
Subscribe
eNewsletter
Ready to get certified?
Free CDCES Coach App
eNewsletter
Free CDCES Coach App
RT says they keep using the same site for their insulin pump, since it doesn’t hurt as much. When you evaluate their abdomen, you notice a large lump at the site.
Why are you worried about this practice?
Click Here to Test your Knowledge
It’s election day. Let’s make sure to get to out and Vote!
Whether you are a novice or an expert in providing diabetes care, we invite you to attend this exciting training program that provides the essential steps to address diabetes distress combined with an innovative approach to glucose management that will revolutionize your practice.
“ReVive 5” breathes new life into our relationship with diabetes, bringing a fresh perspective to both the person with with diabetes and the provider.
By releasing old habits that no longer serve us, we have the opportunity to create a new life tool kit toolkit in partnership with the person living with diabetes.
The ReVive 5 program is built on international research study results and will revolutionize your approach to diabetes self-management education.
Team of Experts:
ReVive 5 is taught by a team of 3 Interdisciplinary Experts:
Training Program Includes:
Don’t worry if you can’t make it live. Your registration guarantees access to the recorded version in the Online University.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
We are excited to announce the new ADA/EASD Consensus Statement on the Management of Hyperglycemia in Type 2 diabetes. Coach Beverly has poured through the pages of this document and is thrilled to share her findings with you. Key points are summarized in the blog article below and you are invited to join her upcoming Diabetes ADA/EASD Updates Webinar on Dec. 1st.
To celebrate Diabetes Month and say thank you to our community of diabetes educators and advocates, we are pleased to announce our annual Cyber Monday Sale.
Take 30% off ALL of our online university courses and bundles on November 28th, for one day only.
Given the prevalence of insulin rationing due to the high cost, we explore reasons and provide resources to help. Hopefully, through advocacy and legislation, this life-saving hormone will be made affordable to people with diabetes in the near future.
We detail the new Freestyle Libre 3 glucose sensor, which is not only smaller but offers several critical features that improve ease of use and functionality for individuals and providers alike.
As the holidays roll around, this can be a gastronomically and emotionally challenging time for people living with diabetes. We are happy to share our “Surviving the Holidays” Handout with all of you. Please feel free to print and share it with your community.
Lastly, we encourage you to test your knowledge with our Question and Rationale of the Week.
Happy Diabetes Month and thank you for your care, concern, and advocacy for people living with diabetes. With thanks,
Beverly, Bryanna, and Amanda
Featured Articles
FREE Resources
Whether you are a novice or an expert in providing diabetes care, we invite you to attend this exciting training program that provides the essential steps to address diabetes distress combined with an innovative approach to glucose management that will revolutionize your practice.
“ReVive 5” breathes new life into our relationship with diabetes, bringing a fresh perspective to both the person with with diabetes and the provider.
By releasing old habits that no longer serve us, we have the opportunity to create a new life tool kit toolkit in partnership with the person living with diabetes.
The ReVive 5 program is built on international research study results and will revolutionize your approach to diabetes self-management education.
Team of Experts:
ReVive 5 is taught by a team of 3 Interdisciplinary Experts:
Training Program Includes:
Don’t worry if you can’t make it live. Your registration guarantees access to the recorded version in the Online University.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.

For last week’s practice question, we quizzed test takers on how Metformin impacts cancer risk. 64% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question:
JR is taking Metformin 1000mg BID but is worried that it may increase their risk of cancer and is thinking about stopping the metformin.
Which of the following is an accurate statement regarding metformin, cancer and safety?
