
Subscribe
eNewsletter
Ready to get certified?
Free CDCES Coach App
eNewsletter
Free CDCES Coach App
Happy Earth Day Everyone!

In celebration of Earth Day, we are excited to highlight the importance of plants and their role in supporting wildlife. The biggest secret to success is choosing Native Plants for your outdoor pots, balcony, yard or garden this year.
By choosing plants that originated from your geographic area, you help support your regional ecosystem and offer pollinators, birds, butterflies and other healthy critters needed food, pollen and building materials for their survival.
When we first moved into our house 24 years ago, we just planted flowers and grasses that we found visually appealing and could tolerate the heat of our region. Our house and my office are situated on an acre of land, so there was lots of space to plant a wide variety of foliage and trees to provide shade and beauty. But, we weren’t yet tuned-in to the native plant and animal habitats of our new home.
To be honest, 25 years ago, I didn’t give much thought to supporting native plants or animals.
Over time, I started learning about the impact habitat loss for creatures and pollinators. I started exploring plants that support our local area and found a native nursery nearby my home. Now, my husband and I are working hard to make our land a nourishing and welcoming space for pollinators, birds, amphibians, lizards and more. With the help of a few great websites and a visit to our local native nursery, we now bring home plants that support our community of animals and are drought tolerant at the same time.
In addition to plants, providing a water source can be a game changer for thirsty pollinators, birds and others animals too. Simply placing a bowl of water, bird bath or even creating a small pond can make a big difference in supporting a variety of wild life. Last year, we dug a frog pond and within a few short weeks, frogs, toads and birds arrived to enjoy a drink, take a swim or a bath. A year later, our pond is teaming with tadpoles, mosquito fish, water beetles, dragonflies and lots of microscopic creatures. This lively pond brings me, my family and our visitors an abundance of joy and wonderment. Plus, we appreciate how connecting with nature improves our mental health and helps with stress management and well being.
For people with diabetes or other chronic health issues, caring for plants and living beings can be very therapeutic and gratifying, and it doesn’t have to be complicated. Just take one step at a time.
I encourage you to check out the article, Audubon – 20 Common Types of Native Plants, which includes a helpful list of 20 different native plants that support wildlife in the United States. You can cross-reference plants with your zip code finder above to see if these would be a good addition to your neighborhood. For example, in Chico, California, the California Christmas-Berry is a great food source for local birds and is drought tolerant.
In general, consider adding these native plants to your wish list:
Trees: Oaks, Pines, Dogwoods and Willows.
To bring color to your yard, porch or planters try planting Sunflowers or Coneflowers.
Treats for you and our bird friends include Blueberries, Elderberries, or Service berries.
Audubon has a great tool, Audubon – 20 Common Types of Native Plants, in which you can enter your zip code to see which plants are native to your locality.
The National Wildlife Federation (NWF) also provides a wonderful website, Native Plant Finder – NWF, to determine by zip code, native plants for your area. You can create and save your own personalized plant list too.
The Plant Native website, provides a listing of native nurseries throughout the U.S.
I also encourage you to visit www.Earthday.org and Project Regeneration for other great ideas to improve the health of our planet.

Many of us feel discouraged about what is happening to our planet, but there is a rising awareness of our impact and also a rising belief in our ability to protect this beautiful earth. Each action matters. Your action matters. And you can just start by planting one bush, flower, tree, plant or another acting on another idea that is meaningful to you. Thank you in advance for your action.
MJ is on an insulin pump and takes 1 unit of insulin for every 15 gms of carb. For a meal with 5 ounces of steak, medium baked potato with sour cream, asparagus, and salad, MJ bolused 3 units of insulin to cover carbs. What might MJ expect to happen 3 hours later?
Click Here to Test your Knowledge

Whether you are new to diabetes or a seasoned expert, you’ll benefit from this virtual conference with the latest research plus critical content that you can immediately apply to your clinical practice.
