
Subscribe
eNewsletter
Ready to get certified?
Free CDCES Coach App
eNewsletter
Free CDCES Coach App

Be a part of our diabetes community while learning about the latest in diabetes care. Plus, Coach Beverly provides an interactive question and answer session at the end of each live webinar.
Topics:
This course offers critical content that will help with certification exam success. Coach Beverly will delve into Social Determinants of health, assessment strategies, & behavior change approaches.
She will explore the psychosocial issues that can discourage individuals from adopting healthier behaviors & provide strategies to identify & overcome these barriers. Life studies are used to apply theory to real-life situations. This is a great course for anyone in the field of diabetes education or for those looking for a new perspective on assessment & coping strategies.
Can’t make it live? No worries. We will send post the recorded version to the Online University within 24 hours of the broadcast
Instructor: Beverly Thomassian RN, MPH, CDCES, has been Board Certified in Advanced Diabetes Management for over 20 years. She is an Associate Clinical Professor at UCSF, a working educator, and a nationally recognized diabetes expert. She has a Master’s Degree in Public Health from UCLA, with a focus on behavioral health and education.
All hours earned count toward your CDCES Accreditation Information
Topics:
In this exciting webinar, Coach Beverly walks participants through the “Management of Hyperglycemia in Type 2 Diabetes” as outlined by the most recent American Diabetes Association (ADA) guidelines. She kicks-it off with a brief overview of the different classes of medications then uses a case study approach to apply the ADA algorithm.
Can’t make it live? No worries. We will send post the recorded version to the Online University within 24 hours of the broadcast
Instructor: Beverly Thomassian RN, MPH, CDCES, has been Board Certified in Advanced Diabetes Management for over 20 years. She is an Associate Clinical Professor at UCSF, a working educator, and a nationally recognized diabetes expert. She has a Master’s Degree in Public Health from UCLA, with a focus on behavioral health and education.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.

For last week’s practice question, we quizzed participants on what is the difference between a CDCES & BC-ADM. 57% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
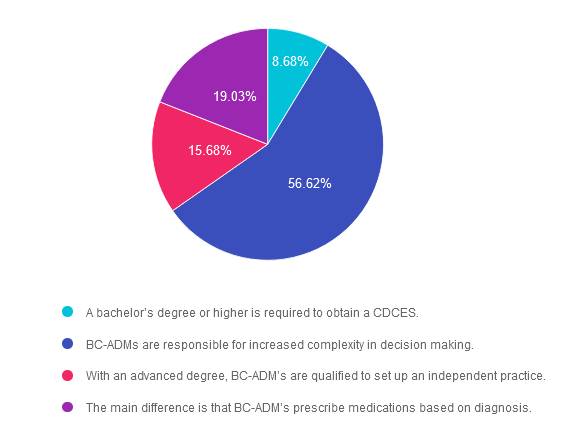
Question: What best describes the difference between a Certified Diabetes Care and Education Specialist (CDCES) and a person Board Certified in Advanced Diabetes Management (BC-ADM)?
Answer Choices:
If you are thinking about taking the certification exam, this practice test question will set you up for success. Test writers anticipate possible answers based on the details in the question. They will wave those “juicy answers” right under your nose. Your job is to weed through the particulars, pluck out the most important elements and choose the BEST answer.
Answer 1 is incorrect. 8.68% chose this answer.” A bachelor’s degree or higher is required to obtain a CDCES.”
Eligibility to take the exam is based on licensure, registration, or certification. According to the CDCES website, the following health care professionals meet the discipline requirement.
Answer 2 is correct. 56.62% of you chose this answer.” BC-ADMs are responsible for increased complexity in decision making.”
Answer 3 is incorrect. About 15.68% of respondents chose this. “With an advanced degree, BC-ADM’s are qualified to set up an independent practice.”
This is a juicy answer but is not correct. Let’s say I want to set up shop as a Registered Nurse with a Masters in Public Health. I also have my CDCES and BC-ADM. Even with my BC-ADM, I couldn’t bill for services, and under whose oversight would I see people with diabetes and make treatment recommendations?
