
Subscribe
eNewsletter
Ready to get certified?
Free CDCES Coach App
eNewsletter
Free CDCES Coach App
Are you considering pursuing certification in diabetes care, but are not sure which certification is right for you and how to get started?

Coach Beverly is excited to share her insights on determining the best certification choice and the pathway to success. She will share her personal journey on achieving both her CDCES and BC-ADM over 20 years ago and how these credentials have impacted her opportunities as a diabetes specialist and president of her own company. We hope you can join us!
Webinar Topics
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.

Our November 23rd Question of the week quizzed test takers on the Nobel Prize insulin. 34% of respondents, chose the best answer. We are excited to share this info about the discovery of insulin with you.
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer below: Answer Question
Question:
In 1923, the Nobel Prize in Physiology or Medicine was awarded for the discovery of insulin.
Which group of scientists were the recipients of the award?
Answer Choices:
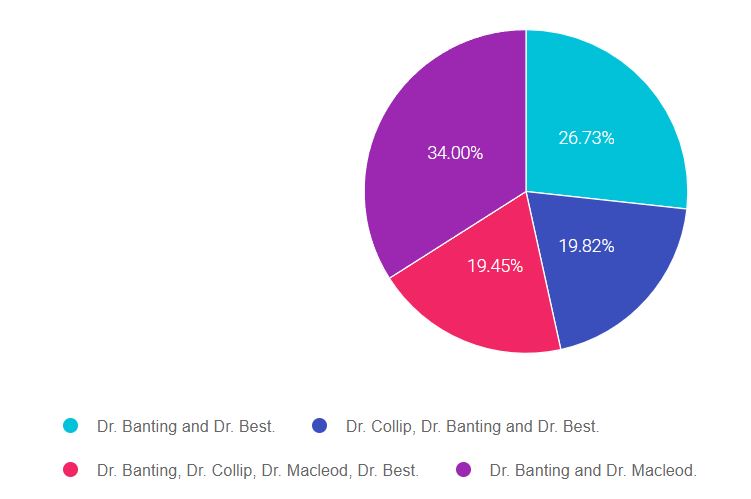
As shown above, the most common choice was option 3, the second most common answer was option 2, then option 4, and finally option 1.

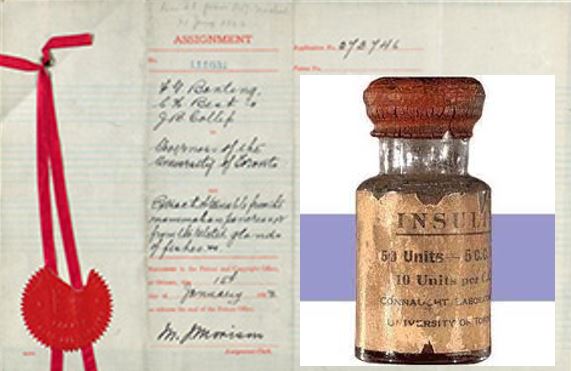
The Nobel Prize in Physiology or Medicine 1923 was awarded jointly to Frederick Grant Banting and John James Rickard Macleod “for the discovery of insulin.”
According to the summary at the Nobel Prize Website – Previous doctors realized that diabetes is caused by a lack of insulin, which is formed in parts of the pancreas but could not prove it. Frederick Banting suspected that another substance formed in the pancreas, trypsin, broke down the insulin.
In John MacLeod’s laboratory in 1921, Frederick Banting and Charles Best treated dogs so that they no longer produced trypsin. Insulin could then be extracted and used to treat diabetes. A short while later, Dr. Collip made a breakthrough in purifying the extract, using alcohol in slightly over 90 percent concentration to precipitate out the active ingredient (insulin).
Although Dr. Banting, Dr. Collip, Dr. Macleod, and Dr. Best were all involved in the discovery of insulin, only Dr. Banting and the lab director, Dr. Macleod received the official Nobel prize for Medicine.
Answer 1 is incorrect. 26.73% chose this answer, “Dr. Banting and Dr. Best.” Credited for their experiments on dogs at the University of Toronto in 1921 that eventually led to the discovery of insulin.
Answer 2 is incorrect. 19.82% of you chose this answer, “Dr. Collip, Dr. Banting, and Dr. Best”. Although Dr. Collip made a breakthrough in purifying the extract, using alcohol in slightly over 90 percent concentration to precipitate out the active ingredient (insulin), he, along with Best, was not recognized with a Nobel Prize.
