
Subscribe
eNewsletter
Ready to get certified?
Free CDCES Coach App
eNewsletter
Free CDCES Coach App
 November Newsletter is here!
November Newsletter is here!by Coach Beverly
Beverly Thomassian, RN, MPH, CDCES®, BC-ADM
November Newsletter now available!
The theme of this Diabetes Month Celebration focuses on the family unit. Families play an active role in preventing diabetes, supporting each other in making healthier choices and coaching each other to keep moving forward! Articles include:
Click here to read our newsletter!
Our Diabetes Detective Team scans the diabetes news to discover the most relevant info that Diabetes Educators need in their daily practice. We post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]We apologize for the inconvenience, please enjoy other recent Blog Byte:
 Recent Blog Bytes:
Recent Blog Bytes:Mindful Monday | Daylight Savings – Tips to stay healthy during the dark days
Diabetes and Obesity Increase Flu Risk – Vaccinations Save Lives
Free Resource Friday – Preparing for the CDCES Exam Webinar!
Happy Diabetes Month – Toolkits and Resources
Don’t Be Spooked by Leftover Halloween Candy – 7 Strategies
 Research conducted by the University of Queensland has shown that the increased prevalence of chronic conditions such as diabetes and above target weight, will cause more hospitalizations if there is a major flu outbreak.
Research conducted by the University of Queensland has shown that the increased prevalence of chronic conditions such as diabetes and above target weight, will cause more hospitalizations if there is a major flu outbreak.
A factor contributing to this likelihood, is that people who are above target weight or have diabetes, are more likely to get the flu. Plus, this same group is often antibiotic resistant. Which means they may not respond to antibiotics if they get a secondary infection. This can turn a mild flu season into a severe outbreak.
Individuals who are obese or have diabetes “are more likely to be hospitalised or die from the flu,” though it is not yet fully understood why this is the case. These conditions may have a significant affect on immune response which protects against foreign virus’. The inability to fight off a virus may cause a rapid spread of infectious disease.
Scientist believe that the next flu pandemic is eminent as the rates of chronic disease and antibiotic resistance continue to increase. This pandemic may mirror the 1918 Spanish flu that killed between 50-100 million people.
Antibiotic resistance also plays a key role in the spread of infectious diseases. In 1918, many people perished due to the lack of antibiotics. We are now facing a similar situation as many bacteria are becoming resistant to these antibiotics. Climate change may also have a significant impact on the immune response as risk for malnutrition from crop losses increases. Climate change is also affecting animal behavior, such as bird migration patterns, “which can contribute to the spread of the flu.”
Dr. van de Sandt of the University of Queensland states that, “there is a lot to be concerned about, and we still don’t have a vaccine to protect against all the strains of influenza.” Developing a new vaccine is the next big step in preventing this pandemic. Decreasing the rates of diabetes and above target weight will also make a significant impact on immunity and flu prevention.
For more information, visit Rise of diabetes could exacerbate future flu pandemics.
 An abundance of research supports getting adequate sleep for adequate growth and overall health. Health risks increase when an individual is sleep deprived. Sleep deprivation increases risk for type 2 diabetes, high blood pressure, heart disease, and insulin resistance.
An abundance of research supports getting adequate sleep for adequate growth and overall health. Health risks increase when an individual is sleep deprived. Sleep deprivation increases risk for type 2 diabetes, high blood pressure, heart disease, and insulin resistance.
In addition, new research by the academic journal “Sleep,” has shown that,”Social Jet Lag” waking up at different times on the weekends vs. weekdays, may increase the risk of heart disease.
Current research by Duke University Medical Center demonstrated that individuals with what is referred to as “social jet lag” may also have an increased risk of depression and stress than subjects who woke up at the same time consistently. The connection thus far is not clear as some researchers believe that, “poor sleep interferes with the body’s metabolism which can lead to weight gain” which creates a vicious cycle of poor sleep and weight gain. Previous studies have also shown that a varied sleep schedule can lead to the development of obesity and type 2 diabetes.
The authors conclude that further research is needed to determine why individuals who get less sleep are gaining weight and increasing their risk for cardiometabolic conditions.
For more information on “social jet lag” and its effects on cardiometabolic health, visit A regular bedtime may benefit your heart and metabolism”
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]An educational tool to increase knowledge of diabetes self-management terms and goals of care. In Spanish and English.
Players learn about diabetes management while having fun! A must have for support groups and in the classroom setting.
Perfect for Diabetes Awareness Activities. Up to 30 Can play! English on one side, Spanish on the other.
. DiaBingo is now available to download for free in English and Spanish!
Simply print out the player cards and choose items to use as markers to get started.
