Subscribe
eNewsletter
Ready to get certified?
Free CDCES Coach App
eNewsletter
Free CDCES Coach App
Setting realistic person-centered goals is a critical part of providing diabetes education care and support. We have created a goal sheet that you can use in your practice to capture the next steps toward improving self-care.
You can customize this sheet with your logo and contact information or just download and print the PDF to get started. No permission is needed. We are delighted to share these sheets with you.
Taking on a new behavior is not easy.
By careful coaching, we can help participants create goals that are REALLY achievable and important to the individual.
For example, someone says they want to “eat more healthfully”, then we can ask, “What would that look like for you?”. They might reply, “I want to eat for more fruits and vegetables instead of junk food”. To get more specific, we can discuss how many servings of fruit and vegetables a day do they think would be realistic? We can encourage individuals to start with one to two servings a day and gradually increase portions as the person gains more confidence in their ability.
To help build success, we may want to emphasize that is doesn’t matter whether people consume fresh, frozen or canned fruits and vegetables. They all offer similar nutrient values. The main consideration is highlighting affordable and appealing fruits and veggies based on the individuals’ taste and preferences.
This simple goal sheet can help capture the negotiated goals and follow-up care activities. This checklist of activities can also be reminders for us to discuss eye and foot care, plus oral hygiene and vaccinations too.
Learn Test-Taking Secrets with Coach Bev – Option to add on 200+ Computerized Practice Test Questions for $49
During this webinar, Coach Beverly will help you transform your nervousness into focused energy that will help you succeed. She will provide test-taking tips based on her experience taking the certification exam six times.
To provide plenty of practice, Coach Beverly will sample 20 test questions that have been plucked from our Test Taking Toolkit during this live webinar.
She will explain how to dissect the question, eliminate wrong answers and avoid getting lured in by juicy answers.
Includes a review of 20 sample test questions with test taking strategies.
This includes access to the recorded version of this webinar on your Online University Student Portal.
Plus, the Test Taking Toolkit provides you with over 200+ sample online practice questions, simulating the exam experience.
A perfect way to assess your knowledge and create a focused study plan, while increasing your test-taking confidence.
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.

For last week’s practice question, we quizzed test takers on MR who was recently diagnosed with diabetes at age 13. 70% of respondents chose the best answer. We want to share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question: MR is 13 years old, and went to urgent care because they weren’t feeling well and told the Provider “I feel so tired all the time and I have to go the bathroom a lot”. The provider draws labs and gets a urine sample. The A1C is 8.7% with some ketones in the urine. The antibody results aren’t back yet. Based on the ADA Standards and this information, what is the best action?
Answer Choices:
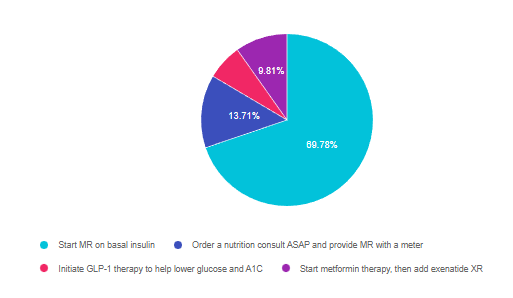
As shown above, the most common choice was option 1, the second most common answer was option 2, then option 4, and finally 3.
Answer 1 is correct. 69.78% chose this answer, “Start MR on basal insulin.” YES, GREAT JOB. This is the best answer according to ADA Standard 14 on Diabetes and Youth. If a person under the age of 18 has new-onset diabetes and an A1C of 8.5% or greater, basal insulin is needed to get blood glucose to target and stop ketosis. The next step is to determine if they have immune-mediated diabetes by evaluating their autoantibodies. If they don’t have autoantibodies (GAD, ICA, IAA), then the guidelines suggest starting metformin and gradually decreasing the insulin to see if they can be managed on metformin alone or with the addition of a GLP-1 RA. If the antibodies come back positive, MR would need to be managed on basal-bolus insulin therapy.
Answer 2 is incorrect. 13.71% of you chose this answer, “Order a nutrition consult ASAP and provide MR with a meter.” This is a juicy answer since a nutrition consult and meter are critical to managing a new diabetes diagnosis. However, we would provide the nutrition consult after we figure out what type of diabetes and after lowering blood glucose levels with insulin to prevent a hyperglycemic crisis. Regardless of the type of diabetes, ordering a meter right away and providing basic nutrition guidelines are both critical steps to keep MR safe and to evaluate treatment response.