Answer 3 is incorrect. 19.45% of respondents chose this answer, “Dr. Banting, Dr. Collip, Dr. Macleod, Dr. Best” All four of these physicians played a major part in the discovery and availability of insulin, but only Dr. Banting and Dr. Maccleod were awarded the Nobel prize.
Finally, Answer 4 is correct. 34% chose this answer, “Dr. Banting and Dr. Macleod” YES, GREAT JOB.
The Nobel Prize in Physiology or Medicine 1923 was awarded jointly to Frederick Grant Banting and John James Rickard Macleod “for the discovery of insulin.” According to the summary at the Nobel Prize Website – In John MacLeod’s laboratory in 1921, Frederick Banting and Charles Best treated dogs so that they no longer produced trypsin. Insulin could then be extracted and used to treat diabetes.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
You are invited to join Coach Beverly for this FREE Webinar. And, if you want to have access to an additional 220+ sample practice online questions, you can purchase the complete Test Taking Toolkit.
During this webinar, Coach Beverly will help you transform your nervousness into focused energy that will help you succeed. She will provide test-taking tips based on her experience taking the certification exam six times.
This includes a review of 20 sample test questions with test-taking strategies. This does not include access to the recorded webinar or the practice questions.
This includes access to the recorded version of this webinar on your Online University Student Portal.
Plus, the Test Taking Toolkit provides you with over 220 sample online practice questions, simulating the exam experience. A perfect way to assess your knowledge and create a focused study plan, while increasing your test-taking confidence.
Don’t worry if you can’t make it live.
Your registration guarantees access to the recorded version.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
About 30% of people living with type 1 diabetes experience diabetes distress.
Which of the following statements reflects someone struggling with diabetes distress?
Click Here to Test your Knowledge
This presentation will include the latest information on Social Determinants of health, assessment strategies, and approaches. We will explore the psychosocial issues that can discourage individuals from adopting healthier behaviors and provides strategies to identify and overcome these barriers. Life studies are used to apply theory to real-life situations. A great course for anyone in the field of diabetes education or for those looking for a new perspective on assessment and coping strategies.
Objectives:
Intended Audience: A great course for healthcare professionals in the field of diabetes education looking for a straightforward explanation of identification and treatment of hyperglycemic crises.
Instructor: Beverly Thomassian RN, MPH, CDCES, BC-ADM is a working educator and a nationally recognized diabetes expert.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
To celebrate National Diabetes Month, our Questions of the Week will challenge test takers on their historical knowledge of the discovery of insulin. Thanks for joining us on this fun adventure.
In 1923, the Nobel Prize for in Medicine was awarded for the discovery of insulin.
Which group of scientists were the recipients for the award?
Click Here to Test your Knowledge
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
This month, we are quizzing test takers on the history of diabetes. Our November 16th Question of the week quizzed test takers on the cost of the insulin patent. 74% of respondents, chose the best answer. We are excited to share this info with you in celebration of National Diabetes Month.
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer below: Answer Question
Question:
On January 23rd, 1923, Dr.’s Banting, Best, and Collip were awarded the patent for insulin.
How much did Banting, Best, and Collip each charge the University of Toronto for their share of the insulin patent?
Answer Choices:
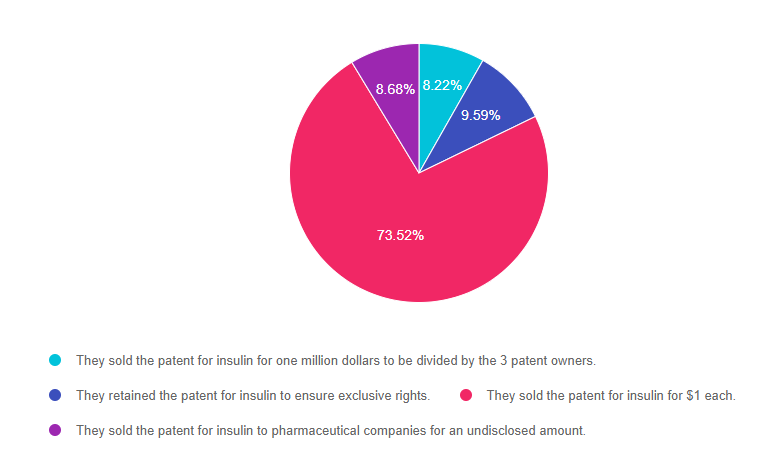
As shown above, the most common choice was option 3, the second most common answer was option 2, then option 4, and finally option 1.
