar topics:
 Presented By: Gutsy Bev and the Microbials
Presented By: Gutsy Bev and the Microbials Feedback from a recent participant:
Feedback from a recent participant:
“This Webinar New Horizons is filled with Bev’s energy, knowledge, and passion for diabetes that she replicates in all her teachings. She puts a demand on herself to be a mentor to all. Her information is well organized, full of current/relevant research, and helps CDCES’s * view into future as a changing world impacts diabetics. I find her to be the most exciting and engaging educator and … OUTSTANDING teacher!!”

The goal of this conference is to give voice to courageous women leaders who have made a significant impact in their communities and beyond. We have carefully created an agenda that includes a collection of women leaders and trailblazers in the field of diabetes. We are inviting them to share their journey and vision to inspire a generation of future luminaries.
Our Intention is to inspire diabetes health care professionals to take risks, try new approaches and envision themselves as powerful change agents.
To generate excitement and action toward change, we are building in purposeful time for networking, creating a plan for change and brief activity breaks between speakers.
Women as Change Agents Conference Brochure
Women as Change Agents Conference Agenda
Registration Fee: (includes breakfast, lunch, Diabetes Med PocketCards, CE Certificate)
![]()
See Bio Page for detailed speaker information
This conference is a labor of love and passion. It is a dream co-opted by two Diabetes Nurse Specialists who believe that woman make a powerful difference in the lives of people living with diabetes.
 Registration Information:
Registration Information:
Date: May 10th, 2019 | 8:00 a.m. – 4:30 p.m.
Location: AC Hotel San Francisco Airport / Oyster Point Waterfront
CEs – 7.5 for Nurses, RDs and CA Pharmacists
So many have reached out to check in on us and we appreciate your outpouring of love and support.
Diabetes Education Services is open and ready to serve. Our office is located in Chico, CA which is about 10 miles west of Paradise and the Camp Fire.
Coach Beverly and Anne are safe and sound and determined to keep moving forward and provide services to our Diabetes Education Community.
As you have heard on the news, the town of Paradise and surrounding areas have been completely devastated.
Most of the homes and businesses are gone and there is only scorched earth in its place.
For twenty years, I have driven up the hill to Paradise on Tuesdays, to run the diabetes program at Adventist Health, Feather River Hospital.
I loved that small community hospital, all the patients I get to work with and our amazing diabetes education staff. Together, we built an ADA Recognized Diabetes Program, a thriving support group and we launched a wildly popular Diabetes Prevention Program in January 2018.
Very sadly, the hospital is partially burnt down and many of the surrounding clinics are completely gone. It is a miracle that the courageous nurses and hospital staff were able to evacuate all the patients to safety while fire was raging all around them. They are such amazing heroes and I am forever thankful for their courage and dedication.
 The future of our Diabetes Education and Prevention Program is unknown, but we will figure out a way to provide this critical service to our community in the near future. I am very worried about several of my patients whom I have known for years and have become such an important part of my life. I hope to hear from them soon.
The future of our Diabetes Education and Prevention Program is unknown, but we will figure out a way to provide this critical service to our community in the near future. I am very worried about several of my patients whom I have known for years and have become such an important part of my life. I hope to hear from them soon.
So many of you have asked how you can help. Most people fled their home with only the clothes on their back and their pets. The shelters are overwhelmed with food and clothing donations.
What is needed now is donations to emergency relief funds.
Here are a few reputable organizations that you can feel good contributing to knowing that the funds will get to the people who need it most.
Thank you again for all your kindness and concern!
With love,
Coach Beverly & Anne