Answer Choices:
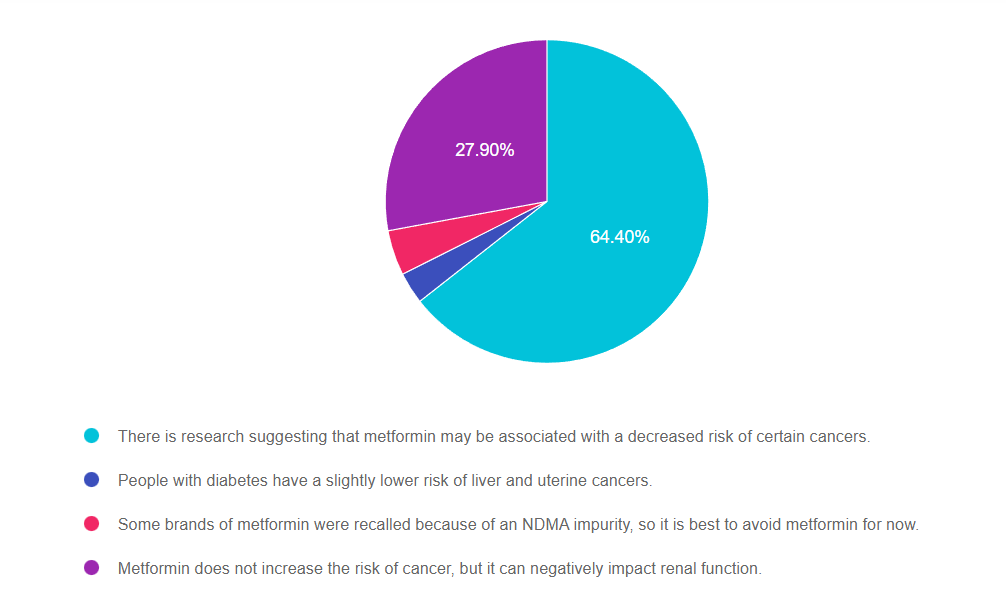
Answer 1 is correct. 64.40% chose this answer, “There is research suggesting that metformin may be associated with a decreased risk of certain cancers.” YES, this is the best answer, GREAT JOB. Research is showing that metformin decreases risk of DNA replication disruption, improves cellular health and increases telomere length. In addition, it enhances intestinal microbial diversity, decreases inflammation and lowers glucose levels. There are many research studies investigating metformin’s potential for cancer prevention and improvement of treatment outcomes.
Answer 2 is incorrect. 3.17% of you chose this answer, “People with diabetes have a slightly lower risk of liver and uterine cancers.” People with diabetes are actually at higher risk for liver, pancreas and breast cancer. Researchers aren’t sure exactly why, but insulin resistance, extra body weight, and DNA replication disruption in addition to genetics and social determinants of health, all seem to play a part.
Answer 3 is incorrect. 4.52.% of respondents chose this answer, “Some brands of metformin were recalled because of an NDMA impurity, so it is best to avoid metformin for now.” Since the NDMA impurity was recognized, manufacturing processes were improved to prevent future contamination. Metformin is an important treatment option for people living with diabetes.
Finally, Answer 4 is incorrect. 27.90% chose this answer, “Metformin does not increase the risk of cancer, but it can negatively impact renal function.” Metformin does NOT harm the kidneys. As a matter of fact, metformin protects the kidneys by lowering blood sugars and decreasing inflammation. It is true that people with a GFR below 30, need to avoid metformin to prevent lactic acidosis, however this a VERY rare complication. Metformin is the most widely used diabetes medication world-wide and it has an excellent safety profile. Bonus note, metformin ER causes less GI upset and costs the same as the non-extended release version ($4 a month).
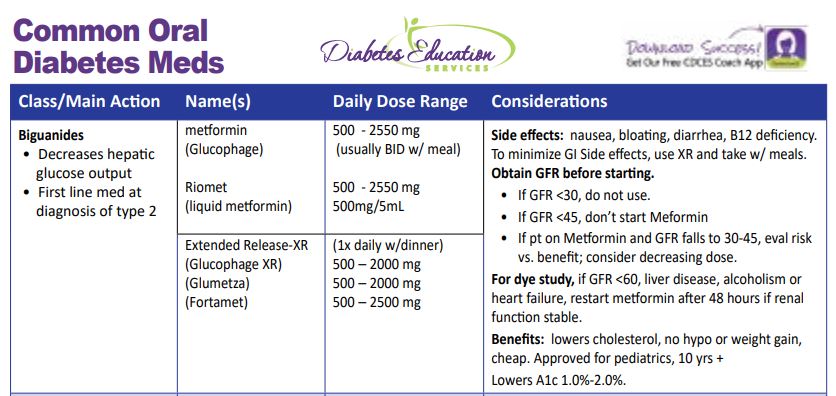
Thank you so much for reading this “Rationale of the Week”. You can download our Medication PocketCard, for more information.

Diabetes Education Services Online University Courses are an excellent way to study for your exam anytime and anywhere that is convenient for you. You will have immediate access to your courses for 1 year after your purchase date. Each individual online course includes a: video presentation, podcast, practice test and additional resources.
Patients with cancer often experience hyperglycemia secondary to treatment, which can increase risk of infection and compromise their nutritional status. In addition, recent research has identified the link between diabetes and cancer. Join us to learn more about this unexpected link and treatment strategies for steroid induced hyperglycemia using a case study approach.