On January 23rd, 1923 Banting, Best, and Collip were awarded the American patents for insulin. They sold the patent to the University of Toronto for $1 each. Banting notably said: “Insulin does not belong to me, it belongs to the world.” His desire was for everyone who needed access to it to have it.
In order for the insulin to be mass-produced and widely available, the pharmaceutical company Eli Lilly and Co. were given the right to do so. Currently, Eli Lilly, Sanofi, and Novo Nordisk are the major insulin producers. Insulin is no longer extracted from beef and pork pancreases. Now companies use E. coli and yeast to produce insulin through recombinant DNA therapy.
With insulin patents expiring, we are now seeing the approval of biosimilar insulins that come with lower price tags. This lower-cost insulin keeps Dr. Banting’s dream alive, which is to make insulin a gift that belongs to the world.
Answer 1 is incorrect. 8.22% chose this answer, “They sold the patent for insulin for one million dollars to be divided by the 3 patent owners.”
Answer 2 is incorrect. 9.59% of you chose this answer, “They retained the patent for insulin to ensure exclusive rights.”
Answer 3 is correct. 73.52% of respondents chose this answer, “They sold the patent for insulin for $1 each.” YES, GREAT JOB. This is the BEST ANSWER!
Finally, Answer 4 is incorrect. 8.68% chose this answer, “They sold the patent for insulin to pharmaceutical companies for an undisclosed amount.”
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
You are invited to join Coach Beverly for this FREE Webinar. And, if you want to have access to an additional 220+ sample practice online questions, you can purchase the complete Test Taking Toolkit.
During this webinar, Coach Beverly will help you transform your nervousness into focused energy that will help you succeed. She will provide test-taking tips based on her experience taking the certification exam six times.
This includes a review of 20 sample test questions with test-taking strategies. This does not include access to the recorded webinar or the practice questions.
This includes access to the recorded version of this webinar on your Online University Student Portal.
Plus, the Test Taking Toolkit provides you with over 220 sample online practice questions, simulating the exam experience. A perfect way to assess your knowledge and create a focused study plan, while increasing your test-taking confidence.
Don’t worry if you can’t make it live.
Your registration guarantees access to the recorded version.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
This month, we are quizzing test takers on the history of diabetes. Our November 9th Question of the week quizzed test takers on Diabetes Mellitus. 49% of respondents, chose the best answer. We are excited to share this info with you in celebration of National Diabetes Month.
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer below: Answer Question
Question:
The term diabetes mellitus is derived from Greek and Latin languages, with roots dating back to the Greek physician Demetrius of Apamea in 129-199 AD.
Which is the most accurate translation of the term diabetes mellitus in English?
Answer Choices:
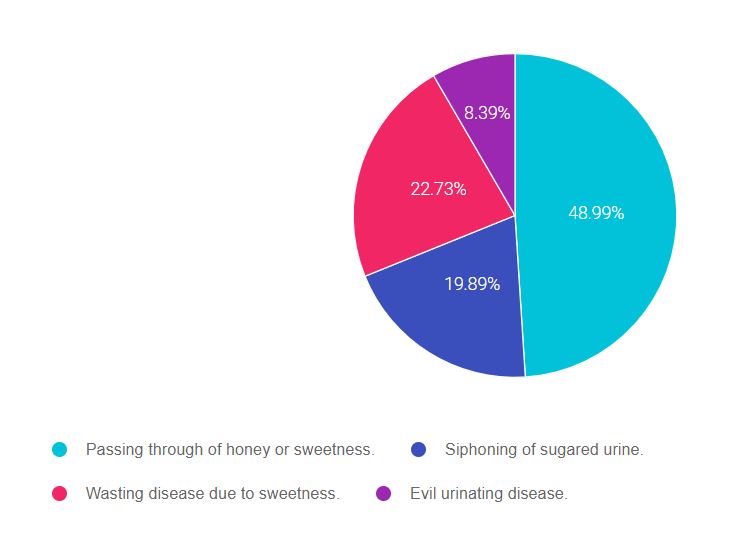
As shown above, the most common choice was option 1, the second most common answer was option 3, then option 2, and finally option 4.
If you are thinking about taking the certification exam, this practice test question will set you up for success. Test writers anticipate possible answers based on the details in the question. They will wave those “juicy answers” that seem so familiar to you, right under your nose. Your job is to weed through, eliminate FALSE answers and then choose the BEST answer.
A short history of the evolution of the term “Diabetes mellitus“
The ancient Egyptians described clinical features of diabetes over 3000 years ago. Indian physicians called it madhumeha (‘honey urine’) because it attracted ants.
