
Subscribe
eNewsletter
Ready to get certified?
Free CDCES Coach App
eNewsletter
Free CDCES Coach App
RJ is in the hospital for the 3rd time this year in DKA. You ask RJ to complete the diabetes distress survey tool and immediately recognize that RJ is experiencing high levels of diabetes distress.
When working with RJ to assess what is happening, which of the following approaches could be used as a conversational tool?
Click Here to Test your Knowledge
Whether you are a novice or an expert in providing diabetes care, we invite you to attend this exciting training program that provides the essential steps to address diabetes distress combined with an innovative approach to glucose management that will revolutionize your practice.
“ReVive 5” breathes new life into our relationship with diabetes, bringing a fresh perspective to both the person with with diabetes and the provider.
By addressing old habits that no longer serve us, we have the opportunity to create a new life tool kit toolkit in partnership with the person living with diabetes.
The ReVive 5 program is built on sound research and will revolutionize your approach to diabetes self-management education.
Team of Experts:
ReVive 5 is taught by a team of 3 Interdisciplinary Experts:
Training Program Includes:
Don’t worry if you can’t make it live. Your registration guarantees access to the recorded version in the Online University.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
The content of this newly published guideline is thoughtful, person-centered, and offers a clear clinical path for the management of type 2 diabetes. I tip my hat to the authors in gratitude for their dedication and vision.
Besides having lots of attractive infographics and a fantastic summary of the research, this guideline offers evidence-based strategies to get glucose to the goal with an emphasis on taking a person-centered approach to pharmacologic and lifestyle interventions. We invite you to enjoy a detailed review by joining our webinar or reading this brief summary of the findings that impressed me most.
There is so much more to this article. I hope I have inspired you to read the complete ADA/EASD Consensus document or join our webinar on December 1st to learn more.

Plan on joining this exciting webinar that walks participants through the newly released, “Management of Hyperglycemia in Type 2 Consensus Report by the ADA and EASD”. These updated guidelines will be incorporated into the 2023 ADA Standards of Care, but you can get a early sneak peak by joining Coach Beverly on December 1st, 2022. She will highlight the revised guidelines with a focus on new elements and exciting changes on how we approach medication management for type 2 diabetes. Together, we will explore clinical factors to consider when determining the best strategy to improve glucose management in people with type 2 diabetes and other co-conditions. There will be a special focus on cardiovascular risk reduction and renal protection and addressing clinical inertia.
Objectives:
Intended Audience: A great course for health care professionals seeking evidence-based information that improves the quality of life and outcomes.
Don’t worry if you can’t make it live. Your registration guarantees access to the recorded version in the Online University.
All hours earned count toward your CDCES and BC-ADM Exam Accreditation Information

For last week’s practice question, we quizzed test takers on the best action before starting Tirzepatide (Mounjaro). 67% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question:
AR is 36 years old with type 2 diabetes and a BMI of over 40. Current A1C 7.9%, UACR less than 30, and GFR more than 60. Current diabetes medications include metformin, sitagliptin, and empagliflozin at maximum doses. AR is prescribed the new dual incretin tirzepatide (Mounjaro) to help improve glucose levels and support weight loss.
Before starting tirzepatide (Mounjaro), what action do you recommend to the provider?