Again, it’s not the BC-ADM that creates the opportunity to set up an independent practice. As a licensed RN, I can’t set up an independent practice and bill for my services in my state. Certification does not change your scope of practice and can come from different organizations. Each state’s licensure and scope of practice regulations come from a governmental authority. We must practice within the legal parameters of our scope of practice based on licensure.
Finally, Answer 4 is incorrect. 19.03% chose this answer. “The main difference is that BC-ADM’s prescribe medications based on diagnosis.”
The BC-ADM is a certification exam and it does not confer prescriptive authority. Only those with certain licenses can prescribe medications, and the regulations can vary from state to state. For example, I am a Registered Nurse with a Masters in Public Health. I also have my CDCES and BC-ADM. As a licensed RN, I do not have prescriptive authority. Certification does not change your scope of practice and can come from different organizations. Licensure comes from governmental authority.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!

Topics:
Coach Beverly is excited to share her insights on determining the best certification choice and the pathway to success. She will share her personal journey on achieving both her CDCES and BC-ADM over 20 years ago and how these credentials have impacted her opportunities as a diabetes specialist and president of her own company. We hope you can join us!
Can’t make it live? No worries. We will send post the recorded version to the Online University within 24 hours of the broadcast
Instructor: Beverly Thomassian RN, MPH, CDCES, has been Board Certified in Advanced Diabetes Management for over 20 years. She is an Associate Clinical Professor at UCSF, a working educator, and a nationally recognized diabetes expert. She has a Master’s Degree in Public Health from UCLA, with a focus on behavioral health and education.
Topics:
In this exciting webinar, Coach Beverly walks participants through the “Management of Hyperglycemia in Type 2 Diabetes” as outlined by the most recent American Diabetes Association (ADA) guidelines. She kicks-it off with a brief overview of the different classes of medications then uses a case study approach to apply the ADA algorithm.
Can’t make it live? No worries. We will send post the recorded version to the Online University within 24 hours of the broadcast
Instructor: Beverly Thomassian RN, MPH, CDCES, has been Board Certified in Advanced Diabetes Management for over 20 years. She is an Associate Clinical Professor at UCSF, a working educator, and a nationally recognized diabetes expert. She has a Master’s Degree in Public Health from UCLA, with a focus on behavioral health and education.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.

The U.S. Food and Drug Administration approved tirzepatide (Zepbound) injection for chronic weight management in adults with a BMI of 30 or with a BMI of 27 or greater with at least one weight-related condition (such as high blood pressure, type 2 diabetes, or high cholesterol) this November. Tirzepatide is a dual glucose-dependent insulinotropic polypeptide (GIP) and glucagon-like peptide-1 (GLP-1) receptor agonist.
Up to 25% body weight loss
The SURMOUNT clinical trials demonstrated that tirzepatide therapy not only improved glucose levels but also had a substantial impact on body weight reduction. At the highest dose (15 mg), people taking Zepbound lost on average 48 lb., while at the lowest dose (5 mg), people lost on average 34 lb. (compared to 7 lb. on placebo).
Additionally, 1 in 3 clinical participants taking Zepbound at the highest dose lost over 58 lb. (25% of body weight), compared to 1.5% on placebo, according to data not controlled for type 1 error. The average starting weight was 231 lb. Zepbound is recommended along with healthy eating and increased activity.
About the SURMOUNT clinical trial program
The SURMOUNT phase 3 global clinical development program for tirzepatide in chronic weight management began in late 2019 and has enrolled more than 5,000 people with obesity or overweight across six registration studies, four of which are global. SURMOUNT-1 and SURMOUNT-2 were submitted to the FDA and demonstrated tirzepatide significantly reduced body weight compared with placebo in people living with obesity or overweight, with or without type 2 diabetes.
