
Subscribe
eNewsletter
Ready to get certified?
Free CDCES Coach App
eNewsletter
Free CDCES Coach App

For last week’s practice question, we quizzed test takers on abdominal lumps and insulin injections. Only 46% of respondents chose the best answer, which indicates that there was some confusion. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question:
JL is 67 years old, with a BMI of 23 and A1C of 7.6% and injects insulin 4 times a day to manage their type 1 diabetes. On visual inspection, you notice that there are many areas of lipohypertrophy on JL’s abdominal region.
Which of the following interventions would be the best recommendation?
Answer Choices:
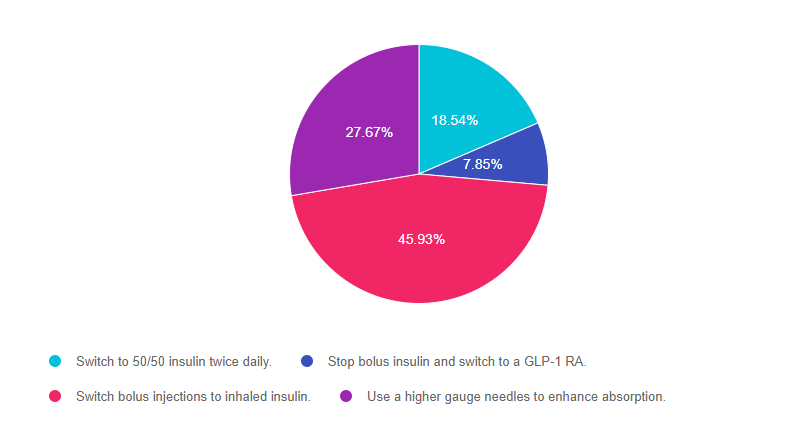
Answer 1 is incorrect. 18.54% chose this answer, “Switch to 50/50 insulin twice daily.” This is not the best answer since it doesn’t address the core issue of injection site overuse and fat accumulation. Switching to 50/50 insulin may even lead to worsening blood sugars since it is a premixed basal bolus insulin that would be difficult to fine tune for people with type 1 diabetes. (See photo of lipohypertrophy below)
Answer 2 is incorrect. 7.85% of you chose this answer, “Stop bolus insulin and switch to a GLP-1 RA.” This is not the best answer since GLP-1 RA’s are not FDA approved to treat people with type 1 diabetes*. If a person with type 1 diabetes stopped their bolus insulin, they would become very insulin deprived and likely experience severe blood glucose elevations and hyperglycemic crisis. Plus, this answer doesn’t address the core issue of injection site overuse and fat accumulation. *Footnote: some people with type 1 are prescribed a GLP-1 RA (off label) in ADDITION to basal bolus insulin to lower glucose levels and help with weight management. (See photo of lipohypertrophy below)
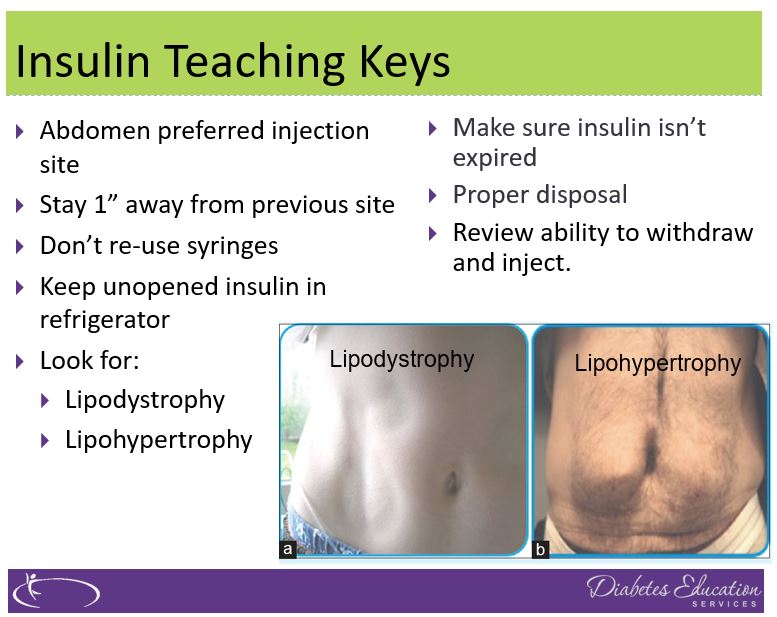
Answer 3 is correct. 45.93% of respondents chose this answer, “Switch bolus injections to inhaled insulin.” YES, GREAT JOB. Lipohypertrophy, a lump of fat accumulation due to frequent injections, has been shown to affect ?50% of people injecting insulin and results from lack of injection site rotation and needle. Injecting into these “lumps” reduces insulin absorption and action, raises postprandial glucose, and greatly increases insulin uptake variability. Despite this, inspection of injection sites is not routinely performed by health care professionals or people with diabetes, which reveals the “unexplained” nature of many blood glucose fluctuations. (Excerpted from this Article on Insulin Injection Technique- Clinical Diabetes, 2019).