The questions are designed by our experts to help players become informed about diabetes and self-care in an upbeat and entertaining way. You are welcome to customize these questions as needed to make it relevant to your group.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]
Being a diabetes educator can be challenging. This one-hour presentation by Heather Nielsen, MA, LPC, CHWC will provide diabetes educators with helpful hands-on strategies to incorporate mindfulness and self-compassion into our daily lives and professional practice. As a counselor and a certified wellness coach, Heather has an abundance of wellness wisdom to share with educators who provide lifesaving diabetes education and support to people living with diabetes.
Topics include:
This webinar is free and you can view it at any time, on any device.

Guest speaker: Heather Nielsen, MA, LPC, CHWC – Follow her on her Healthy Connections FaceBook Page
Since 2001, Heather has worked in both medical and behavioral health fields. She is currently a Licensed Professional Counselor and Certified Health and Wellness Coach at Heather Nielsen Counseling and Coaching. Her personal mission is to help people with diabetes find balance, peace, and well-being.“We all need help in managing chronic illness, and I specialize in helping people live well, despite diabetes. With practice and presence, we can learn to transform our brains and our minds, thus finding healthier ways to relate to our disease and to life. I offer a very individualized approach for each client.”
Heather’s passion for mindfulness and diabetes came from her own struggles of living imperfectly with Type 1 since 1997. She is the mother of three teenage daughters, and credits her own practice in mindfulness and self-compassion as a key factor in her good health and happiness in this phase of parenting! She and her husband, an internist, just opened a Functional Medicine clinic in Hood River, Oregon, where they provide team care to people with chronic illnesses of all kinds. Of course, people with diabetes are her favorites.
See more Mindfulness Resources here >>
Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the diabetes certification exams. CBDCE & ADCES does not endorse any preparatory or review materials for the certification exams, except for those published by CBDCE & ADCES.
**To satisfy the requirement for renewal of certification by continuing education for the Certification Board for Diabetes Care & Education (CBDCE), continuing education activities must be applicable to diabetes and approved by a provider on the CBDCE List of Recognized Providers (www.ncbde.org). CBDCE does not approve continuing education. Diabetes Education Services is accredited/approved by the Commission of Dietetic Registration which is on the list of CBDCE Recognized Providers.
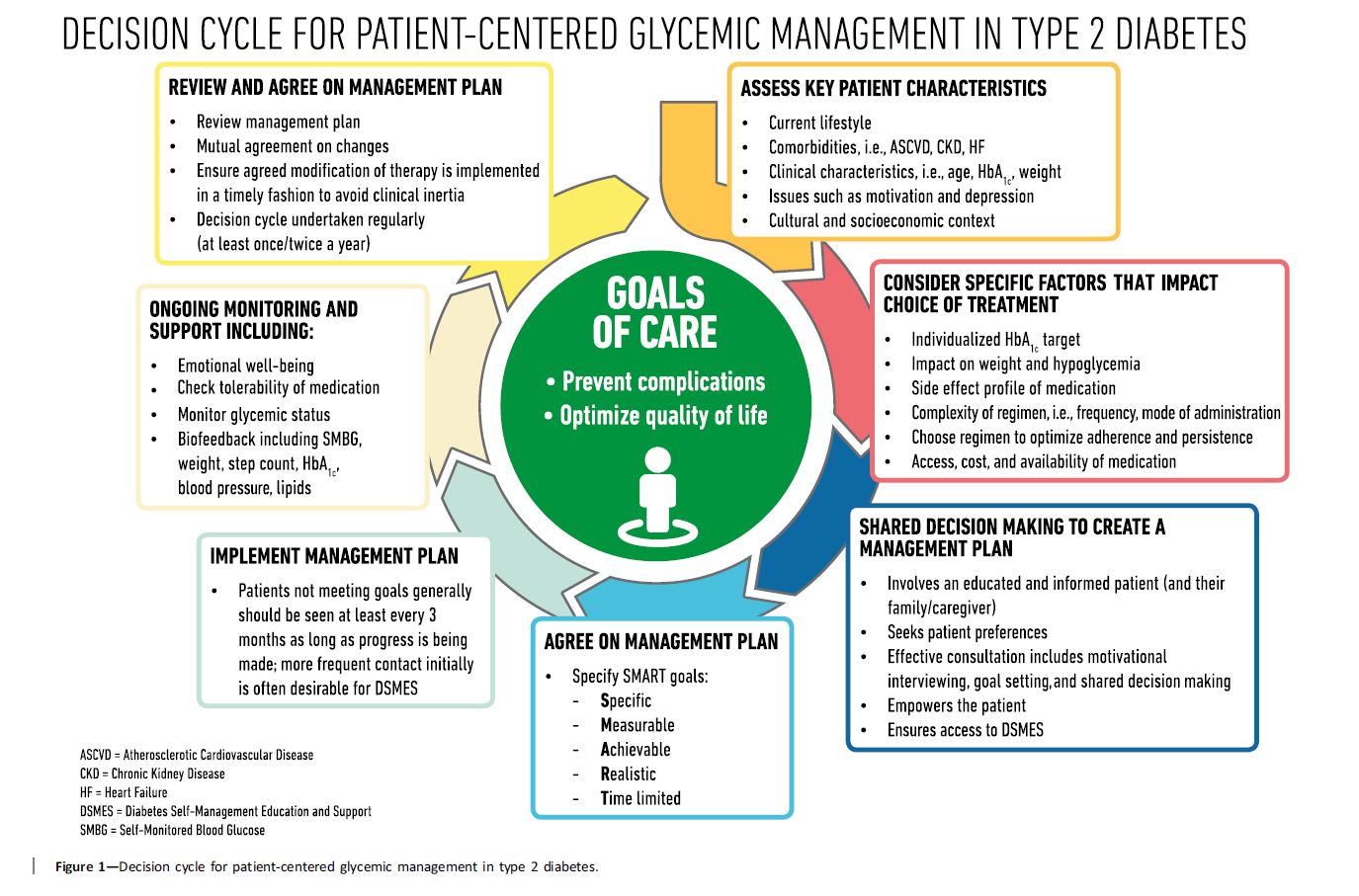
Management of Hyperglycemia in Type 2 Diabetes, 2018. https://doi.org/10.2337/dci18-0033
A Consensus Report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD).
This new consensus statement is a summary of findings based on a comprehensive literature search of peer reviewed articles published from 2014 to February 2018.
Here are some key statements from the Principles of Care Section that really stood out. In addition, the Decision Cycle Chart below, is an excellent summary of person centered considerations to determine the best path to take when deciding upon lifestyle and medication therapy.