Download Course Schedule | Download Course Flyer
If you are seeking a state-of-the-art review of current diabetes care, this course is for you. Our team has been fine-tuning this course for over fifteen years, and we know what you need. This program can also be a great addition to your CDCES or BC-ADM exam study plan.
Join us LIVE for this Virtual Course and enjoy a sense of community!
Team of expert faculty includes:
Deluxe Option for $499: Virtual Program includes:
Deluxe Version includes Syllabus, Standards and Swag*:
Deluxe Option for $499: Virtual Program includes:
Don’t worry if you can’t make it live. Your registration guarantees access to the recorded version in the Online University.
All hours earned count toward your CDCES Accreditation Information
Are you preparing for the CDCES Exam?
Starting your journey to becoming a CDCES? We recommend watching our FREE Preparing for CDCES Exam Webinar!
This course will transform your test anxiety into calm self-confidence and test taking readiness.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.

This year, the ADA Standards focused on the importance of fiber. Since fiber intake is so important to our health, we decided to deem it the new “F” word for 2022. To highlight this under-consumed nutrient, we quizzed test takers on the goal of fiber intake. 70% of respondents chose the best answer. We want to share this important updated information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer below: Answer Question
Question: AR has type 2 diabetes, is on metformin 1000mg BID, has a UACR of 28 mg/g and a GFR of 62. AR is struggling with constipation. What are the ADA Fiber Intake Recommendations?
Answer Choices:
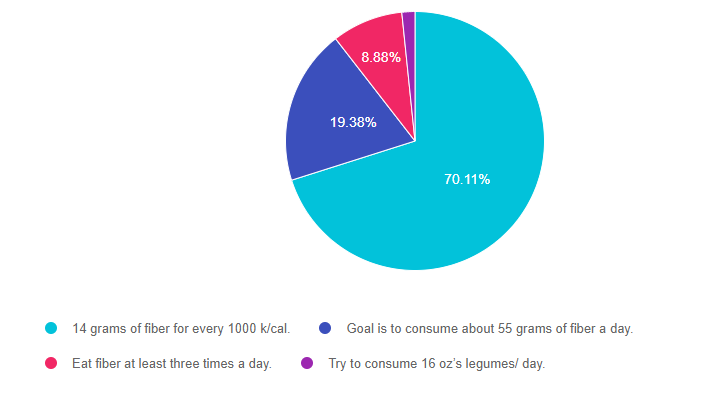
As shown above, the most common choice was option 1, the second most common answer was option 2, then option 3, and then finally option 4.
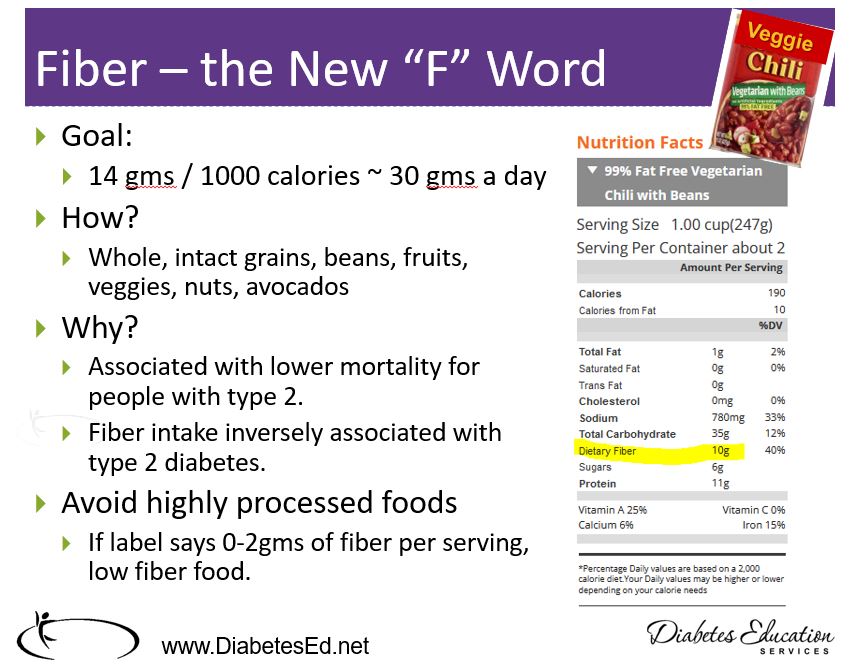
Answer 1 is correct. 70.11% chose this answer, “14 grams of fiber for every 1000 k/cal.” YES, GREAT JOB. This is the best answer based on the ADA Standards of Care and national nutrition guidelines. The daily goal is to consume about 30gms of fiber a day. Yet, most Americans only eat about half that amount. Approximately 70% of the food consumed in the U.S. is processed. Processed and fast foods are notorious for low fiber content. Fiber intake is associated with better overall health, improved longevity, and happier gut bacteria. By increasing intake of fresh fruit, legumes, vegetables, popcorn, avocados, whole grains, and nuts, we would all feel a little bit better.