However, the term “diabetes” (Greek for ‘siphon’) was first used by Greek physician Demetrius of Apamea in 129-199 AD. The findings of sweet urine and blood was first noticed by ancient Indians. A few thousand years later, the Latin word “mellitus” (‘sweet like honey’) was coined by the British Surgeon-General, John Rollo in 1798.
History of the Islets and Insulin:
Paul Langerhans, 22 and working on his medical doctorate in 1869, identified the beta cells that came to be known as the ‘islets of Langerhans’. The name insulin was based on the secretions of the islets (Latin, insula = island). The term insulin was coined in 1909 and 1910, individually by de Mayer and Schaefer, respectively. Read more in this article, The History of Diabetes Mellitus, 2013 by Ritu Lakhtakia.
Answer 1 is correct. 48.99% chose this answer, “Passing through of honey or sweetness.” YES, GREAT JOB! The term “diabetes” is Greek for ‘siphon or passing through and the “mellitus” is Latin for “sweet like honey”.
Answer 2 is incorrect. 19.89% of you chose this answer, “Siphoning of sugared urine.” This is a juicy answer, but there is no Latin or Greek word for “urine” in the term “diabetes mellitus”.
Answer 3 is incorrect. 22.73% of respondents chose this answer, “Wasting disease due to sweetness.” Another juicy answer, but there is no Latin or Greek word for “wasting disease” in the term diabetes mellitus.
Finally, Answer 4 is incorrect. 8.39% chose this answer, “Evil urinating disease.” Some people might favor this term, but the term “diabetes mellitus” only describes the passing through of honey as a medical observation. There is no judgment associated with it.
Want to learn more about this fascinating topic? Read more in this article, The History of Diabetes Mellitus, 2013 by Ritu Lakhtakia.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!

You are invited to join Coach Beverly for this FREE Webinar. And, if you want to have access to an additional 220+ sample practice online questions, you can purchase the complete Test Taking Toolkit.
During this webinar, Coach Beverly will help you transform your nervousness into focused energy that will help you succeed. She will provide test-taking tips based on her experience taking the certification exam six times.
This includes a review of 20 sample test questions with test-taking strategies. This does not include access to the recorded webinar or the practice questions.
This includes access to the recorded version of this webinar on your Online University Student Portal.
Plus, the Test Taking Toolkit provides you with over 220 sample online practice questions, simulating the exam experience. A perfect way to assess your knowledge and create a focused study plan, while increasing your test-taking confidence.
Don’t worry if you can’t make it live.
Your registration guarantees access to the recorded version.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
Vertex Pharmaceuticals just announced preliminary results from a trial that explores a new intervention to treat type 1 diabetes. The early results are very promising.
The first person with type 1 diabetes to receive this new stem-cell derived experimental therapy, had an 91% drop in their insulin needs. The person has lived with type 1 for over 40 years. After the intervention, they not only experienced a reduction in their insulin needs, their fasting C-peptide levels went from undetectable to 280. This dramatic C-peptide increase is a clinical indicator of stem-cell therapy success and endogenous insulin secretion.
These results are exciting and offer hope for a potential new treatment approach for type 1 diabetes.
VX-880 is a stem cell derived therapy that replaces damaged beta cells with healthy transplanted insulin producing cells in clinical trials. However, these new cells are at risk for attack by the body’s immune system, so immunosuppression therapy is currently required for stem-cell transplant success.
The future goal is to create a version of this treatment that doesn’t require immunosuppressive therapy. And Vertex, the makers of VX-880 are working on creating an encapsulated islet cell program that doesn’t initiate an autoimmune attack.
For more information and clinical trials, click this link.

Below is a list of helpful online resources for Type 1 Diabetes. They include sites for national organizations like the American Diabetes Association (ADA), sites for diabetes interest groups, and other participant organizations that provide helpful diabetes tips and opportunities to join online groups. Click here for a Type 1 Resource Handout to share with colleagues and people living with type 1 diabetes.
Click the links below to visit the website:
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]To celebrate National Diabetes Month, our Questions of the Week will challenge test takers on their historical knowledge of the discovery of insulin. Thanks for joining us on this fun adventure.
On January 23rd, 1923, Dr.’s Banting, Best, and Collip were awarded the patent for insulin.
How much did Banting, Best, and Collip each charge the University of Toronto for their share of the insulin patent?
Click Here to Test your Knowledge
This bundle is specifically designed for healthcare professionals who want to learn more about diabetes fundamentals for their clinical practice or for those who are studying for the Certified Diabetes Care and Education Specialist (CDCES) exam.
2022 Live Webinar Updates
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.