The dual action of tirzepatide on both GIP and GLP-1 receptors allows for a comprehensive approach to blood sugar regulation with substantial weight loss. Tirzepatide, the active ingredient in Zepbound, is already approved under the trade name Mounjaro to be used along with diet and exercise to help improve blood sugar in adults with type 2 diabetes. With this new FDA approval for weight loss, people who meet the BMI and risk criteria qualify to use this novel medication class, whether or not they have diabetes.
Cost
Zepbound is expected to be available in the U.S. by the end of the year in six doses (2.5 mg, 5 mg, 7.5 mg, 10 mg, 12.5 mg, 15 mg) at a list price of $1,059.87
Side effects:
Zepbound may be associated with gastrointestinal adverse reactions, sometimes severe. The most commonly reported adverse events (observed in ? 5% of clinical trial participants) were nausea, diarrhea, vomiting, constipation, abdominal pain, dyspepsia, injection-site reactions, fatigue, hypersensitivity reactions, eructation, hair loss, and gastroesophageal reflux disease. In studies, most nausea, diarrhea, and vomiting occurred when people increased their dose – but the effects generally decreased over time. Zepbound may cause tumors in the thyroid, including thyroid cancer. Watch for possible symptoms, such as a lump or swelling in the neck, hoarseness, trouble swallowing, or shortness of breath, and avoid using if there is a family history of medullary thyroid carcinoma (MTC).
For more information, see FDA Approval Information.
Topics:
In this exciting webinar, Coach Beverly walks participants through the “Management of Hyperglycemia in Type 2 Diabetes” as outlined by the most recent American Diabetes Association (ADA) guidelines. She kicks-it off with a brief overview of the different classes of medications then uses a case study approach to apply the ADA algorithm.
Can’t make it live? No worries. We will send post the recorded version to the Online University within 24 hours of the broadcast
Instructor: Beverly Thomassian RN, MPH, CDCES, has been Board Certified in Advanced Diabetes Management for over 20 years. She is an Associate Clinical Professor at UCSF, a working educator, and a nationally recognized diabetes expert. She has a Master’s Degree in Public Health from UCLA, with a focus on behavioral health and education.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
Which of the following strategies is most effective when working with someone with low literacy skills?
Click Here to Test your Knowledge
Topics:
Providing exceptional diabetes care and education begins with our first meeting with an individual with diabetes. Coach Beverly will delve into person-centered interview approaches, including assessing social determinants of health, motivational interviewing & practical communication approaches. This course offers critical content that will help with certification exam success.
Can’t make it live? No worries. We will send post the recorded version to the Online University within 24 hours of the broadcast
Instructor: Beverly Thomassian RN, MPH, CDCES, has been Board Certified in Advanced Diabetes Management for over 20 years. She is an Associate Clinical Professor at UCSF, a working educator, and a nationally recognized diabetes expert. She has a Master’s Degree in Public Health from UCLA, with a focus on behavioral health and education.
All hours earned count toward your CDCES Accreditation Information
Topics:
In this exciting webinar, Coach Beverly walks participants through the “Management of Hyperglycemia in Type 2 Diabetes” as outlined by the most recent American Diabetes Association (ADA) guidelines. She kicks-it off with a brief overview of the different classes of medications then uses a case study approach to apply the ADA algorithm.
Can’t make it live? No worries. We will send post the recorded version to the Online University within 24 hours of the broadcast
Instructor: Beverly Thomassian RN, MPH, CDCES, has been Board Certified in Advanced Diabetes Management for over 20 years. She is an Associate Clinical Professor at UCSF, a working educator, and a nationally recognized diabetes expert. She has a Master’s Degree in Public Health from UCLA, with a focus on behavioral health and education.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
Be a part of our diabetes community while learning about the latest in diabetes care. Plus, Coach Beverly provides an interactive question and answer session at the end of each live webinar.
Topics:
This course discusses common causes of hyperglycemia crises. Topics include hyperglycemia secondary to medications & insulin deprivation. The differences & similarities between Diabetes Ketoacidosis and hyperosmolar Hyperglycemic Syndrome are also covered. Treatment strategies for all situations are included.