Answer 2 is incorrect. 19.38% of you chose this answer, “Goal is to consume about 55 grams of fiber a day.” This is a juicy answer, but a little ambitious. The daily goal is to consume about 30gms of fiber a day. Yet, most Americans only eat about half that amount.
Answer 3 is incorrect. 8.88% of respondents chose this answer, “Eat fiber at least three times a day.” Eating fiber at each meal is a great idea, but the goal is to consume at least 30gms a day.
Finally, Answer 4 is incorrect. 1.63% chose this answer, “Try to consume 16 oz’s legumes/ day.” While legumes are very high in fiber (16 ounces of beans, packs 70gms of fiber), the goal is to consume 30gms from whatever sources of fiber the individual enjoys most.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this important learning activity!
Whether you are new to diabetes or a seasoned expert, you’ll benefit from this virtual conference with the latest research plus critical content that you can immediately apply to your clinical practice.
If you are seeking a state-of-the-art review of current diabetes care, this course is for you. Our team has been fine-tuning this course for over fifteen years, and we know what you need. This program can also be a great addition to your CDCES or BC-ADM exam study plan.
Download Course Schedule | Download Course Flyer
Join us LIVE for this Virtual Course and enjoy a sense of community!
Team of expert faculty includes:
Download Course Schedule | Download Course Flyer
Deluxe Option for $499: Virtual Program includes:
Deluxe Version includes Syllabus, Standards and Swag*:
Deluxe Option for $499: Virtual Program includes:
Don’t worry if you can’t make it live. Your registration guarantees access to the recorded version in the Online University.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
The new ADA Standard on Chronic Kidney Disease and Risk Management outlines importance of measuring kidney function and the impact on our practice and quality of life for people living with diabetes.
Based on my review, we share four findings and take a closer look at renal function tests and their significance.
4 Kidney function findings that impact our practice:
What is albuminuria?
Albuminuria is a general term that means there is significant protein in the urine. In the old days, we would order a 24 hour urine collection to determine the degree of albumin in the urine. We used the terms microalbuminuria to describe slightly elevated protein levels and macroalbuminuria to describe significant urine albumin. Since those terms are no longer used, how do we describe how much protein is in the urine? Now, we use Urinary Albumin Creatinine Ratio (UACR) to determine levels of urine protein and their significance.