To avoid lipohypertrophy, we can transition people to boluses of inhaled insulin to cover for food and hyperglycemia and still provide one basal injection a day, using sites free of fatty lumps. This reduction of the injection frequency allows time for tissue healing and reduces creation of new lipohypertrophy sites. Download our FREE Insulin PocketCards here.
If a person decides to stay on injections, encourage them to systematically space them at least 1 cm (about the width of an adult finger) from each other; this helps to avoid repeat tissue trauma. One approach involves dividing sites into quadrants (or halves when using the buttocks or thighs), using one quadrant per week and moving from quadrant to quadrant in a consistent direction (e.g., clockwise). Encourage people to rotate injections between sites, as well as within a site. Use needles once and toss, since excessive reuse of needles can traumatize the skin and underlying structures. (See photo of lipohypertrophy below)
Finally, Answer 4 is incorrect. 27.67% chose this answer, “Use a higher gauge needles to enhance absorption.” This is not the best answer since it doesn’t address the core issue of injection site overuse and fat accumulation. Switching to a higher gauge needle just means the barrel of the needle is thinner and hurts less when passing through the skin. Improper injection site rotation and needle reuse are the most common factors associated with lipohypertrophy. (See photo of lipohypertrophy below)
Read more great info here, The Injection Technique Factor: What You Don’t Know or Teach Can Make a Difference – Article from Clinical Diabetes, 2019. You are also invited to join our Virtual Conference where we tackle this topic and many more factors that affect diabetes self-care.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
LS is 72 years old with type 2 diabetes and injects insulin 4 times a day. They were started on a CGM device last month and you are looking at the Ambulatory Glucose Profile (AGP) together. You notice their time in range is 60%, their time above range is 38%, in low range is 2% and their coefficient of variation is less than 36%.
What is the best response?
Click Here to Test your Knowledge
Join our Virtual Conference to gain valuable insights from
Technology Expert, Dr. Diana Isaacs
and/or

Topics covered include:
Intended Audience: A great course for healthcare professionals who want to learn the steps involved in providing a thorough lower extremity assessment.
Instructor: Beverly Thomassian RN, MPH, CDCES, BC-ADM is a working educator and a nationally recognized diabetes expert.
All hours earned count toward your CDCES Accreditation Information
Don’t worry if you can’t make it live. Your registration guarantees access to the recorded version in the Online University.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
Belly Dance “Fun”damentals – Women of all ages and body shapes invited!
Join us in a safe, body-accepting environment and experience a sense of community while having fun learning the fundamentals of belly dance. Students wear workout clothes that they feel comfortable in and we supply sparkly hip shawls and veils. The movements of belly dance help strengthen core muscles, improve balance, and build self-confidence. This performance art is open to people of all ages and shapes. Join us to celebrate our strength and express joy through community, belly rolls and lots of shimmies!
Location: monca art museum
900 Esplanade, Chico, CA 95926
Time: Saturdays from 10am – 11am
Cost: $10 a class or $60 for 8 classes
All proceeds are donated to monca to support the arts.
You can mail payment to monca or bring payment to first class.
You can also venmo @Beverly-Thomassian
Click on this Link to Sign Up and hold your spot.
Instructor:
Belly Dance Fundamentals with Anushala (Beverly). She started shimmying when she turned 40 and hasn’t stopped since. Dancing lightens her life and brings immense joy. Plus, she loves sharing this art form with others. She believes in the healing powers of dance and community.
Share this flyer and invite your friends! We will have so much FUN!
We hope you can join us. You can email questions to [email protected].