Answer 3 is incorrect. 6.70% of respondents chose this answer, “Initiate GLP-1 therapy to help lower glucose and A1C.” Since the A1C is above 8.5%, the ADA Standards state to start basal insulin to lower glucose and prevent hyperglycemic crises. If the autoantibodies come back negative, we would start metformin therapy and consider a GLP-1 RA as a future add-on therapy.
Finally, Answer 4 is incorrect. 9.81% chose this answer, “Start metformin therapy, then add exenatide XR if needed.” Since the A1C is above 8.5%, the ADA Standards state to start basal insulin to lower glucose and prevent a hyperglycemic crisis. If the autoantibodies come back negative, we would start metformin therapy and consider a GLP-1 RA as a future add-on therapy.
Learn Test-Taking Secrets with Coach Bev – Option to add on 200+ Computerized Practice Test Questions for $49
During this webinar, Coach Beverly will help you transform your nervousness into focused energy that will help you succeed. She will provide test-taking tips based on her experience taking the certification exam six times.
To provide plenty of practice, Coach Beverly will sample 20 test questions that have been plucked from our Test Taking Toolkit during this live webinar.
She will explain how to dissect the question, eliminate wrong answers and avoid getting lured in by juicy answers.
Includes a review of 20 sample test questions with test-taking strategies.
This includes access to the recorded version of this webinar on your Online University Student Portal.
Plus, the Test Taking Toolkit provides you with over 200+ sample online practice questions, simulating the exam experience.
A perfect way to assess your knowledge and create a focused study plan, while increasing your test-taking confidence.
This course includes updated goals and guidelines for children living with type 1 or type 2 diabetes. This course discusses the special issues diabetes educators need to be aware of when working with children with diabetes and their families. We discuss the clinical presentation of diabetes, goals of care, and normal growth and development through the early years through adolescence. Strategies to prevent acute and long term complications are included with an emphasis on positive coping for family and child with diabetes.
Objectives:
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
In health care settings across the country, people with diabetes and providers have been asking if intermittent fasting is effective at helping with weight loss. Finally, a randomized outpatient study provides some answers so we can accurately respond to this frequently asked question.
According to a recent study published in The New England Journal of Medicine, “a regimen of time-restricted eating was not more beneficial with regard to reduction in body weight, body fat, or metabolic risk factors than daily calorie restriction.”
In this study, 139 participants were randomized into two groups. Both groups were placed on a limited calorie diet. Men in the study were limited to a 1500 to 1800 kcal per day diet while women were limited to a 1200 to 1500 kcal per day diet.
The main difference, was the eating time frame.
The intermittent fasting group ate their calorie-restricted diet between the limited hours of 8:00 am to 4:00 pm. Which is a fasting period of 16 hours and an eating window of 8 hours.
The control group also followed the calorie restrictions but could eat their assigned calories at whatever time.
Results After One Year
After a 12-month period of following these diets, each group was evaluated for changes in body weight, body fat, waist circumference, body-mass index (BMI), and metabolic risk factors. 85% of participants completed the trial.
The participants in the time-restricted group had a mean weight loss from baseline of -8.0 kg while the calorie restriction only group had a 6.3 kg mean weight loss from baseline. While the time-restricted group had a higher weight loss, it wasn’t enough to reach statistical significance.
Additionally, there were no statistically significant changes in waist circumference, body fat, body lean mass, BMI, blood pressure, and other metabolic risk factors between the two groups.
The conclusion is that time-restricted eating was not significantly beneficial in weight loss in comparison to following a calorie-restricted diet.
To read more, click here.
LS wears an insulin pump and uses lispro insulin. LS has an average basal rate of 0.6 units and hour, a 1:15 carb ratio and a 1:50 correction ratio. Based on the ambulatory glucose profile, LS is experiencing elevated glucose levels from 4am to 7am. To get glucose to target, what is the best next step?
Click Here to Test your Knowledge
Learn Test-Taking Secrets with Coach Bev – Option to add on 200+ Computerized Practice Test Questions for $49
During this webinar, Coach Beverly will help you transform your nervousness into focused energy that will help you succeed. She will provide test-taking tips based on her experience taking the certification exam six times.
To provide plenty of practice, Coach Beverly will sample 20 test questions that have been plucked from our Test Taking Toolkit during this live webinar.
She will explain how to dissect the question, eliminate wrong answers and avoid getting lured in by juicy answers.
Includes a review of 20 sample test questions with test taking strategies.
This includes access to the recorded version of this webinar on your Online University Student Portal.
Plus, the Test Taking Toolkit provides you with over 200+ sample online practice questions, simulating the exam experience.
A perfect way to assess your knowledge and create a focused study plan, while increasing your test-taking confidence.