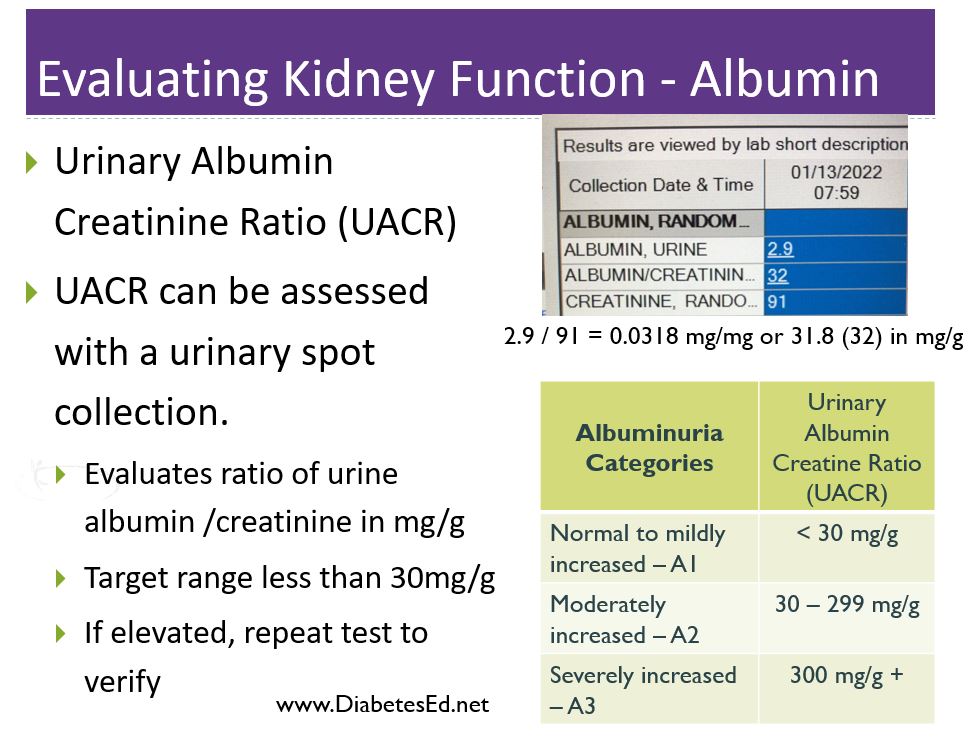
What Exactly is Urinary Albumin Creatinine Ratio (UACR)?
Simply put, UACR is ratio of urine albumin to urine creatinine. The UACR is usually already calculated on the lab report, but using this lab example to the right, the albumin is 2.9 and the urine creatinine is 91. To determine the UACR, you would divide albumin by creatinine, 2.9 / 91 = 0.0318 in mg/mg. Then convert it to mg/g by moving the decimal point over three places, or 31.8 (32) in mg/g.
The reason this value is reported as a ratio as opposed to just urine albumin, is to account for the concentration and hydration status of the individual which improves accuracy.
UACR is an important measure of kidney health and the goal is to measure it yearly and if elevated, more frequently.
Any level of UACR 30mg/g or greater indicates kidney damage and requires prompt protective action by the health care team.
Action to protect the kidney include lifestyle interventions, blood pressure (ACE or ARB) and blood glucose management, along with use of SGLT-2 Inhibitors, GLP-1 RA’s and possibly finerenone.
Testing for UACR and Confirming Results
Testing for UACR is fairly easy. The ADA has approved using urine dipstick or a urine sample to calculate the UACR, However, according to the standards, two of three tests need to be positive to confirm diagnosis within a 3 to 6 month period before confirming diagnosis of moderate or severe albuminuria. Exercise within 24 h, infection, fever, congestive heart failure, marked hyperglycemia, menstruation, and marked hypertension may elevate UACR independently of kidney damage.
