
Subscribe
eNewsletter
Ready to get certified?
Free CDCES Coach App
eNewsletter
Free CDCES Coach App

For last week’s practice question, we quizzed test takers on the best action for glucagon rescue medicine with beer. 70% of respondents chose the best answer. Great JOB. We want to share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question:
RT is a 17-year-old with type 1 diabetes who uses an insulin pump and glucose meter to manage blood glucose levels. RT is out with friends, drinking beers and suddenly passes out. One of RT’s friends carries a glucagon rescue medication and administers it to RT in a panic.
Which of the following statements is most accurate?
Answer Choices:
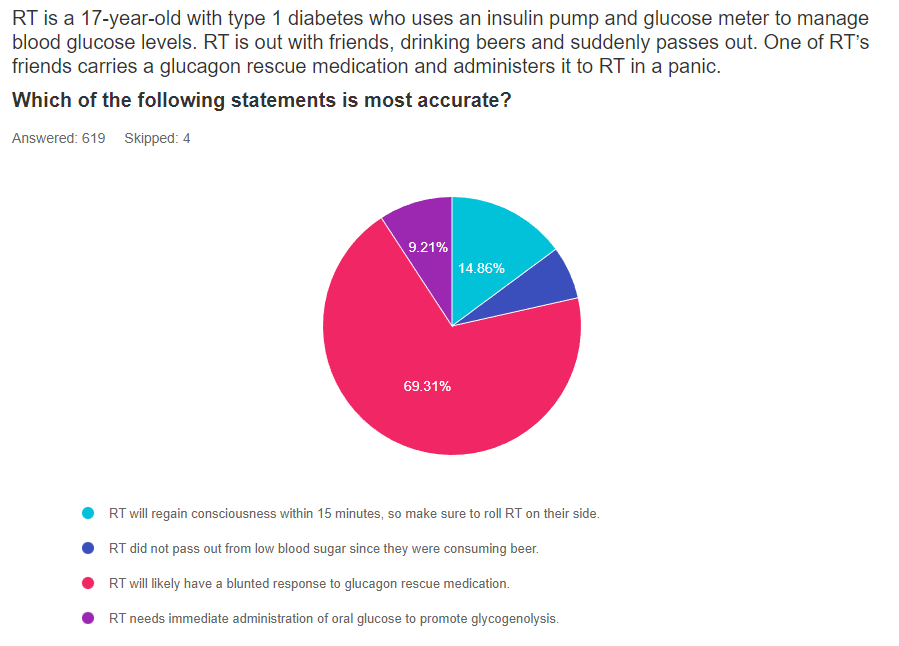
Answer 1 is incorrect. 15% chose this answer, “RT will regain consciousness within 15 minutes, so make sure to roll RT on their side.” Since alcohol consumption slows glycogen breakdown in the liver, higher levels of alcohol in the blood can delay and blunt the effectiveness of glucagon rescue medications. While we hope the RT regains consciousness quickly, there is a real possibility that it will take longer than 15 minutes. However, the second half of the answer offers sound advice. Since people often get nauseated and may vomit after receiving glucagon, it is a good idea to roll RT on their side. See our Blog for more info – Warning Alcohol can Blunt Impact of Glucagon
Answer 2 is incorrect. 5% of you chose this answer, “RT did not pass out from low blood sugar since they were consuming beer.” Although beer may contain some carbohydrate, the body considers alcohol a toxin and as soon as it reaches the bloodstream, the liver prioritizes metabolizing the alcohol and breaking it down. During this clean-up process, the liver is distracted from hormone signals that direct the liver to break down glycogen for energy and liberate glucose into the bloodstream. This clean-up can last for up to 8 hours, making delayed hypoglycemia a real possibility. See our Blog for more info – Warning Alcohol can Blunt Impact of Glucagon
Answer 3 is correct. 70% of respondents chose this answer, “RT will likely have a blunted response to the glucagon rescue medication.” YES, this is the best answer. Alcohol consumption slows glycogen breakdown in the liver, higher levels of alcohol in the blood can delay and blunt the effectiveness of glucagon rescue medications. When a person with type 1 diabetes drink alcohol, they at increased risk of hypoglycemia because the liver is less capable of breaking down stored glycogen.
Having a conversation with people with type 1 about the suppressive nature of alcohol on glycogen release for many hours after consuming alcohol is very important.