For last week’s practice question, we quizzed test takers on the right amount of insulin for an 83 year old. Only 50% of respondents chose the best answer, which indicates that there was some confusion. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question:
MS is an 83-year-old admitted to the hospital for a broken hip. MS has a BMI of 22.4, A1C of 6.9% on metformin 500mg twice daily. UACR is less than 30 and GFR is 48. The MD writes to stop oral meds in prep for surgery and start on basal-bolus insulin therapy.
Based on MS’s profile, what would be the most accurate formula to calculate their total daily insulin dose?
Answer Choices:
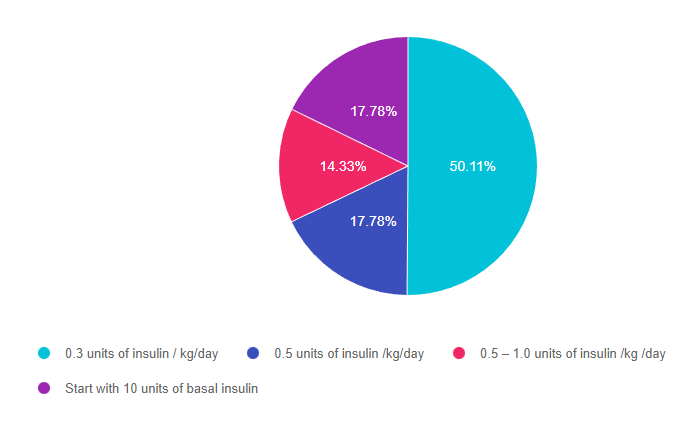
Answer 1 is correct. 50.11% chose this answer, 0.3 units of insulin / kg/day.” YES, GREAT JOB. This is the best answer for several reasons. We can tell from the case study that MS is a frail 83-year-old who is probably very insulin sensitive based on the following details: BMI of 22.4, A1C of 6.9% and GFR is 48. Leaner individuals need less insulin and people with a low GFR have slower renal clearance of insulin putting them at higher risk of hypoglycemia. In addition MS is insulin naïve and their A1C is on target on only 1000mg of Metformin daily. For all these reasons, starting on a VERY conservative total daily insulin dose is the best and safest approach.
Answer 2 is incorrect. 17.78% of you chose this answer, “0.5 units of insulin /kg/day.” This is a juicy answer However MS is a frail 83-year-old who is probably very insulin sensitive based on the following details: BMI of 22.4, A1C of 6.9% and GFR is 48. Leaner individuals need less insulin and people with a low GFR have slower renal clearance of insulin putting them at higher risk of hypoglycemia. In addition MS is insulin naïve and their A1C is on target on only 1000mg of Metformin daily. For all these reasons, starting MS on 0.5 units/kg total daily insulin might be too much and might put MS at risk of hypoglycemia due to over insulinization.
Answer 3 is incorrect. 14.33% of respondents chose this answer, “0.5 – 1.0 units of insulin /kg /day.” This is another juicy answer However MS is a frail 83-year-old who is probably very insulin sensitive based on the following details: BMI of 22.4, A1C of 6.9% and GFR is 48. Leaner individuals need less insulin and people with a low GFR have slower renal clearance of insulin putting them at higher risk of hypoglycemia. In addition MS is insulin naïve and their A1C is on target on only 1000mg of Metformin daily. For all these reasons, starting MS on 0.5 – 1.0 units/kg total daily insulin might be too much and might put MS at risk of hypoglycemia due to over insulinization.
Finally, Answer 4 is incorrect. 17.78 chose this answer, “Start with 10 units of basal insulin.” This answer is appealing, since we often start people on 10 units of basal insulin. However, in this case study, we don’t have MS’s body weight to calculate their total daily insulin needs. Since we don’t have their weight in kgs, we don’t know what the right starting basal dose. For this reason, this is not the best answer.

Glucose control in the hospital matters! This course provides participants with a step-by-step approach to safely and effectively implement Basal Bolus Insulin Therapy in the inpatient setting. We discuss appropriate insulin dosing based on the patient’s clinical presentation and apply dosing strategies to a variety of case studies. Included are hard-to-manage situations that commonly occur in hospital settings and a discussion of solutions that will keep patients safe and get glucose levels to goal. In addition, sample basal/bolus and insulin drip guidelines plus lots of resource articles are included.