How to test for GFR
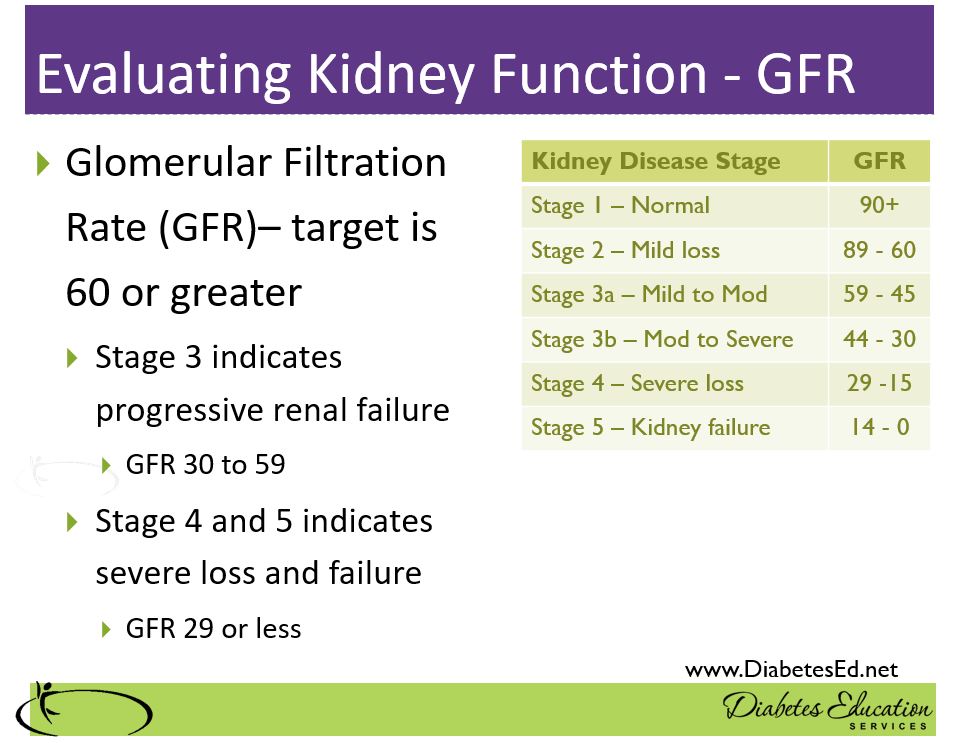
Another measure of kidney function is the Glomerular Filtration Rate. The result is derived from a complicated mathematical calculation, using the person’s creatinine and other data. For this reason, it’s often called an estimated GFR or eGFR. People with diabetes need their creatinine evaluated yearly to determine their GFR. Here is a link to an eGFR Calculator.
For people with diabetes, we start keeping a close eye on the GFR when levels start dropping below 60. As with UACR, heath care providers need to take preventive action to maintain kidney function and protect GFR through lifestyle and medications.
In conclusion, as diabetes specialists, being familiar with the results of these kidney health measures help us advocate on behalf of people with diabetes. Making sure our health care organizations are regularly measuring kidney function and taking action to protect these amazing filtering units can save lives and improve quality of life.
You are reviewing an ambulatory glucose profile with JR, a 27-year-old on an insulin pump. Time in range is 59% and the coefficient of variation is 46%. JR asks you to explain the coefficient of variation. What is the most helpful response?
Click Here to Test your Knowledge
Whether you are new to diabetes or a seasoned expert, you’ll benefit from this virtual conference with the latest research plus critical content that you can immediately apply to your clinical practice.
Download Course Schedule | Download Course Flyer
If you are seeking a state-of-the-art review of current diabetes care, this course is for you. Our team has been fine-tuning this course for over fifteen years, and we know what you need. This program can also be a great addition to your CDCES or BC-ADM exam study plan.
Join us LIVE for this Virtual Course and enjoy a sense of community!
Team of expert faculty includes:
Deluxe Option for $499: Virtual Program includes:
Deluxe Version includes Syllabus, Standards and Swag*:
Basic Option for $399: Virtual Program includes:
Don’t worry if you can’t make it live. Your registration guarantees access to the recorded version in the Online University.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
We will be awarding 2 Scholarships for our DiabetesEd Specialist Virtual Conference! Due March 2nd!
If you are passionate about diabetes education, actively involved in providing the best diabetes care, preparing for certification and seeking financial assistance to attend our DiabetesEd Specialist Course, you are invited to apply for one of these scholarships.
We are awarding 2 Scholarships for our DiabetesEd Specialist Virtual Conference, April 13-15, 2022.
We don’t want financial barriers to stop anyone from attending this conference. In appreciation of those who are role models and advocates for practicing the best diabetes care in their communities, we are offering one $499 Scholarships and one $399 dollar scholarship. Scholarships are due by March 2nd, so apply today!
Download Course Schedule | Download Course Flyer
“Not just a course – it’s an experience”
An opportunity to earn 30+ CEs and learn in an interactive, fun-spirited environment with our team of experts.