Whether you are new to diabetes or a seasoned expert, you’ll benefit from this virtual conference with the latest research plus critical content that you can immediately apply to your clinical practice.
Download Course Flyer | Download Schedule
If you are seeking a state-of-the-art review of current diabetes care, this course is for you. Our team has been fine-tuning this course for over fifteen years, and we know what you need. This program can also be a great addition to your CDCES or BC-ADM exam study plan.
Join us LIVE for this Virtual Course and enjoy a sense of community!
Team of expert faculty includes:
Deluxe Option for $499: Virtual Program includes:
Deluxe Version includes Syllabus, Standards and Swag*:
Basic Option for $399: Virtual Program includes:
Don’t worry if you can’t make it live. Your registration guarantees access to the recorded version in the Online University.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
For last week’s practice question, we quizzed test takers on fatty liver disease. 57% of respondents chose the best answer. We want to share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question: 45 to 75% of individuals with type 2 diabetes have non-alcoholic fatty liver disease (NAFLD). NAFLD has associated with an increased risk of steatohepatitis, cirrhosis, and liver cancer. Which of the following statements is true based on ADA Standards of Care?
Answer Choices:
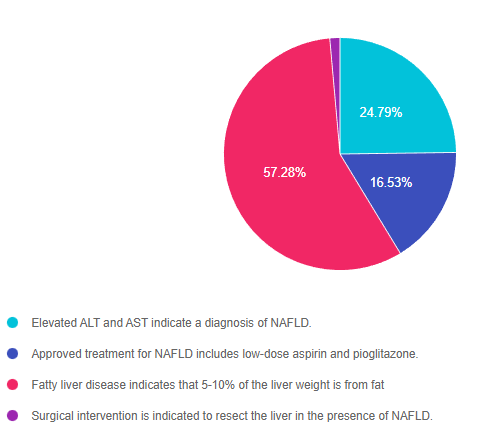
As shown above, the most common choice was option 3, the second most common answer was option 1, then option 2, and finally 4.
Answer 1 is incorrect. 24.79% chose this answer, “Elevated ALT and AST indicate a diagnosis of NAFLD.” These two liver enzyme tests certainly indicate liver inflammation and are a signal that further investigation is warranted. However, to confirm and diagnose NAFLD, a comprehensive review of patient history, lab results, liver imaging studies and possibly a biopsy are required.
Answer 2 is incorrect. 16.53% of you chose this answer, “Approved treatment for NAFLD includes low-dose aspirin and pioglitazone.” The cornerstones of treatment for NAFLD are nutrition therapy interventions with a focus on decreasing processed foods, sugary beverages and foods high in saturated fat. Plus, increasing intake of whole foods and committing to a structured physical activity plan to decrease visceral and hepatic adiposity is imperative. There is no officially approved medication to treat NAFLD, but pioglitazone and GLP-1 RA’s appear to decrease fatty liver based on current studies.
Answer 3 is correct. 57.28% of respondents chose this answer, “Fatty liver disease indicates that 5-10% of the liver weight is from fat.” GREAT JOB, this is the best answer. The good news is that weight loss and increased activity are very effective in treating fatty liver disease. A weight loss of 7-10% linked with a 50% drop in liver fat. Every pound lost makes a big difference. The cornerstones of treatment for NAFLD are nutrition therapy interventions with a focus on decreasing processed foods, sugary beverages and foods high in saturated fat. Plus, increasing intake of whole foods and committing to a structured physical activity plan to decrease visceral and hepatic adiposity is imperative.
Finally, Answer 4 is incorrect. 1.41% chose this answer, “Surgical intervention is indicated to resect the liver in the presence of NAFLD.” People with NAFLD and other risk factors, have an increased risk of disease progression to cirrhosis and liver cancer, which might require surgical intervention. However, no surgical intervention is warranted for NAFLD. The cornerstones of treatment for NAFLD are nutrition therapy interventions with a focus on decreasing processed foods, sugary beverages and foods high in saturated fat. Plus, increasing intake of whole foods and committing to a structured physical activity plan to decrease visceral and hepatic adiposity is imperative.
Learn Test-Taking Secrets with Coach Bev – Option to add on 200+ Computerized Practice Test Questions for $49
During this webinar, Coach Beverly will help you transform your nervousness into focused energy that will help you succeed. She will provide test-taking tips based on her experience taking the certification exam six times.
To provide plenty of practice, Coach Beverly will sample 20 test questions that have been plucked from our Test Taking Toolkit during this live webinar.
She will explain how to dissect the question, eliminate wrong answers and avoid getting lured in by juicy answers.
