Subscribe
eNewsletter
Ready to get certified?
Free CDCES Coach App
eNewsletter
Free CDCES Coach App
To celebrate National Diabetes Month, our Questions of the Week will challenge test takers on their historical knowledge of the discovery of insulin. Thanks for joining us on this fun adventure.
Which of the following statements is true regarding the first experiments using insulin in humans?
Click Here to Test your Knowledge
Did you miss the live conference? No worries!
You can register now to watch on-demand
Click here to learn more and get started!
Whether you are new to diabetes or a seasoned expert, you’ll benefit from this virtual conference with the latest research plus critical content that you can immediately apply to your clinical practice.
If you are seeking a state-of-the-art review of current diabetes care, this course is for you. Our team has been fine-tuning this course for over fifteen years, and we know what you need. This program can also be a great addition to your CDCES or BC-ADM exam study plan.
Team of expert faculty includes:
In addition to informative lectures, we also use group activities and case studies to highlight the essential knowledge, skills, and strategies needed to succeed in diabetes education today!
CEs: Includes over 30 CEs
Program Info: 2021 Diabetes Educator Course Flyer & Schedule (subject to change)
Speakers: View Conference Faculty.
Dates: Your registration fee includes access to FREE podcast and all recorded webinars for one year.
Virtual DiabetesEd Specialist Conference Deluxe | Recorded & Ready for Viewing! | 30+ CEs
Deluxe Virtual Program for $459 includes:
+Plus Syllabus, Standards and Swag:
2021 Diabetes Educator Course Flyer & Schedule (subject to change)
Team of Experts: Our team of expert faculty has been fine-tuning this course for over fifteen years and we know what you need to succeed! In addition to informative lectures, we also use group activities and case studies to highlight the essential knowledge, skills, and strategies needed to succeed in diabetes education today!
When you register for our Virtual Course, you have immediate access to these Bonus DiabetesEd University Online Courses – for FREE!
2021 Diabetes Educator Course Flyer & Schedule (subject to change)
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
Are you preparing for the CDCES Exam?
Starting your journey to becoming a CDCES? We recommend watching our FREE Preparing for CDCES Exam Webinar!
This course will transform your test anxiety into calm self-confidence and test-taking readiness.
Read More: What is a CDCES? First awarded in 1986, as Certified Diabetes Educator (CDE) credential and in 2020 with a new name: Certified Diabetes Care and Education Specialist (CDCES) to more accurately reflect the specialty. CDCES has become a standard of excellence for the delivery of quality diabetes education. Those who hold this certification are known to possess comprehensive knowledge of and experience in diabetes prevention, management, and prediabetes. “Becoming a Certified Diabetes Care and Education Specialist (CDCES) is one of the best professional and personal decisions I have ever made.” – Coach Beverly Thomassian, RN, MPH, CDCES, BC-ADM 
Read More: 3 Reasons to Become a CDCES “The best part of becoming a CDCES is working with my colleagues and people living with diabetes. As diabetes educators, we hear compelling and beautiful life stories. I am astounded by the barriers they face and inspired by their adaptability, problem-solving skills, and resilience.” Reason 1: CDCES is a widely recognized certification by employers and health care professionals throughout the U.S. This credential demonstrates a specialized and in-depth knowledge in the prevention and treatment of individuals living with pre-diabetes and diabetes. Reason 2: Currently, 10% of people in the U.S. have diabetes and another 35% have pre-diabetes which means 45% of Americans are running around with elevated blood glucose levels. Given this epidemic, there will be plenty of future job opportunities. Reason 3: Having my CDCES along with my nursing degree, has opened many doors of opportunity; from working as an inpatient Diabetes Nurse Specialist in a hospital to working as a Manager of Diabetes Education in the outpatient setting to starting my own consulting company.

Join us live on November 11th from 8:00 am to 4:00 pm for our Virtual Conference: Diabetes in the 21st Century | 6.5 CEs
This conference offers comprehensive presentations on care of a person with diabetes examining a variety of evidence-based topics to aid in the care of a person with diabetes.
Click here to download the program flyer.
Location: Virtual
Fees: No charge for Meritus Health Employees. $50.00 for Non-Meritus Health Participants Meritus Health Employees: Please register via Healthstream, using keyword search “21st Century” or by clicking here.
Cancellation Policy: If you must cancel, please notify Ruth Leizear by phone at 301-790-8619 or toll free at 888-803-1518.
Check-in: Check-in starts at 8:00 a.m., please log in 15 minutes prior to the first presentation
Accreditation:
Click here to download the program flyer.