As a general rule of thumb, encouraging people with type 1 to eat 15gms of carbs with each drink and have a glass of water in between, may help make sure they have enough circulating carbs and slow the pace of alcohol consumption to help the liver with processing. They may also consider decreasing their insulin dose in association with alcohol intake to prevent this serious side effect. See our Blog for more info- Warning Alcohol can Blunt Impact of Glucagon
Finally, Answer 4 is correct. 9% chose this answer, “RT needs immediate administration of oral glucose to promote glycogenolysis.” This is a juicy answer. AFTER RT regains consciousness, they will certainly need to consume an oral form of energy to replete their glycogen stores and stabilize glucose levels. Of course, it isn’t safe to administer oral glucose when a person loses consciousness. Instead, emergency responders would administer glucagon or dextrose through an IV. See our Blog for more info- Warning Alcohol can Blunt Impact of Glucagon
LS tells you that they frequently attend company mixers where they feel compelled to have at “least a few drinks”, to fit in and network.
The tricky part is that LS lives with type 1 diabetes. Since they don’t have a working pancreas, their circulating levels of insulin and glucagon are often mismatched to their body’s needs.
If LS has several drinks, then loses consciousness from hypoglycemia, will emergency treatment be effective?
There is emerging evidence that glucagon rescue medications may have a blunted response when ingesting alcohol.
This bundle is specifically designed for healthcare professionals who want to learn more about Specialty Topics for their clinical practice or for those who are studying for the Board Certified in Advanced Diabetes Management (BC-ADM) certification exam.
Previously recorded & available for on-demand viewing
All courses air at 11:30 a.m. (PST)

Coach Beverly Thomassian, RN, MPH, BC-ADM, CDCES
Author, Nurse, Educator, Clinician and Innovator, Beverly has specialized in diabetes management for over twenty years. As president and founder of Diabetes Educational Services, Beverly is dedicated to optimizing diabetes care and improving the lives of those with diabetes.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
Have you inspected a salad mix that you bought last week and wondered if you should toss it because it expired yesterday? If you said yes, you are not alone. About 40% of food waste happens in the kitchen, when consumers throw away foods that have passed the expiration date.

However, food and legal experts are asking consumers to reconsider their thinking.
According to an NPR Article, “The U.S. Department of Agriculture, the Food and Drug Administration, the Harvard Food Law Clinic – all say that consumer uncertainty about the meaning of food dates is part of the food waste problem. And it’s not just about wasting food or wasting the water and resources that went into making it. Food is the main thing we send to U.S. landfills.” Food in landfills is converted to methane, a highly potent greenhouse gas.
Consider all the money we are throwing way every day by disposing of foods that might be perfectly fine for consumption. For people living with diabetes on a limited or fixed income, it can really add up. In addition, people may avoid purchasing fresh fruits and vegetables if they are worried about eating it by the date stamped on the package.
Research shows that one in three bags of groceries purchased will end up in the trash due to dates stamped on food items. What do these dates mean anyway?
The federal government doesn’t require dates on any food except baby formula. According to the United States Department of Agriculture (USDA), foods are still safe for consumption after these expiration dates pass, but make sure to look out for an off odor, flavor, or texture that mean the food has spoiled and should not be eaten.
The FDA says the dates on food aren’t serving a safety role. A food and law expert, Broad Leib says, “however, you do want to pay attention to dates on food in the prepared food section, including deli meat, raw fish, unpasteurized milk and cheese.”
But for most foods, like a box of mushrooms or a bottle of ketchup, Broad Leib suggests we take a pause to look at the food. Smell and taste it to determine if it seems okay to eat. We can tell if something went bad.
Except for infant formula, dates are not an indicator of the product’s safety and are not required by Federal law.
Where do the dates come from? Since the federal government doesn’t require the dates, the “sell by” or “enjoy by” dates are determined mostly by the manufacturers. Manufacturers put the date on the package to encourage consumers to eat the food product when it tastes best, not when the food will go “bad”. They want to protect their brand and encourage the consumer to purchase their product again.
Sometimes states will get involved in determining a shelf life of a product for various reasons, including supporting local companies. For this reason, there is a lot of discrepancy from state to state, since the date isn’t based on food spoilage data. An example is that in Montana, milk has to be sold within 12 days of pasteurization. In Idaho, the milk can stay on the shelf for 23 days.