Objectives:
Intended Audience: These courses are knowledge-based activities designed for individual or groups of diabetes educators, including RNs, RDs, Pharmacists, Nurse Practitioners, Clinical Nurse Specialists, Physician Assistants and other health care providers interested in enhancing their knowledge of diabetes management for people with cancer.
Don’t worry if you can’t make it live. Your registration guarantees access to the recorded version in the Online University.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
In the summer of 2021, I decided it was time to get my first pet as an adult. I had just bought my first home and felt I finally had the space to get an animal.

I looked on my local shelter’s website and immediately fell in love with Biscuit. She’s a Calico with striking green, grumpy eyes. Her profile said she had been in the shelter for a long time and wasn’t doing well in that environment. I knew I wanted to bring her home where she could feel safe. I filled out an application and set up an appointment to see her. The next day she came home.
When she arrived, she immediately hid under the couch, unsure of where she was. I sat on the floor with her for a while until she felt okay enough to come out. It took many months for her to feel comfortable, and though at times she is still very anxious, she has relaxed enough to let her personality shine through. She is silly, loves to snuggle, and has a lot of cattitude.

Due to all of her progress, I thought she now might enjoy a friend to hang out with.
In November, I checked my local shelter’s website again and saw Muffin, who like Biscuit, is a Calico with beautiful eyes. Again, I contacted the shelter and went to pick her up. For the first three days, I kept both cats in separate areas of the house, while slowly introducing them over the past few weeks.
Every day, Muffin is building her confidence in her new home; she is very curious, sweet, and loves to play.

Biscuit is still struggling with a new cat in the house, but they are slowly making progress and spending more time together. Muffin loves to follow Biscuit around and mimic what she is doing. I have even caught them laying down next to each other.
I know it will take more time until they become friends, but I am so joyful their relationship is growing.
Written by Bryanna, our Director of Operations & Customer Happiness
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
The new ADA /EASD Management of Hyperglycemia in Type 2 Consensus Statement 2022 was just released.
Which of the following is an accurate recommendation according to these updated guidelines?
Click Here to Test your Knowledge

Plan on joining this exciting webinar that walks participants through the newly released, “Management of Hyperglycemia in Type 2 Consensus Report by the ADA and EASD”. She will highlight the revised guidelines with a focus on new elements and exciting changes on how we approach medication management for type 2 diabetes. Together, we will explore clinical factors to consider when determining the best strategy to improve glucose management in people with type 2 diabetes and other co-conditions. There will be a special focus on cardiovascular risk reduction and renal protection and addressing clinical inertia.
Objectives:
Intended Audience: A great course for health care professionals seeking evidence-based information that improves the quality of life and outcomes.
Don’t worry if you can’t make it live. Your registration guarantees access to the recorded version in the Online University.
For last week’s practice question, we quizzed test takers on basal, bolus and blood transfusions. 62% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question:
JZ is excited about their A1c of 5.4%. They take bolus insulin 4 times a day, plus basal insulin at night. To treat their leukemia, JZ receives blood transfusions weekly.
What is your biggest concern?
Answer Choices:
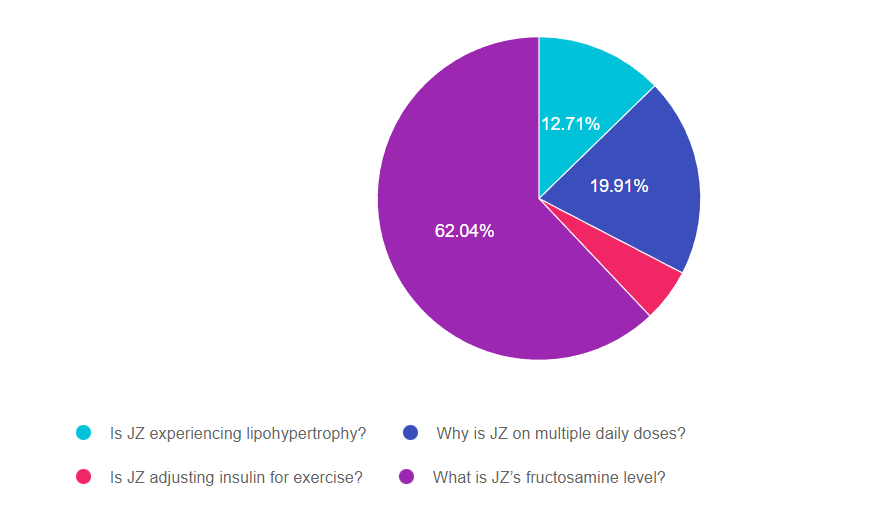
Answer 1 is incorrect. 12.71% chose this answer, “Is JZ experiencing lipohypertrophy?” This answer is tempting, but it is not accurate. Lipohypertrophy is a build up of fat at the injection site, often leading to hyperglycemia (not hypoglycemia) since much of the injected insulin is not being absorbed.