Answer Choices:
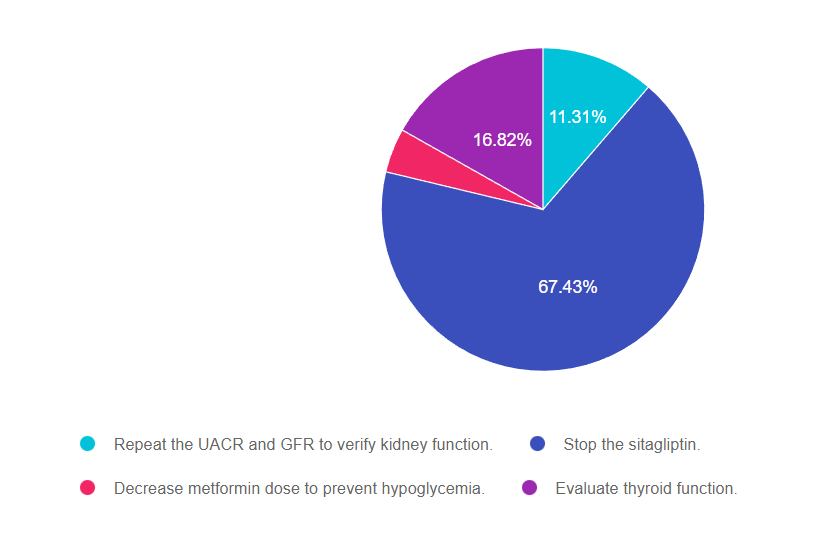
Answer 1 is incorrect. 11.31% chose this answer, “Repeat the UACR and GFR to verify kidney function.” This is not the best answer because JR has great kidney function, evidenced by a normal UACR and GFR. So we do not need to recheck kidney function before starting this new dual incretin tirzepatide (Mounjaro).
Answer 2 is correct. 67.43% of you chose this answer, “Stop the sitagliptin.” YES, this is the best answer. The American Diabetes Association (ADA) and American Association of Clinical Endocrinologists recommend against combination therapy with a DPP4-inhibitor and a GLP-1 RA due to the lack of evidence that this strategy is beneficial. Initial research combining the two classes, reflect a negligible glucose lowering effect when GLP-1’s and DPP-4’s are combined. Given the approximate average wholesale price for the DPP-4 inhibitor of $434 and GLP-1 RA of $887, using both simultaneously is not cost effective or clinically beneficial.
Answer 3 is incorrect. 4.4.% of respondents chose this answer, “Decrease metformin dose to prevent hypoglycemia.” No need to decrease the metformin dose, since JR is not on any medication class that will cause hypoglycemia.
Finally, Answer 4 is incorrect. 16.82% chose this answer, “Evaluate thyroid function.” This class of medication is not recommended for any person with a history of medullary thyroid tumor. However, we don’t need to draw a TSH to see if this medication is safe, we would simply do a careful history to see if there is a family history of medullary thyroid tumor.
Thank you so much for reading this “Rationale of the Week”. You can download our Medication PocketCard below, for more information.
We have just added this novel, first in class, dual incretin hormone therapy, Tirzepatide (Mounjaro), to our printed version of our Diabetes Medication PocketCard.
This new twin therapy includes not only a GLP-1 Receptor Agonist, but also a Glucose-dependent insulinotropic polypeptide (GIP), which magnifies the therapeutic effectiveness. The SURPASS studies indicate that study participants experienced an A1C drop of up to 2.5% and weight loss of up to 10kg or more.
The FDA just authorized the Insulet Omnipod 5 tubeless insulin delivery system for pediatrics with type 1 diabetes starting as young as age 2. This remarkable moment marks the availability of the world’s first tubeless, wearable insulin delivery system for toddlers.
The Omnipod 5 received FDA approval earlier this year for integration with the Dexcom G6 continuous glucose monitor for adults and kids with type 1, but Insulet also petitioned the FDA to approve this technology for toddlers.
This first tubeless hybrid closed loop system to receive FDA authorization includes the Omnipod 5, Dexcom G6 CGM and a phone app or controller to manage insulin delivery and monitor glucose levels. The Omnipod holds three days worth of insulin in a pod delivery device without the need for tubing, which can be helpful for active toddlers. No calibration or fingersticks are required.
As a hybrid loop system, the Omnipod and Dexcom are continuously data sharing, so most of the insulin delivery is automated. However, users can make needed adjustments, deliver bolus insulin and easily share data with the smartphone app or Ominpod 5 Controller.
Based on a study presented at the annual ADA Scientific Session, children with type 1 diabetes experienced a drop in A1C levels from a baseline of 7.4% to 6.9% and they remained at this improved A1C level for one year into the study. Time in range also increased from 57% at baseline to 68% after using the Omnipod 5 for three months. In addition, there were no reported cases of DKA or severe hypoglycemia. For more information on the latest in insulin pumps and CGMs, please join our Virtual Conference with technology expert Diana Issacs. In addition to explaining the technology, she provides an awesome “show and tell”.