Objectives:
Don’t worry if you can’t make it live. Your registration guarantees access to the recorded version in the Online University.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
JL is 67 years old, with a BMI of 23 and A1C of 7.6% and injects insulin 4 times a day to manage their type 1 diabetes. On visual inspection, you notice that there are many areas of lipohypertrophy on JL’s abdominal region.
Which of the following interventions would be the best recommendation?
Click Here to Test your Knowledge
Whether you are new to diabetes or a seasoned expert, you’ll benefit from this virtual conference with the latest research plus critical content that you can immediately apply to your clinical practice.
Download Course Flyer | Download Schedule
If you are seeking a state-of-the-art review of current diabetes care, this course is for you. Our team has been fine-tuning this course for over fifteen years, and we know what you need. This program can also be a great addition to your CDCES or BC-ADM exam study plan.
Team of expert faculty includes:
Don’t worry if you can’t make it live. Your registration guarantees access to the recorded version in the Online University.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
If you are considering taking the CDCES or BC-ADM Exam, we have great news. We are offering 2 different options that will help you get started or propel you across the finish line.
3 Day Intensive: Diabetes Ed Virtual Training Conference streams LIVE in October. Invite your friends to enjoy a group discount. Plus, save on travel costs and enjoy conference interactivity through demonstrations, games and Q&A sessions. Our Deluxe Conference Package includes a 100+ page printed syllabus, Med PocketCards, ADA Standards and swag. This advanced level course features 3 expert speakers who translate the ADA Standards, Meds, Technology, Complications, Nutrition Therapy and more. Join us to get recharged or to prepare for certification.
Self-Study Online Certification Bundles: These courses are designed to walk participants through the knowledge needed to succeed at either the CDCES or BC-ADM certification exams. Viewed at your convenience and pace, each module contains poll questions, case studies and real life situations that prepare participants for clinical situations as well as the exams. Students consistently state that our online courses not only helped them achieve certification, they also provided valuable insights into providing effective diabetes care. See more info below.
As health care professionals, we value your limited study time by offering evidence-based content carefully crafted for exam success with direct application to your clinical practice.
Please let us know if we can be of any help on your journey!
Warmly, Coach Beverly and Bryanna
Whether you are new to diabetes or a seasoned expert, you’ll benefit from this virtual conference with the latest research plus critical content that you can immediately apply to your clinical practice.
Download Course Flyer | Download Schedule
If you are seeking a state-of-the-art review of current diabetes care, this course is for you. Our team has been fine-tuning this course for over fifteen years, and we know what you need. This program can also be a great addition to your CDCES or BC-ADM exam study plan.
Team of expert faculty includes:
Don’t worry if you can’t make it live. Your registration guarantees access to the recorded version in the Online University.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
For last week’s practice question, we quizzed test takers on if you should toss food if it is past the expiration date. Only 35% of respondents chose the best answer, which indicates that there was some confusion. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question:
A person comes into the clinic for a diabetes education appointment. They are on a budget and ask you if they should throw away food if it is older than the date on the package.
What is the most accurate response?
Answer Choices:
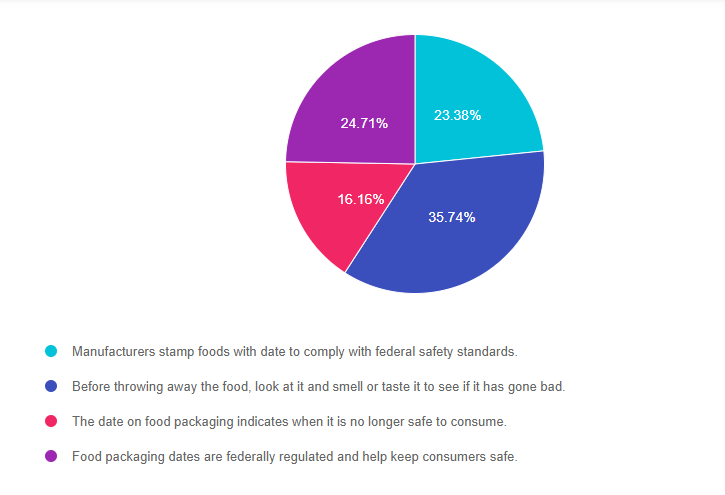
Answer 1 is incorrect. 23.38% chose this answer, “Manufacturer’s stamp foods with a date to comply with federal safety standards.” This is a juicy answer, but it is not the best answer. Except for infant formula, dates are not an indicator of the product’s safety and are not required by Federal law. Since the federal government doesn’t require the dates, the “sell by” or “enjoy by” dates are determined mostly by the manufacturers. Manufacturers put the date on the package to encourage consumers to eat the food product when it tastes best, not when the food will go “bad”. They want to protect their brand and encourage the consumer to purchase their product again.