Instructor: Beverly Thomassian RN, MPH, CDCES, BC-ADM is a working educator and a nationally recognized diabetes expert.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.

Our October 19th Question of the week quizzed test takers on a person who is clearly in crisis. 36% of respondents, chose the best answer. We feel it is important to share this rationale of the week, so you can advocate for people struggling with mental health while trying to manage their diabetes.
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer below: Answer Question
Question: JR is 26 years old with newly diagnosed diabetes. JR keeps missing appointments and when you finally get a hold of them on the phone, they start crying and say “my life is a mess”. JR is struggling with addiction, periods of houselessness and extra weight in addition to diabetes.
Based on this information, what is the most likely barrier to JR engaging in self-care?
Answer Choices:
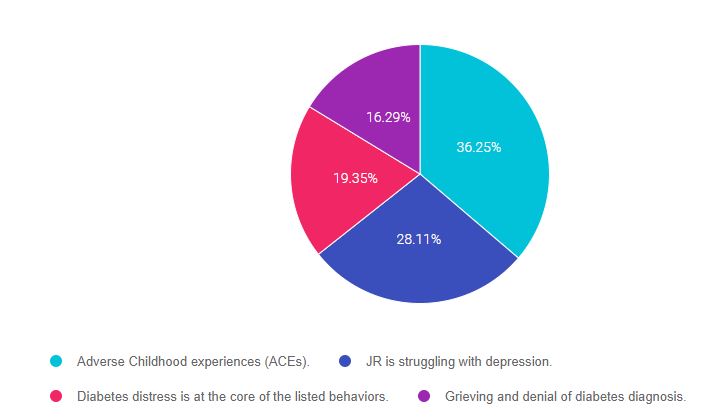
As shown above, the most common choice was option 4, the second most common answer was option 1, then option 2, and finally option 3.
If you are thinking about taking the certification exam, it is helpful to know the goals of care and mental health considerations for people with diabetes . This practice test question will set you up for success. Test writers anticipate possible answers based on the details in the question. They will wave those “juicy answers” that seem so familiar to you, right under your nose. Your job is to weed through the to choose the BEST answer.
Answer 1 is correct. 36.25% chose this answer, “Adverse Childhood Experiences (ACEs).” YES, Good job, this is the BEST Answer. JR is missing appointments and when you finally get a hold of them, they say, “my life is a mess”. In addition, we know that JR is struggling with addiction, periods of houselessness and extra weight in addition to diabetes. These are all signs that JR has lived through adverse childhood experiences and toxic stress. By addressing this and providing resources, we can help JR move toward healing. See our ACE Resource page for more info.
Answer 2 is incorrect. 28.11% of you chose this answer, “JR is struggling with depression.” Is this situation, depression can be considered, but we don’t hear the hallmark statements associated with depression – “Loss of pleasure in things that used to bring them joy or feeling down or hopeless”. ACE’s are a better match for what JR is describing. See our Psychosocial Care Resource Page– for articles and screening tools.
Answer 3 is incorrect. 19.35% of respondents chose this answer, “Diabetes distress is at the core of the listed behaviors.” Is this situation, diabetes distress certainly can be considered, but it doesn’t seem to be the driving force behind JR’s struggle with addiction, periods of houselessness and extra weight. Diabetes distress is more heavily associated with diabetes specific related behaviors (fear of hypo, provider doesn’t understand my diabetes, etc.). See our Psychosocial Care Resource Page– for articles and the diabetes distress screening tool.
Finally, Answer 4 is incorrect. 16.29% chose this answer, “Grieving and denial of diabetes diagnosis.” Is this situation, grieving and denial can certainly can be considered, but it doesn’t seem to be the driving force behind JR’s struggle with addiction, periods of houselessness and extra weight. Diabetes denial is more heavily associated with lack of self-care; not checking blood glucose, avoiding medications, eating “whatever”. We don’t hear any of that from this person. The best explanation is that JR has lived through adverse childhood experiences and toxic stress. By addressing this and providing resources, we can help JR move toward healing. See our ACE Resource page for more info.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Want to learn about this important topic?
Adverse childhood experiences (ACE) are associated with an increased risk of diabetes, heart disease, cancer and a variety of other health consequences for adults. This session reviews how diabetes care and education specialists can provide screening, assessment, and trauma-informed care to individuals who experienced ACEs and are living with toxic stress. We will explore strategies to address ACES and improve outcomes for individuals and communities. Throughout, we will focus on supporting self-care with a focus on recognizing and promoting resilience.