Includes a review of 20 sample test questions with test taking strategies.
This includes access to the recorded version of this webinar on your Online University Student Portal.
Plus, the Test Taking Toolkit provides you with over 200+ sample online practice questions, simulating the exam experience.
A perfect way to assess your knowledge and create a focused study plan, while increasing your test-taking confidence.
Whether you are new to diabetes or a seasoned expert, you’ll benefit from this virtual conference with the latest research plus critical content that you can immediately apply to your clinical practice.
Download Course Flyer
If you are seeking a state-of-the-art review of current diabetes care, this course is for you. Our team has been fine-tuning this course for over fifteen years, and we know what you need. This program can also be a great addition to your CDCES or BC-ADM exam study plan.
Join us LIVE for this Virtual Course and enjoy a sense of community!
Team of expert faculty includes:
Deluxe Option for $449: Virtual Program includes:
Deluxe Version includes Syllabus, Standards and Swag*:
Don’t worry if you can’t make it live. Your registration guarantees access to the recorded version in the Online University.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
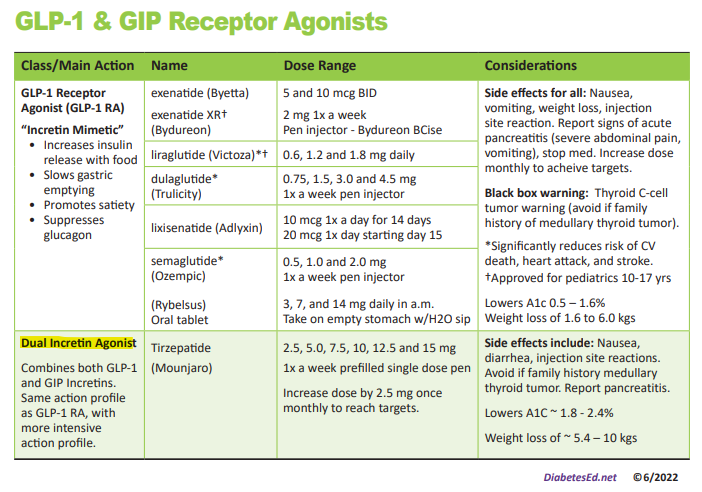
We have just added this novel, first in class, dual incretin hormone therapy, Tirzepatide (Mounjaro), to our printed version of our Diabetes Medication PocketCard.
This new twin therapy includes not only a GLP-1 Receptor Agonist, but also a Glucose-dependent insulinotropic polypeptide (GIP), which magnifies the therapeutic effectiveness. The SURPASS studies indicate that study participants experienced an A1C drop of up to 2.5% and weight loss of up to 10kg or more.

Incretins (GLP-1 and GIPs) play a major role in glucose regulation post prandially. Incretins are gut hormones that stimulate insulin release from the pancreas when glucose rises in response to food ingestion. They keep blood sugars in check as well as activating the satiety center, to increase the sense of fullness. Incretins slow gastric emptying and also curb post-meal glucagon release, decreasing post prandial glucose spikes. Unfortunately, people with type 2 diabetes, make less than half of the usual amount of the GLP-1 and GIP hormones, which contributes to chronically elevated glucose levels.
To date, therapies that have only included the Glucagon-Like Peptide-1 (GLP-1) have demonstrated major success in managing Type 2 DM.
By creating a formulation with BOTH the GIP and GLP incretin hormones, the A1C lowering and weight loss effectiveness has been significantly amplified.
Tirzepatide is a novel synthetic peptide, engineered to provide a once-weekly injectable medication that acts on glucose-dependent insulinotropic polypeptide (GIP) and glucagon-like peptide-1 (GLP-1) receptors.
Tirzepatide has been granted FDA approval for treatment of type 2 diabetes based primarily on a series of trials known as SURPASS. The SURPASS 1 trial compared increasing doses to evaluate dose response. The SURPASS 2-5 Trials compared tirzepatide to the GLP-1 semaglutide and to the basal insulins degludec and glargine. In all of the trials, the findings were impressive.
Summary of SURPASS Trials and Results based on Tirzepatide Package Insert.
This once a week injectable is for adults with type 2 diabetes as an adjunct to diet and exercise to improve glycemic control and support weight loss. Tirzepatide is delivered with a single dose prefilled pen.
Starting Dose: 2.5 mg SC every week for 4 weeks initially; THEN increase to 5 mg SC every week. If additional glycemic improvement is needed, increase by 2.5-mg increments after at least 4 weeks at current dose.