Key concepts that I found intriguing and helpful from this section:
Therapeutic inertia, also called clinical inertia, refers to the lack of action even when blood glucose targets are above target. This is something I have frequently seen in my diabetes practice. A common example of this is a PWD on two to three different diabetes medication and basal insulin, with an A1c is greater than 9%, yet no changes in therapy are made for months or years. The causes of this inertia may complex, but can be a result of the provider, person with diabetes or the health care system.
To avoid or stop Clinical inertia, here are recommended strategies:
 Remission of type 2 diabetes: Mission Not Impossible.
Remission of type 2 diabetes: Mission Not Impossible.In the Management of Hyperglycemia in Type 2 Diabetes, 2018.A Consensus Report by the American Diabetes Association (ADA) and the European Association for the Study of Diabetes (EASD), on page 12 and 18, they reference the results of the DiRECT study below. They recommend that all overweight and obese PWD be advised of the health benefits of weight loss and encouraged to engage in an intensive lifestyle program to achieve weight loss reduction.
The DiRECT study, published in the Lancet in February 2018, aimed to assess whether intensive weight management within routine primary care would achieve remission of type 2 diabetes.
Goals of the study were weight loss of 15 kg or more and remission of diabetes, defined as A1c less than 6·5%, after at least 2 months off all antidiabetic medications, from baseline to 12 months.
To evaluate if this was possible, the research team initiated an open-label, cluster-randomised trial (DiRECT) at 49 primary care practices in Scotland and the Tyneside region of England. They recruited individuals aged 20-65 years who had been diagnosed with type 2 diabetes within the past 6 years, had a body-mass index of 27-45 kg/m2, and were not receiving insulin.
All diabetes and hypertension medications were stopped and very low calorie diet was started.
For 12 months, two groups consisting each of 149 participants were followed. The intervention group received weight management support and the control group received no weight loss intervention.
At end of study (12 months), diabetes remission was achieved in 68 (46%) participants in the intervention group and six (4%) participants in the control group
Diabetes remission rates associated with weight status at 12 months:
Other interesting observations:
Nine serious adverse events were reported by seven (4%) of 157 participants in the intervention group and two were reported by two (1%) participants in the control group. Two serious adverse events (biliary colic and abdominal pain), occurring in the same participant, were deemed potentially related to the intervention. No serious adverse events led to withdrawal from the study.
The results show that, at 12 months, almost half of participants in intervention group achieved, with a mean weight loss of 10%, experienced remission to a non-diabetes state without diabetes medications.
The authors conclude that remission of type 2 diabetes through a structured weight loss intervention is a practical target for primary care
Want to read more?
Lancet. 2018 Feb 10;391(10120):541-551. doi: 10.1016/S0140-6736(17)33102-1. Epub 2017 Dec 5.