On a related note, I would like to give recognition to the courageous Lila Grace Moss, who lives with type 1 diabetes. On a recent runway show, she did not shy away from wearing her Omnipod as she modeled the latest fashion styles with camera’s clicking and hundreds of audience members.
Social media took note and many instagram followers thanked Lila for her bold and brave statement.
Thanks Lila!
Whether you are new to diabetes or a seasoned expert, you’ll benefit from this virtual conference with the latest research plus critical content that you can immediately apply to your clinical practice.
Download Course Flyer | Download Schedule
If you are seeking a state-of-the-art review of current diabetes care, this course is for you. Our team has been fine-tuning this course for over fifteen years, and we know what you need. This program can also be a great addition to your CDCES or BC-ADM exam study plan.
Team of expert faculty includes:
Don’t worry if you can’t make it live. Your registration guarantees access to the recorded version in the Online University.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
JT has type 1 diabetes and tells you they are avoiding carbs and trying to eat less than 30gms of carbs daily. JT is 76 years old, with an A1C of 6.6% and a BMI of 22.
What is the best response?
Click Here to Test your Knowledge
Whether you are a novice or an expert in providing diabetes care, we invite you to attend this exciting training program that provides the essential steps to address diabetes distress combined with an innovative approach to glucose management that will revolutionize your practice.
“ReVive 5” breathes new life into our relationship with diabetes, bringing a fresh perspective to both the person with diabetes and the provider.
By releasing old habits that no longer serve us, we have the opportunity to create a new life tool kit toolkit in partnership with the person living with diabetes.
The ReVive 5 program is built on international research study results and will revolutionize your approach to diabetes self-management education.
Team of Experts:
ReVive 5 is taught by a team of 3 Interdisciplinary Experts:
Accredited Training Program:
Dates and Times for ReVive Virtual Training
Don’t worry if you can’t make it live. Your registration guarantees access to the recorded version in the Online University.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
The Diabetes Educator Flower Scholarship is awarded to 2 individuals each year. This scholarship awards two deserving applicants the opportunity to attend our DiabetesEd Specialist Virtual Conference on October 12-14, 2022 free of charge. This gift of recognition is donated by a generous diabetes nurse specialist who believes that the health of our future depends on supporting diabetes educators in providing care in underserved communities.
The Flower Scholarship’s vision is to increase diversity in the diabetes education workforce by supporting diabetes nurse educators who come from underserved communities.
It is always a very difficult decision for all of the judges. We read each application in careful detail considering the applicant’s impact on underserved communities, building bridges to improve access, volunteerism, financial need and readiness to take the CDCES exam. Read more about Ms. Owens and Ms. Hillman below.

Janeka Owens is a recipient of our “Flower Scholarship” because of her belief that “Diversity and representation matter in diabetes education”. She turns this belief into action in her work as a Nurse Educator in a hospital and in an outpatient Population Health Department in Pensacola, Florida. In addition to providing individual education, Janeka also provides group classes to both insured and uninsured individuals. She assists with hospital discharges and care management for individuals experiencing food and medical insecurity and makes sure they are connected with community health centers to receive ongoing care. Janeka goes on to say that, “representation is important to improve outcomes, build stronger communities and overall restore trust in health care”. Thank you, Janeka, for being a trusted health care provider and advocating to improve access to diabetes self-management and support programs for your community members.

Patricia Hillman is also a Flower Scholarship Recipient. She provides diabetes care at a federally qualified health center in an underserved community. Many of the people she serves have no insurance and struggle to manage their diabetes. Patricia works directly with her Maternal/Fetal physician to co-manage people during pregnancy and often follows up with high-risk individuals on weekends. Many of the clients she serves, have limited resources, and lack insurance coverage. Patricia goes out her way to make sure they have needed resources and that they can easily access her with questions and concerns. Patricia has created a library of information in English, Spanish and Creole to meet community needs and create bridges of understanding. She often accompanies those who have not yet learned English to the pharmacy to assist with language barriers and ensure they get the supplies they need. Patricia plans to apply the knowledge garnered from the course to continue empowering her community.