Can’t make it live? No worries. We will send post the recorded version to the Online University within 24 hours of the broadcast
Instructor: Beverly Thomassian RN, MPH, CDCES, has been Board Certified in Advanced Diabetes Management for over 20 years. She is an Associate Clinical Professor at UCSF, a working educator, and a nationally recognized diabetes expert. She has a Master’s Degree in Public Health from UCLA, with a focus on behavioral health and education.
All hours earned count toward your CDCES Accreditation Information

Are you considering pursuing certification in diabetes care, but are not sure which certification is right for you and how to get started?
Coach Beverly is excited to share her insights on determining the best certification choice and the pathway to success. She will share her personal journey on achieving both her CDCES and BC-ADM over 20 years ago and how these credentials have impacted her opportunities as a diabetes specialist and president of her own company. We hope you can join us!
Webinar Topics
Can’t make it live? No worries. We will send post the recorded version to the Online University within 24 hours of the broadcast
Instructor: Beverly Thomassian RN, MPH, CDCES, has been Board Certified in Advanced Diabetes Management for over 20 years. She is an Associate Clinical Professor at UCSF, a working educator, and a nationally recognized diabetes expert. She has a Master’s Degree in Public Health from UCLA, with a focus on behavioral health and education.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
For last week’s practice question, we quizzed participants on how to best detect euglycemic ketosis. 53% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question:
According to recent research by the ADA/EASD, about 10% of people admitted to the hospital in diabetes crisis have euglycemic diabetes ketoacidosis.
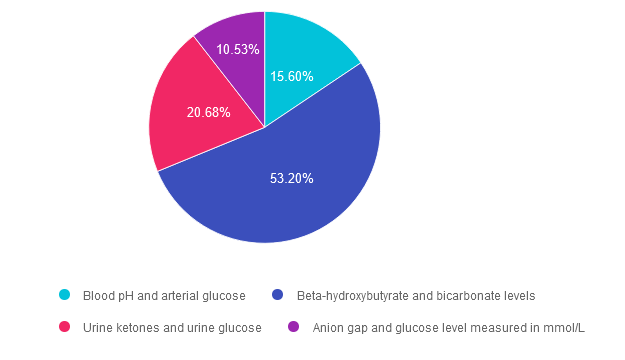
Since blood sugars are at normal levels or only slightly elevated, which of the following lab tests most accurately evaluate for euglycemic ketosis?
Answer Choices:
If you are thinking about taking the certification exam, this practice test question will set you up for success. Test writers anticipate possible answers based on the details in the question. They will wave those “juicy answers” right under your nose. Your job is to weed through the particulars, pluck out the most important elements and choose the BEST answer.
Answer 1 is incorrect. 15.60% chose this answer. “Blood pH and arterial glucose.” Since euglycemic ketosis is often associated with blood glucose levels less than 200 mg/dL, checking arterial glucose levels won’t provide additional clarity on diagnosis. However, checking pH levels is recommended, since a pH less than 7.3 is a clear clinical indication of ketosis.
Answer 2 is correct. 53.20% of you chose this answer. “Beta-hydroxybutyrate and bicarbonate levels.” YES, this is the best answer. Beta-hydroxybutyrate evaluation with a low cutoff equal to or greater than 3.0 mmol/L, whether by lab or point-of-care-testing, is one of the most accurate measurements to evaluate if a person is in ketosis. Bicarbonate level concentration < 18 mmol/L also helps to provide confirmation of ketosis. Ketoacidosis in diabetes is due to inadequate circulating insulin, so the body switches to burning fat for fuel (instead of glucose), which leads to a build up of ketones or ketosis.
Answer 3 is incorrect. About 20.68% of respondents chose this. “Urine ketones and urine glucose.” Urine ketone testing can be used if Beta-hydroxybutyrate evaluation is not available. A urine ketone strip value of 2+ or greater indicates ketosis. However, checking urine glucose levels won’t provide additional clarity on diagnosis, since euglycemic ketosis is often associated with blood glucose levels less than 200 mg/dL.