Deciphering Food Label dates:
Food makers, grocery stores, federal agencies are ready to decrease the confusion and food waste. They suggest getting rid of all the “enjoy-by, packaged on” dates and have only two options – best if used by or use by.
“Best if used by” would tell consumers this ketchup would be best by this date, but you could still eat it after.
“Use by” would tell consumers, after this date, it’s probably not a good idea to eat the mustard.
The next time you are ready to toss your salad mix or Worchester sauce, look it over, take a whiff or a taste and you will know if it’s still good to eat.
For more information, see our Protecting the Planet Resource Page.
Your team is invited to our Virtual DiabetesEd™ Training Conference! Set your team apart and prepare for diabetes certification!
Join this state-of-the-art conference taught by content experts, Diana Isaacs, PharmD, BCPS, BCACP, BC-ADM, CDCES, Beverly Thomassian RN, MPH, CDCES, BC-ADM, and Ashley LaBrier who are passionate about improving diabetes care.
?Group discounts are available!*
Download Course Flyer | Download Schedule
Join us LIVE for this Virtual Course and enjoy a sense of community!
Team of expert faculty includes:
Don’t worry if you can’t make it live. Your registration guarantees access to the recorded version in the Online University.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
A person comes into the clinic for a diabetes education appointment. They are on a budget and ask you if they should throw away food if it is older than the date on the package?
What is the most accurate response?
Click Here to Test your Knowledge
Whether you are new to diabetes or a seasoned expert, you’ll benefit from this virtual conference with the latest research plus critical content that you can immediately apply to your clinical practice.
Download Course Flyer | Download Schedule
If you are seeking a state-of-the-art review of current diabetes care, this course is for you. Our team has been fine-tuning this course for over fifteen years, and we know what you need. This program can also be a great addition to your CDCES or BC-ADM exam study plan.
Team of expert faculty includes:
Don’t worry if you can’t make it live. Your registration guarantees access to the recorded version in the Online University.
All hours earned count toward your CDCES Accreditation Information
Have you inspected a food product that you bought last week and wondered if you should toss it because it expired yesterday? If you said yes, you are not alone.
About 40% of food waste happens in the kitchen, when consumers throw away foods that have passed the expiration date.
Are we throwing away perfectly good food based on the date stamped on the package?
Dates are confusing and they are often not associated with safety concerns. Learn why food and legal experts are asking consumers to reconsider their thinking.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
For last week’s practice question, we quizzed test takers on what to do when premeal glucose is too low. 49% of respondents chose the best answer. We want to share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question: RL carb counts and takes 1 unit of insulin for every 10 gms of carbohydrate. RL also uses a correction ratio and takes 1 unit for every 40 points above their glucose target of 120. RL’s asks you what to do if their premeal glucose is less than 70 before their lunch meal at work. RL often has blood sugar drops right before lunch and usually eats a sandwich, chips, berries and some sparkling water for lunch.
Given the situation, what is the best recommendation for JL to do if their pre-lunch glucose is less than 70 mg/g?
Answer Choices:
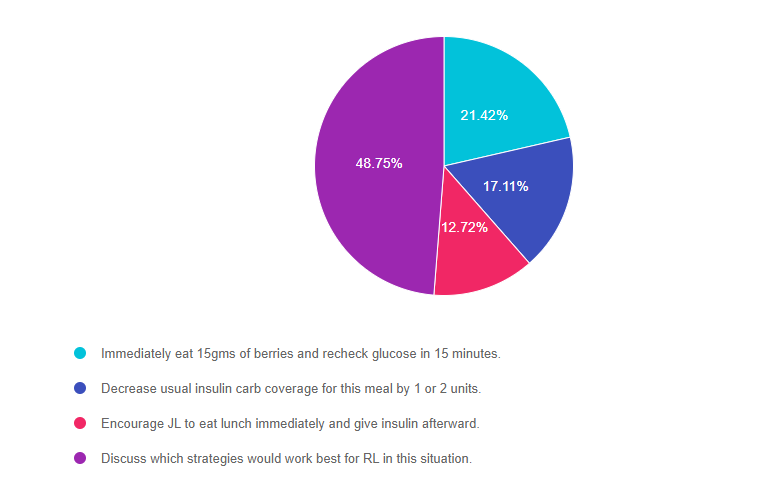
As shown above, the most common choice was option 4, the second most common answer was option 1, then option 2, and finally option 3.