Congratulations to Janeka and Patricia. You both are Flower Scholarship Recipients!

Without reading any scientific papers, we intuitively know that we just feel better after moving. Humans are designed for motion interspersed with periods of rest. However, while activities like yoga, walking, or swimming may give us a boost of energy, are there specific exercises that will actually make you feel happy?
What activities not only crank up our heart rate, improve muscle strength and flexibility while also bringing us feelings of JOY?
Researchers have identified specific movements that exist across cultures that inspire joy.
I did my own study with an “n” of 1. I rated my joy feelings on a scale of 1-10 (and pulse) before doing these seven activities that each last for one minute. My joy rating was about a 3 before and it easily jumped up to an 8 during the movements and I couldn’t help but spontaneously smile. Plus, the glow continued afterward. Those 8 minutes of joy movement gave me the extra mental boost I needed to finish this blog post on a busy Monday morning,
Try it for yourself. Commit eight minutes out of your day to try this simple body joy workout. Invite your friends and family to compare their “joy” before and after doing these movements.
The American Diabetes Association recommends that people with prediabetes and diabetes get up and move every half hour. This joy workout offers a starting point to begin a new habit of moving more. Of course, individuals may need to modify some of the moves for safety and comfort. If doing it all at once is too much, a person could spread the workout throughout the day, doing one move at each half hour break. Even turning on the music for a few minutes and spontaneously dancing invokes joy and improves health.
You are invited to choose your favorite beat or just enjoy the music on the Joy Workout Video (from Newsweek article).
Consider this as an experiment and an invitation to rediscover the joy of movement. There are plenty of other science-backed ways to improve your mood with exercise and these exercises may just be the start.
Whether you are new to diabetes or a seasoned expert, you’ll benefit from this virtual conference with the latest research plus critical content that you can immediately apply to your clinical practice.
Download Course Flyer | Download Schedule
If you are seeking a state-of-the-art review of current diabetes care, this course is for you. Our team has been fine-tuning this course for over fifteen years, and we know what you need. This program can also be a great addition to your CDCES or BC-ADM exam study plan.
Team of expert faculty includes:
Don’t worry if you can’t make it live. Your registration guarantees access to the recorded version in the Online University.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
For last week’s practice question, we quizzed test takers on DKA. Only 53% of respondents chose the best answer, which indicates that there was some uncertainty. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question:
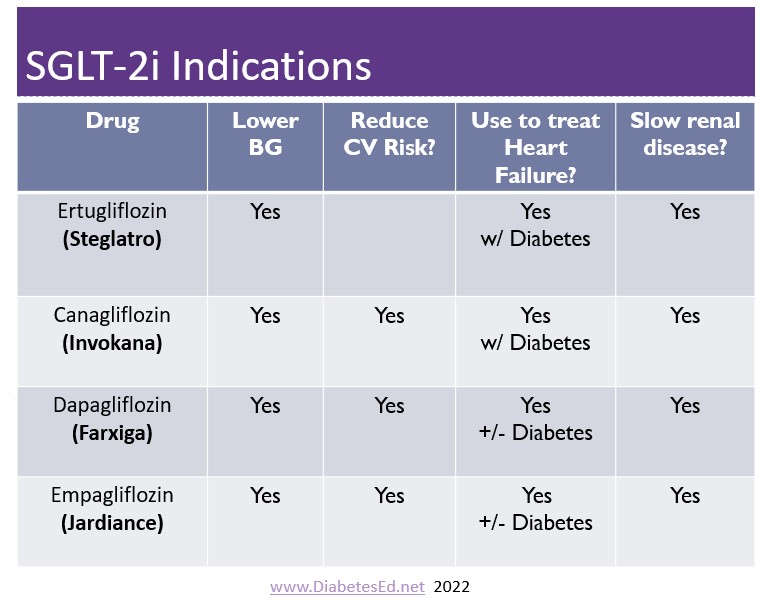
JR, a 67-year-old with type 2 diabetes for seven years and an A1C of 9.7% was started on empagliflozin 10mg two weeks ago. Other labs include a GFR of 49 and a UACR of 34 mg/g. Other diabetes medications include glucotrol 10mg twice daily and sitagliptin 100mg daily. JR sometimes has a few shot’s of whiskey before bed, especially if they had a stressful day. JR’s partner calls you in a panic and says JR is admitted to the hospital in DKA.