Finally, Answer 4 is incorrect. 10.53% chose this answer. “Anion gap and glucose level measured in mmol/L.” he anion gap has long been a clinical measure of acidosis; however it is not considered to be a key indicator in the new guidelines. Metabolic acidosis is now defined as a pH < 7.3 and a bicarbonate concentration < 18 mmol/L. The anion gap can still be used in settings where ketone testing is unavailable. In addition, checking urine glucose levels won’t provide additional clarity on diagnosis, since euglycemic ketosis is often associated with blood glucose levels less than 200 mg/dL.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
What best describes the difference between a Certified Diabetes Care and Education Specialist (CDCES) and a person Board Certified in Advanced Diabetes Management (BC-ADM)?
Click Here to Test your Knowledge
Topics:
Coach Beverly is excited to share her insights on determining the best certification choice and the pathway to success. She will share her personal journey on achieving both her CDCES and BC-ADM over 20 years ago and how these credentials have impacted her opportunities as a diabetes specialist and president of her own company. We hope you can join us!
Can’t make it live? No worries. We will send post the recorded version to the Online University within 24 hours of the broadcast
Instructor: Beverly Thomassian RN, MPH, CDCES, has been Board Certified in Advanced Diabetes Management for over 20 years. She is an Associate Clinical Professor at UCSF, a working educator, and a nationally recognized diabetes expert. She has a Master’s Degree in Public Health from UCLA, with a focus on behavioral health and education.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
JR lives with type 1 diabetes and is excited to eat a stack of blueberry pancakes with a new type of maple syrup sweetened with allulose. The syrup label reads that there are 28 grams of carbs in 2 Tablespoons of Zero Sugar Maple syrup. JR adds up the total carbs in the pancakes and syrup, and takes 6 units of bolus insulin (4 for the pancakes and 2 units for the syrup). Within a half hour, JR realizes their blood sugar is dropping fast and grabs some glucose tabs to treat the sudden low. Trying to figure out what went wrong, JR double confirms the nutrition in the pancakes and then takes a closer look at the Maple Syrup label.
Is the Maple Syrup to blame for the Unexpected Low Blood Sugar?
Looking at the label, JR confirms that there are 28 gm of carbs per serving of this unique maple syrup and 26 of those carb grams come from Allulose. Allulose is a low-calorie sugar that is Generally Recognized As Safe (GRAS) approved by the FDA in 2022. Allulose is considered a rare sugar found naturally in figs, raisins, wheat, maple syrup, and molasses or it can be commercially produced and added to foods. It’s roughly 70% as sweet as sugar and it tastes very similar. Allulose is hardly digested or absorbed, so it provides very few calories – approximately 0.4 calories per gram, compared with 4 calories per gram in table sugar.

Allulose labeling Can Cause Confusion for People Matching Insulin to Carbs
In 2019, US Food and Drug Administration (FDA) issued guidance, allowing food manufacturers to exclude allulose from total and added sugar counts on Nutrition and Supplement Facts labels. Like sugar alcohols and dietary fiber, allulose still counts towards total carbohydrates on the nutrition label.
The fact that allulose hardly raises blood sugar may lead people who match insulin to carbs to take more insulin than needed.
FDA Labeling Rule for allulose:
• Not included in “Total Sugars” or ”Added Sugars”
• Included in Total Carbohydrates
• Calories calculated with 0.4 kcals/gram
• Must be in the ingredient list
Take home message for People Counting Carbs for Accurate Insulin Dosing
Look on labels to see if allulose is listed under carbohydrates or included in the ingredient list. If it is, subtract allulose carbs from the total carbs to get an accurate carbohydrate measurement.
For other people, allulose may be a sweet-tasting alternative to sugar that provides few calories and doesn’t raise blood sugar.