Answer 1 is incorrect. 21.42% chose this answer, “Immediately eat 15gms of berries and recheck glucose in 15 minutes.” This answer is a right answer, but it is not the BEST answer. Yes, we recommend treating low blood sugar with 15 gms of carbohydrate, but is this the preferred treatment strategy for RL? Would RL choose this option?
Answer 2 is incorrect. 17.11% of you chose this answer, “Decrease usual insulin carb coverage for this meal by 1 or 2 units.” This also could be a right answer, but it is not the BEST answer. When faced with a premeal low blood sugar, some people may choose to decrease their bolus insulin dose by 1-2 units, but is this the preferred treatment strategy for RL?
Answer 3 is incorrect. 12.72% of respondents chose this answer, “Encourage RL to eat lunch immediately and give insulin afterward.” This also could be a right answer, but it is not the BEST answer. When faced with a premeal low blood sugar, some people may choose to eat first then give their insulin afterward, based on glucose levels, but is this the preferred treatment strategy for RL?
Finally, Answer 4 is correct. 48.75% chose this answer, “Discuss which strategies would work best for RL in this situation.” YES, this is the BEST answer. RL may choose any of the above mentioned strategies, or RL may have some other ideas on how to manage this situation. Our goal is to keep it person centered and recognize the expertise of the individual who lives with diabetes everyday.

This bundle is specifically designed for healthcare professionals who want to learn more about Specialty Topics for their clinical practice or for those who are studying for the Board Certified in Advanced Diabetes Management (BC-ADM) certification exam.
Previously recorded & available for on-demand viewing
All courses air at 11:30 a.m. (PST)
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
LS tells you that they frequently attend company mixers where they feel compelled to have at “least a few drinks”, to fit in and network. The tricky part of this scenario is that LS lives with type 1 diabetes. Since they don’t have a working pancreas, their circulating levels of insulin and glucagon are often mismatched to their body’s needs.
When discussing the situation, LS says they feel confident they can handle alcohol and prevent lows since they have lived with type 1 diabetes for over ten years. LS shares, “I feel comfortable recognizing when both arrows are pointing down and I am heading for a glucose crash”.
As educators, we are committed to taking person-centered approach while encouraging safe practices.
In regards to LS, we realize alcohol’s impact on the thought process and blood glucose levels. We know that alcohol can affect critical thinking and possibly impair recognition of an impending hypoglycemic event. Inebriation also has many symptoms in common with hypoglycemia. Plus, alcohol consumption slows glycogen breakdown in the liver, which increases the risk of hypoglycemia. Lastly, based on a study published in Endocrinology Advisor, higher levels of alcohol in the blood can delay and blunt the effectiveness of glucagon rescue medications.
In the worst-case scenario, if LS experiences severe low blood sugar and passes out, alcohol ingestion can blunt the effectiveness of the glucagon rescue medications.
Alcohol and Glucagon Pathophysiology Review
The body considers alcohol a toxin and as soon as it reaches the bloodstream, the liver prioritizes metabolizing the alcohol and breaking it down. During this clean-up process, the liver is distracted from responding to endogenous glucagon, the hormone that signals the liver to break down glycogen for energy and liberate glucose into the bloodstream. This clean-up can last for up to 8 hours, making delayed hypoglycemia a real possibility.
When a person with type 1 diabetes drink alcohol, they at increased risk of hypoglycemia because the liver isn’t breaking down stored glycogen to increase blood glucose levels.
Let’s get back to LS. What if LS is drinking gin and diet tonics and only munching on low-carb vegetables and cheeses during the mixer? LS is not ingesting many carbohydrates, so glycogen stores may be low and the liver is busy cleaning up the alcohol and blood sugars start dropping. By the 4th drink, LS isn’t thinking very clearly, says they “feel funny” and passes out.
A colleague of LS carries a glucagon emergency kit and provides LS with a dose and calls 911. After 15 minutes, LS still hasn’t regained consciousness, so a second dose is administered. The paramedics arrive and check the glucose, it is 53.
Simply put, glucagon rescue medications may not work if the person drinks too much alcohol.
After reviewing the package inserts of all available US manufactured Glucagon Rescue Meds, there are no warnings for alcohol intake decreasing the effectiveness of glucagon rescue meds. So, I dug a little deeper and found a decent study on the topic which describes the impact of alcohol ingestion on glucose-regulating hormones.