What is the most likely explanation?
Answer Choices:
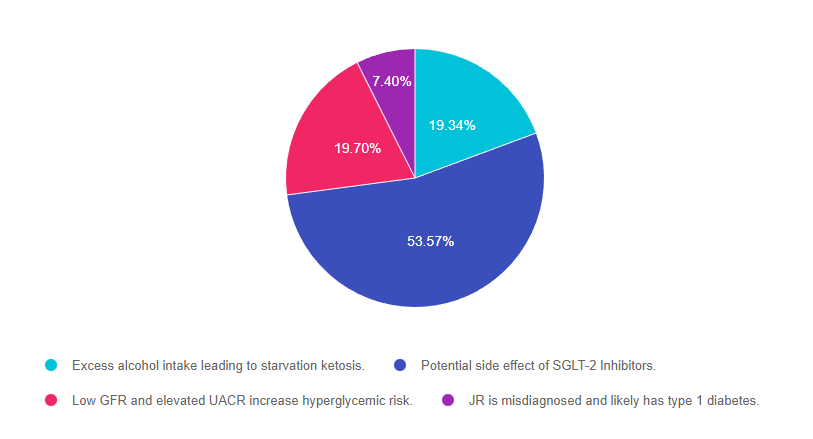
Answer 1 is incorrect. 19.34% chose this answer, “Excess alcohol intake leading to starvation ketosis.” Although this answer is tempting, it is not the best answer. According to the vignette, “JR sometimes has a few shot’s of whiskey before bed, especially if they had a stressful day”. The American Diabetes Association states that women can have 1 drink a day and men can have up to 2 drinks a day. Given that JR only seems to drink a few shots when stressed out, this would not be considered excess alcohol intake associated with malnutrition.
Answer 2 is correct. 53.57% of you chose this answer, “Potential side effect of SGLT-2 Inhibitors.” YES, great job choosing the best answer. The SGLT’s have been associated with a rare but serious adverse drug effect called euglycemic diabetic ketoacidosis (DKA). This seems to be more likely if the person is on insulin and decreased their insulin dose in response to lower blood sugars from the addition of a SGLT-2. However, DKA can also happen to people started on SGLT-2s who are not taking insulin. People taking this class of medication need to be aware of the signs of DKA and appropriate action.
Answer 3 is incorrect. 19.70% of respondents chose this answer, “Low GFR and elevated UACR increase hyperglycemic risk.” With a GFR of 49 and a UACR of 34 mg/g, JR is a perfect candidate for the SGLT-2 Inhibitor class of medication. This class of medication preserves renal function while lowering A1C. JR’s GFR is well above the cut-off point and JR is not at increased risk of hyperglycemia.
Finally, Answer 4 is incorrect. 7.40% chose this answer, “JR is misdiagnosed and likely has type 1 diabetes.” Although it is possible that this is true, it is unlikely. JR has a 7 year history of type 2 with a moderately increased A1C on oral medications only. If JR had type 1 diabetes, the A1C would certainly be more elevated, since glucotrol 20mg and sitagliptin 100mg daily, would not be effective without a semi-functional pancreas. JR might have latent autoimmune diabetes in adults, so checking the GAD, ICA and IAA for autoimmunity could be enlightening.
For a listing of diabetes medications, side effects and considerations, please download our PocketCards
Whether you are new to diabetes or a seasoned expert, you’ll benefit from this virtual conference with the latest research plus critical content that you can immediately apply to your clinical practice.
Download Course Flyer | Download Schedule
If you are seeking a state-of-the-art review of current diabetes care, this course is for you. Our team has been fine-tuning this course for over fifteen years, and we know what you need. This program can also be a great addition to your CDCES or BC-ADM exam study plan.
Team of expert faculty includes:
Don’t worry if you can’t make it live. Your registration guarantees access to the recorded version in the Online University.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