Topics include:
This includes access to the recorded version of this webinar on your Online University Student Portal and 1.0 CE.
Intended Audience: This course is a knowledge-based activity designed for individuals or groups of diabetes educators, including RNs, RDs, Pharmacists, Nurse Practitioners, Clinical Nurse Specialists, Physician Assistants, and other health care providers interested in enhancing their diabetes medication knowledge.
Instructor: Beverly Thomassian RN, MPH, CDCES, BC-ADM is a working educator and a nationally recognized diabetes expert.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
Eli Lilly and Company issues a voluntary nationwide recall of one lot of GLUCAGON® Emergency Kit due to Loss of Potency. Warning – A person with severe hypoglycemia who injects this faulty formulation will experience worsening hypoglycemia.
Eli Lilly and Company is voluntarily recalling lot D239382D, Expiration April 2022, of Glucagon Emergency Kit for Low Blood Sugar (Glucagon for Injection, 1 mg per vial; Diluent for Glucagon, 1 mL syringe).

The Eli Lilly injectable glucagon kit (pictured here), usually contains a syringe with diluent and a vial with powdered glucagon. The user needs to put the diluent into the vial with the powdered glucagon and reconstitute it before injecting it.
However, a product complaint from a user found that the vial of Glucagon was in liquid form instead of powder form. Associated with this useful product complaint, the patient who was given this glucagon vial content, experienced worsening hypoglycemia and also reported subsequent seizures.
The use of the liquid form of this product may fail to treat severe low blood sugar due to loss of potency.
It is well known that severe hypoglycemia in people with diabetes, if not promptly treated and reversed, can potentially cause adverse health consequences ranging from transient, minor complaints to neurological damage, seizures, and even death. Eli Lilly’s investigation indicates that the liquid in this Glucagon vial could be related to a problem with the manufacturing process.
The Eli Lilly Glucagon product is packaged in a kit containing 1mg of freeze-dried (lyophilized) product in a 3 mL vial and a pre-filled diluent syringe. The affected Glucagon Emergency Kit lot is D239382D and the expiration date is April 2022 (label expiry date: 04 2022). The lot number can be found on the label of the kit as well as the vial (refer to the complete FDA warning below). The lot was distributed nationwide to wholesalers and retailers.
Consumers in possession of Glucagon Emergency Kit lot D239382D should contact The Lilly Answers Center at 1-800-LILLYRX (1-800-545-5979) for return and replacement instructions for the product (hours of operation are Monday- Friday, 9AM – 7PM EST) and should contact their health care provider for guidance. Consumers should contact their physician or healthcare provider if they have experienced any problems that may be related to taking or using this product.
Lilly is notifying its distributors and customers by written communication and is arranging for the return and replacement of all recalled products. Wholesalers and Distributors with an existing inventory of Glucagon Emergency Kit lot D239382D should cease distribution and quarantine the product immediately.
Read complete FDA Announcement Here
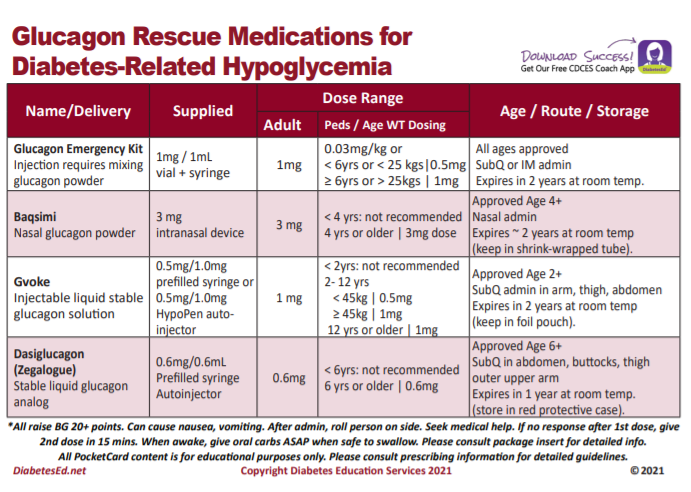
There are now 4 different glucagon formulations to choose from.
This free card details the different formulations available, from the injectables to the nasal powder formulation.
The backside includes teaching and hypoglycemia prevention strategies, along with the different official levels of hypoglycemia (for your certification study preparation).
Join us live on November 11th from 8:00 am to 4:00 pm for our Virtual Conference: Diabetes in the 21st Century | 6.5 CEs
This conference offers comprehensive presentations on care of a person with diabetes examining a variety of evidence-based topics to aid in the care of a person with diabetes.
Click here to download the program flyer.