I also found a very helpful monograph published by Lilly Baqsimi in Canada. Baqsimi is a powdered glucagon rescue medication that is delivered nasally. The Baqsimi monograph clearly states several warnings, “Alcohol can suppress hepatic gluconeogenesis and chronic alcoholism can deplete liver glycogen stores. Therefore BAQSIMI may be less effective in presence of acute or chronic alcohol ingestion. Alcohol-induced hypoglycemia is associated with a failure of blood glucose levels to rise normally after glucagon administration. BAQSIMI may not work if the person drinks too much alcohol.“.
Keeping it Real and Safe
In conclusion, having a conversation with people with type 1 about the suppressive nature of alcohol on glycogen release for many hours after consuming alcohol is very important. Another important teaching point is that glucagon rescue meds may not be as effective and timely in raising glucose to safe levels.
As a general rule of thumb, encouraging people with type 1 to eat 15gms of carbs with each drink and have a glass of water in between, may help make sure they have enough circulating carbs and slow the pace of alcohol consumption to help the liver with processing. They may also consider decreasing their insulin dose in association with alcohol intake to prevent this serious side effect.
Download our Glucagon Rescue Med PocketCard for more information here.
Whether you are new to diabetes or a seasoned expert, you’ll benefit from this virtual conference with the latest research plus critical content that you can immediately apply to your clinical practice.
Download Course Flyer | Download Schedule
If you are seeking a state-of-the-art review of current diabetes care, this course is for you. Our team has been fine-tuning this course for over fifteen years, and we know what you need. This program can also be a great addition to your CDCES or BC-ADM exam study plan.
Team of expert faculty includes:
Don’t worry if you can’t make it live. Your registration guarantees access to the recorded version in the Online University.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
RT is a 17-year-old with type 1 diabetes who uses an insulin pump and glucose meter to manage blood glucose levels. RT is out with friends, drinking beers and suddenly passes out. One of RT’s friends carries a glucagon rescue medication and administers it to RT in a panic.
Which of the following statements is most accurate?
Click Here to Test your Knowledge
This bundle is specifically designed for healthcare professionals who want to learn more about Specialty Topics for their clinical practice or for those who are studying for the Board Certified in Advanced Diabetes Management (BC-ADM) certification exam.
Previously recorded & available for on-demand viewing
All courses air at 11:30 a.m. (PST)
Coach Beverly Thomassian, RN, MPH, BC-ADM, CDCES
Author, Nurse, Educator, Clinician and Innovator, Beverly has specialized in diabetes management for over twenty years. As president and founder of Diabetes Educational Services, Beverly is dedicated to optimizing diabetes care and improving the lives of those with diabetes.
LS tells you that they frequently attend company mixers where they feel compelled to have at “least a few drinks”, to fit in and network.
The tricky part is that LS lives with type 1 diabetes. Since they don’t have a working pancreas, their circulating levels of insulin and glucagon are often mismatched to their body’s needs.
If LS has several drinks, then loses consciousness from hypoglycemia, will emergency treatment be effective?
There is emerging evidence that glucagon rescue medications may have a blunted response when ingesting alcohol.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.

This course will transform your test anxiety into calm self-confidence and test taking readiness.
Read More: Preparing for CDCES Exam Webinar Topics Preparing for the CDCES Exam |
FREE Webinar
Read More: What is a CDCES? First awarded in 1986, as Certified Diabetes Educator (CDE) credential and in 2020 with a new name: Certified Diabetes Care and Education Specialist (CDCES) to more accurately reflect the specialty. CDCES has become a standard of excellence for the delivery of quality diabetes education. Those who hold this certification are known to possess comprehensive knowledge of and experience in diabetes prevention, management, and prediabetes. “Becoming a Certified Diabetes Care and Education Specialist (CDCES) is one of the best professional and personal decisions I have ever made.” – Coach Beverly Thomassian, RN, MPH, CDCES, BC-ADM 
Read More: 3 Reasons to Become a CDCES “The best part of becoming a CDCES is working with my colleagues and people living with diabetes. As diabetes educators, we hear compelling and beautiful life stories. I am astounded by the barriers they face and inspired by their adaptability, problem-solving skills, and resilience.” Reason 1: CDCES is a widely recognized certification by employers and health care professionals throughout the U.S. This credential demonstrates a specialized and in-depth knowledge in the prevention and treatment of individuals living with pre-diabetes and diabetes. Reason 2: Currently, 10% of people in the U.S. have diabetes and another 35% have pre-diabetes which means 45% of Americans are running around with elevated blood glucose levels. Given this epidemic, there will be plenty of future job opportunities. Reason 3: Having my CDCES along with my nursing degree, has opened many doors of opportunity; from working as an inpatient Diabetes Nurse Specialist in a hospital to working as a Manager of Diabetes Education in the outpatient setting to starting my own consulting company.