Answer 2 is incorrect. 19.91% of you chose this answer, “Why is JZ on multiple daily doses?” Another tempting answer, but is doesn’t address the reason behind the very low A1C. Certainly, we would want to investigate their regimen safety, but this doesn’t get to the intent of the question.
Answer 3 is incorrect. 5.33.% of respondents chose this answer, “Is JZ adjusting insulin for exercise?” Exercise can cause low blood sugar, but does it explain this A1C of 5.4%. JZ is getting blood transfusions to treat leukemia, can that be affecting their A1C?
Finally, Answer 4 is correct. 62.04% chose this answer, “What is JZ’s fructosamine level?” YES, GREAT JOB. For people receiving blood transfusions, A1C is not an accurate indicator of glucose levels, since they get infusions of non glycosylated red blood cells. This means they have new red blood cells mixing with their own glycosylated blood cells which can result in false lows A1C readings. For this situation, a better measurement is the fructosamine level, which measures the sugar coating of protein in the blood for the past 2-3 weeks. Fructosamine accuracy is not impacted by blood transfusions.
Thank you so much for reading this “Rationale of the Week”. You can download our Medication PocketCard below, for more information.
Diabetes Education Services Online University Courses are an excellent way to study for your exam anytime and anywhere that is convenient for you. You will have immediate access to your courses for 1 year after your purchase date. Each individual online course includes a: video presentation, podcast, practice test and additional resources.
Patients with cancer often experience hyperglycemia secondary to treatment, which can increase risk of infection and compromise their nutritional status. In addition, recent research has identified the link between diabetes and cancer. Join us to learn more about this unexpected link and treatment strategies for steroid induced hyperglycemia using a case study approach.
Objectives:
Intended Audience: These courses are knowledge-based activities designed for individual or groups of diabetes educators, including RNs, RDs, Pharmacists, Nurse Practitioners, Clinical Nurse Specialists, Physician Assistants and other health care providers interested in enhancing their knowledge of diabetes management for people with cancer.
Don’t worry if you can’t make it live. Your registration guarantees access to the recorded version in the Online University.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
JR is taking Metformin 1000mg BID but is worried that it may increase their risk of cancer and is thinking about stopping the metformin.
Which of the following is an accurate statement regarding metformin, cancer and safety?
Click Here to Test your Knowledge
Diabetes Education Services Online University Courses are an excellent way to study for your exam anytime and anywhere that is convenient for you. You will have immediate access to your courses for 1 year after your purchase date. Each individual online course includes a: video presentation, podcast, practice test and additional resources.
Patients with cancer often experience hyperglycemia secondary to treatment, which can increase risk of infection and compromise their nutritional status. In addition, recent research has identified the link between diabetes and cancer. Join us to learn more about this unexpected link and treatment strategies for steroid induced hyperglycemia using a case study approach.
Objectives:
Intended Audience: These courses are knowledge-based activities designed for individual or groups of diabetes educators, including RNs, RDs, Pharmacists, Nurse Practitioners, Clinical Nurse Specialists, Physician Assistants and other health care providers interested in enhancing their knowledge of diabetes management for people with cancer.
Don’t worry if you can’t make it live. Your registration guarantees access to the recorded version in the Online University.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
Diabetes Education Services Online University Courses are an excellent way to study for your exam anytime and anywhere that is convenient for you. You will have immediate access to your courses for 1 year after your purchase date. Each individual online course includes a: video presentation, podcast, practice test, and additional resources.
People with cancer often experience hyperglycemia secondary to treatment, which can increase the risk of infection and compromise their nutritional status. In addition, recent research has identified the link between diabetes and cancer. Join us to learn more about this unexpected link and treatment strategies for steroid-induced hyperglycemia using a case study approach.
Objectives:
Intended Audience: These courses are knowledge-based activities designed for individuals or groups of diabetes educators, including RNs, RDs, Pharmacists, Nurse Practitioners, Clinical Nurse Specialists, Physician Assistants, and other health care providers interested in enhancing their knowledge of diabetes management for people with cancer.
Don’t worry if you can’t make it live. Your registration guarantees access to the recorded version in the Online University.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.