Answer 2 is correct. 35.74% of you chose this answer, “Before throwing away the food, look at it and smell or taste it to see if it has gone bad.” Research shows that one in three bags of groceries purchased will end up in the trash due to dates stamped on food items. According to the United States Department of Agriculture (USDA), foods are still safe for consumption after these expiration dates pass, but make sure to look out for an off odor, flavor, or texture that mean the food has spoiled and should not be eaten.
The FDA says the dates on food aren’t serving a safety role. A food and law expert, Broad Leib says, “however, you do want to pay attention to dates on food in the prepared food section, including deli meat, raw fish, unpasteurized milk and cheese.” But for most foods, like a box of mushrooms or a bottle of ketchup, Broad Leib suggests we take a pause to look at the food. Smell and taste it to determine if it seems okay to eat. We can tell if something went bad.
Answer 3 is incorrect. 16.16% of respondents chose this answer, “The date on food packaging indicates when it is no longer safe to consume. ” This is a juicy answer, but it is not the best answer. Except for infant formula, dates are not an indicator of the product’s safety and are not required by Federal law. Since the federal government doesn’t require the dates, the “sell by” or “enjoy by” dates are determined mostly by the manufacturers. Manufacturers put the date on the package to encourage consumers to eat the food product when it tastes best, not when the food will go “bad”. They want to protect their brand and encourage the consumer to purchase their product again.
Finally, Answer 4 is incorrect. 24.71% chose this answer, “Food packaging dates are federally regulated and help keep consumers safe.” This is a juicy answer, but it is not the best answer. Except for infant formula, dates are not an indicator of the product’s safety and are not required by Federal law. Since the federal government doesn’t require the dates, the “sell by” or “enjoy by” dates are determined mostly by the manufacturers. Manufacturers put the date on the package to encourage consumers to eat the food product when it tastes best, not when the food will go “bad”. They want to protect their brand and encourage the consumer to purchase their product again.

Have you inspected a food product that you bought last week and wondered if you should toss it because it expired yesterday? If you said yes, you are not alone.
About 40% of food waste happens in the kitchen, when consumers throw away foods that have passed the expiration date.
Are we throwing away perfectly good food based on the date stamped on the package?
Dates are confusing and they are often not associated with safety concerns. Learn why food and legal experts are asking consumers to reconsider their thinking.
Whether you are new to diabetes or a seasoned expert, you’ll benefit from this virtual conference with the latest research plus critical content that you can immediately apply to your clinical practice.
Download Course Flyer | Download Schedule
If you are seeking a state-of-the-art review of current diabetes care, this course is for you. Our team has been fine-tuning this course for over fifteen years, and we know what you need. This program can also be a great addition to your CDCES or BC-ADM exam study plan.
Team of expert faculty includes:
Don’t worry if you can’t make it live. Your registration guarantees access to the recorded version in the Online University.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
If you are considering taking the CDCES or BC-ADM Exam, we have great news. We are offering 2 different options that will help you get started or propel you across the finish line.

3 Day Intensive: Diabetes Ed Virtual Training Conference streams LIVE in October. Invite your friends to enjoy a group discount. Plus, save on travel costs and enjoy conference interactivity through demonstrations, games and Q&A sessions. Our Deluxe Conference Package includes a 100+ page printed syllabus, Med PocketCards, ADA Standards and swag. This advanced level course features 3 expert speakers who translate the ADA Standards, Meds, Technology, Complications, Nutrition Therapy and more. Join us to get recharged or to prepare for certification.
Self-Study Online Certification Bundles: These courses are designed to walk participants through the knowledge needed to succeed at either the CDCES or BC-ADM certification exams. Viewed at your convenience and pace, each module contains poll questions, case studies and real life situations that prepare participants for clinical situations as well as the exams. Students consistently state that our online courses not only helped them achieve certification, they also provided valuable insights into providing effective diabetes care. See more info below.
As health care professionals, we value your limited study time by offering evidence-based content carefully crafted for exam success with direct application to your clinical practice.
Please let us know if we can be of any help on your journey!