This bundle includes our CDCES Online Prep Bundle (featured above) plus the ADCES Review Guide.
The online bundle includes Level 1, Level 2, and Level 3 (Boot Camp), plus two bonus courses. The ADCES Review Guide offers over 480+ practice questions and is a fantastic independent study tool and comprehensive resource for the Diabetes Care and Education Specialist Exam.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
August 2022 eNews | Diabetes Safety Update | Does Alcohol Blunt Glucagon Effectiveness?
Happy August
There is still time to celebrate warm summer nights before the days lengthen and get cooler. For people living with diabetes, summer parties, with their special treats and yummy drinks, can be complicated to navigate.
In our first article, we take a close look at the impact of alcohol on the effectiveness of glucagon rescue medications. As an educator for many years, I was not aware of alcohol’s impact on glucagon efficacy. Through increased knowledge, I am hopeful we can enhance the safety of people living with type 1 diabetes.
Our next article celebrates the abundance and deliciousness of summer fruit. Sadly, so often, people with diabetes are told not to eat fruit because it is “full of sugar.”
I reassure them that fruit is loaded with nutrients, fiber and decreases inflammation. In a new study, researchers highlight clear evidence that eating a portion of fruit is far better for our mental health than eating other sweet treats like cookies and snack foods. Plus, the study demonstrated that snacking on fruit not only boosts mood it can also improve cognition and decrease stress.
We also take a close look at the impact of those pesky dates on our food packaging. Almost 40% of food waste happens in our kitchen when consumers think food is too old to eat based on package dates. But, are we wasting food unnecessarily? Read more to gain clarity on what these dates signify. Let’s share this information with our communities to help decrease food waste and save money.
Lastly, we celebrate our special scholarship recipient, Judith, who recently earned her CDCES. Please join me in congratulating this dedicated, kind and enthusiastic individual.
We hope you enjoy our question and rationale of the week and we invite you to join our upcoming webinars and Virtual Conference.
Thank you in advance for your actions and advocacy on behalf of people living with diabetes.
Beverly, Bryanna, Robert, and Amanda
Featured Articles
Upcoming Webinars
ADCES Book Bundle
This course will transform your test anxiety into calm self-confidence and test taking readiness.
Read More: Preparing for CDCES Exam Webinar Topics Preparing for the CDCES Exam |
FREE Webinar
Read More: What is a CDCES? First awarded in 1986, as Certified Diabetes Educator (CDE) credential and in 2020 with a new name: Certified Diabetes Care and Education Specialist (CDCES) to more accurately reflect the specialty. CDCES has become a standard of excellence for the delivery of quality diabetes education. Those who hold this certification are known to possess comprehensive knowledge of and experience in diabetes prevention, management, and prediabetes. “Becoming a Certified Diabetes Care and Education Specialist (CDCES) is one of the best professional and personal decisions I have ever made.” – Coach Beverly Thomassian, RN, MPH, CDCES, BC-ADM
Read More: 3 Reasons to Become a CDCES “The best part of becoming a CDCES is working with my colleagues and people living with diabetes. As diabetes educators, we hear compelling and beautiful life stories. I am astounded by the barriers they face and inspired by their adaptability, problem-solving skills, and resilience.” Reason 1: CDCES is a widely recognized certification by employers and health care professionals throughout the U.S. This credential demonstrates a specialized and in-depth knowledge in the prevention and treatment of individuals living with pre-diabetes and diabetes. Reason 2: Currently, 10% of people in the U.S. have diabetes and another 35% have pre-diabetes which means 45% of Americans are running around with elevated blood glucose levels. Given this epidemic, there will be plenty of future job opportunities. Reason 3: Having my CDCES along with my nursing degree, has opened many doors of opportunity; from working as an inpatient Diabetes Nurse Specialist in a hospital to working as a Manager of Diabetes Education in the outpatient setting to starting my own consulting company.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.