Regular price: $499 or $399
The goal of these scholarships are three-fold:

Whether you are new to diabetes or a seasoned expert, you’ll benefit from this virtual conference with the latest research plus critical content that you can immediately apply to your clinical practice.
If you are seeking a state-of-the-art review of current diabetes care, this course is for you. Our team has been fine-tuning this course for over fifteen years, and we know what you need. This program can also be a great addition to your CDCES or BC-ADM exam study plan.
Download Course Schedule | Download Course Flyer
Join us LIVE for this Virtual Course and enjoy a sense of community!
Team of expert faculty includes:
Deluxe Option for $499: Virtual Program includes:
Deluxe Version includes Syllabus, Standards and Swag*:
Basic Option for $399: Virtual Program includes:
Don’t worry if you can’t make it live. Your registration guarantees access to the recorded version in the Online University.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
The first tubeless Automated Insulin Delivery (AID) System, was just approved by the Food and Drug Administration (FDA).
The Omnipod 5 hybrid closed-loop system (Insulet Corporation) links with Dexcom’s G6 Continuous Glucose Monitor and is now FDA approved for people with type 1 diabetes age six and older.
This anxiously awaited approval now means that there are 3 semi-automated closed-loop insulin delivery systems in the United States.
A unique feature of the Omnipod 5 system, is that it includes the first approved tubing free insulin delivery device that is paired with the Dexcom G6 continuous glucose monitor (CGM). The Omnipod holds up to 3 days of insulin and is worn directly on the body.
Omnipod 5 Users can monitor glucose trends and deliver insulin using a smartphone app or a separate controller device. Plus, this SmartAdjust technology automatically adjusts insulin to keep glucose on target and minimize hypo and hyperglycemic events.
Included in the app is a SmartBolus calculator that receives Dexcom CGM values every 5 minutes and automatically adjusts insulin based on predicted values for 60 minutes into the future and the individual’s customized glucose targets.
Insulet said it will begin selling the prescription Omnipod 5 device through U.S. pharmacies, starting with an initially limited release before expanding its commercial reach. The company is also offering users of its current Omnipod DASH system—a more manual tubeless pump—an upgrade to the Omnipod 5 at no additional cost once insurance coverage becomes available.
Read more here Omniopod approved by FDA.
Whether you are new to diabetes or a seasoned expert, you’ll benefit from this virtual conference with the latest research plus critical content that you can immediately apply to your clinical practice.
If you are seeking a state-of-the-art review of current diabetes care, this course is for you. Our team has been fine-tuning this course for over fifteen years, and we know what you need. This program can also be a great addition to your CDCES or BC-ADM exam study plan.
Download Course Schedule | Download Course Flyer
Join us LIVE for this Virtual Course and enjoy a sense of community!
Team of expert faculty includes:
Deluxe Option for $499: Virtual Program includes:
Deluxe Version includes Syllabus, Standards and Swag*:
Deluxe Option for $499: Virtual Program includes:
Don’t worry if you can’t make it live. Your registration guarantees access to the recorded version in the Online University.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
AR has type 2 diabetes, is on metformin 1000mg BID, has a UACR of 28 mg/g and a GFR of 62. AR is struggling with constipation. What are the ADA Fiber Intake Recommendations?
Click Here to Test your Knowledge
Whether you are new to diabetes or a seasoned expert, you’ll benefit from this virtual conference with the latest research plus critical content that you can immediately apply to your clinical practice.
If you are seeking a state-of-the-art review of current diabetes care, this course is for you. Our team has been fine-tuning this course for over fifteen years, and we know what you need. This program can also be a great addition to your CDCES or BC-ADM exam study plan.
Download Course Schedule | Download Course Flyer
Join us LIVE for this Virtual Course and enjoy a sense of community!
Team of expert faculty includes:
Deluxe Option for $499: Virtual Program includes:
Deluxe Version includes Syllabus, Standards and Swag*:
Deluxe Option for $499: Virtual Program includes:
Don’t worry if you can’t make it live. Your registration guarantees access to the recorded version in the Online University.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.