Note: The initial 2.5-mg dose is intended for treatment initiation and is not effective for glycemic control
Maximum dose: 15 mg SC qWeek
Common Adverse Side effects: Nausea, diarrhea, abdominal discomfort and injection site hypersensitivity reactions. There is also a black box warning to avoid if family history of medullary thyroid tumor and to report any signs of pancreatitis immediately.
Cost: Tirzepatide is comparably priced to other GLP-1 RAs on the market at $974.33 for four weekly doses, regardless of dose size. Hopefully, insurance companies will recognize the long term benefits of these newer classes of agents, and increase coverage of these beneficial treatment options.
In conclusion: This new medication class substantially lowers blood sugars and body weight, with a once a week injection. Coupled with healthy eating and keeping active, people with diabetes have the opportunity to improve their health and quality of life with this novel medication class.
Author’s note: Beverly Thomassian has no conflict of interest to report and distilled the content of this article from the SURPASS study results and the tirzepatide package insert.
*PocketCardsTM are for individual use only.
MR is 13 years old, and went to urgent care because they weren’t feeling well and told the Provider “I feel so tired all the time and I have to go the bathroom a lot”. The provider draws labs and gets a urine sample. The A1C is 8.7% with some ketones in the urine. The antibody results aren’t back yet. Based on the ADA Standards and this information, what is the best action?
Click Here to Test your Knowledge
Learn Test-Taking Secrets with Coach Bev – Option to add on 200+ Computerized Practice Test Questions for $49
During this webinar, Coach Beverly will help you transform your nervousness into focused energy that will help you succeed. She will provide test-taking tips based on her experience taking the certification exam six times.
To provide plenty of practice, Coach Beverly will sample 20 test questions that have been plucked from our Test Taking Toolkit during this live webinar.
She will explain how to dissect the question, eliminate wrong answers and avoid getting lured in by juicy answers.
Includes a review of 20 sample test questions with test taking strategies.
This includes access to the recorded version of this webinar on your Online University Student Portal.
Plus, the Test Taking Toolkit provides you with over 200+ sample online practice questions, simulating the exam experience.
A perfect way to assess your knowledge and create a focused study plan, while increasing your test-taking confidence.
This course includes updated goals and guidelines for children living with type 1 or type 2 diabetes. This course discusses the special issues diabetes educators need to be aware of when working with children with diabetes and their families. We discuss the clinical presentation of diabetes, goals of care, and normal growth and development through the early years through adolescence. Strategies to prevent acute and long term complications are included with an emphasis on positive coping for family and child with diabetes.
Objectives:
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
We are excited to announce the FDA approval of a novel dual incretin injectable. The SURPASS clinical trials confirm this new diabetes medication not only drops A1C, but also contributes to significant weight loss. We have updated the electronic versions of our Medication PocketCards to include this “first in class” therapy. You can read more in our article below.
June also celebrates Pride Month. Members of the LGBTQ+ community often suffer worse health outcomes and may avoid seeking needed health care due to discrimination or discomfort within the current health care model. We explore strategies to increase inclusion and embrace diversity in diabetes care and beyond.
Our next article explores if intermittent fasting results in weight loss. We highlight the findings of a recently published randomized trial that provides some unexpected findings.
Lastly, we are excited to share a bunch of free resources and webinars with you. You can download our new diabetes self-care cheat sheet in Spanish, plus join us for 3 Free Webinars. These free courses with Coach Beverly include Test Taking Success, CDCES, and BC-ADM Prep Webinars.
Don’t forget to check out our Question and Rationale of the week. We think you will find them interesting and informative. We also love sharing this picture of Amanda, our Logistics Assistant, holding a colorful bundle of newly finished pancreas partners
We thank you for being a light to people living with diabetes. You are touching the lives of many through your care!
Beverly, Bryanna, Jackson, and Amanda
Featured Articles
Upcoming FREE Webinars
Featured Items
Learn Test-Taking Secrets with Coach Bev – Option to add on 200+ Computerized Practice Test Questions for $49
During this webinar, Coach Beverly will help you transform your nervousness into focused energy that will help you succeed. She will provide test-taking tips based on her experience taking the certification exam six times.
To provide plenty of practice, Coach Beverly will sample 20 test questions that have been plucked from our Test Taking Toolkit during this live webinar.
She will explain how to dissect the question, eliminate wrong answers and avoid getting lured in by juicy answers.
Includes a review of 20 sample test questions with test taking strategies.
This includes access to the recorded version of this webinar on your Online University Student Portal.
Plus, the Test Taking Toolkit provides you with over 200+ sample online practice questions, simulating the exam experience.
A perfect way to assess your knowledge and create a focused study plan, while increasing your test-taking confidence.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.