Location: Virtual
Fees: No charge for Meritus Health Employees. $50.00 for Non-Meritus Health Participants Meritus Health Employees: Please register via Healthstream, using keyword search “21st Century” or by clicking here.
Cancellation Policy: If you must cancel, please notify Ruth Leizear by phone at 301-790-8619 or toll free at 888-803-1518.
Check-in: Check-in starts at 8:00 a.m., please log in 15 minutes prior to the first presentation
Accreditation:
Click here to download the program flyer.
Instructor: Beverly Thomassian RN, MPH, CDCES, BC-ADM is a working educator and a nationally recognized diabetes expert.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.

As Diabetes Specialists, it is helpful and fun to become familiar with the foods of different cultures and regions. For today’s Question of the Week, we are quizzing participants on their recognition of a common dish from a Latin American country. Can you identify where this dish called Bandeja Paisa, shown in this picture, originates from?
Which country does this dish originate from?
Click here to test your knowledge!
This Question of the Week is provided by Lorena Drago, multicultural nutrition expert. Thanks Lorena! You can join Lorena for a culinary trip that highlights the foods and traditions of the six largest Hispanic subgroups in the U.S.
Join the Webinar Series – Crack the Cultural Code with Lorena Drago, MS, RD, CDCES
We are excited to share our guest blog post by multicultural nutrition expert, Lorena Drago, MS, RD, CDCES. In addition to creating an amazing 6-week series that provides participants with tools, including live cook-alongs, that highlight the foods and traditions from the six largest Hispanic subgroups in the U.S. Lorena is a great story teller, plus, she is offering a $30 discount for her program series which starts November 2nd. Thanks Lorena for your sense of humor and your determination to get this spicy conversation going!
All Hispanic people like spicy foods, right?

Actually…
Funny story. I was eating a family-style meal with colleagues recently and took a bite from a dish that was spicy hot. I said, “Ooo – not for me. This is too hot.”
They looked at me and asked incredulously, “Aren’t you Latina?”
Yes, I am.
“Didn’t you grow up eating hot and spicy foods?”
No, I did not. I am Colombian.
“Don’t you eat hot foods in Colombia?”
No, we don’t. What we eat depends on the region in which you live. We have nine regions in Colombia, and I was raised in the Caribbean region. Therefore, the food that I tend to eat differs from the Pacific, Andean, Amazonian and other regions in the country.
We laughed over this, and a conversation about culture and food preferences ensued.
Many of us make assumptions about what our clients, including Hispanics, eat. What if you had a solid understanding of the food and culinary preferences of the six major Hispanic subgroups in the U.S.? You can! It’s time to Crack the Cultural Code!
This 6-week program is for YOU; dietitians, nurses, pharmacists, and for all those who provide counseling to the Hispanic population and are asked, “what can I eat now?” Join us if you wish to improve healthcare outcomes for the Hispanic clients you serve who are at risk of chronic diseases, including diabetes. This program will provide you with the tools to counsel clients from the six largest Hispanic subgroups in the U.S. Improve health outcomes. Learn the nuances, food preferences and culinary know-how to confidently counsel your Hispanic clients.
Register now: “Breaking the Cultural Code: How to Counsel the Hispanic Population, Featuring the Cultures and Cuisines of Mexico, Puerto Rico, Dominican Republic, Cuba, El Salvador, and Guatemala” 12 CEUs available
Lorena specializes in the multicultural aspects of diabetes self-management education and is an expert in developing culturally and ethnically oriented nutrition and diabetes education materials. She founded, Hispanic Foodways which received the New York City Small Business Award in 2006. She developed the Nutriportion™ Measuring Cups that has the calorie and carbohydrate amounts of common foods embossed on each cup and the Nutriportion™ Hispanic Food Cards that have pictures and nutrition composition of common Hispanic foods.
Lorena served on the American Association of Diabetes Educators board of directors from 2006-2010, Chair for Latinos and Hispanics in Dietetics and Nutrition. She was Past President of the Metropolitan New York Association of Diabetes Educators in 2004. Lorena won the Diabetic Living People’s Choice Award in 2012 and Latinos & Hispanics in Dietetics and Nutrition Trinko Award in 2016.
She is the author of the book Beyond Rice and Beans: The Caribbean Guide to Eating Well with Diabetes published by the American Diabetes Association. She is a contributing author and co-editor of the book Cultural Food Practices published by the Academy of Nutrition and Dietetics and was print communications chair for the Diabetes Care and Education Specialty Practice Group of the Academy of Nutrition and Dietetics from 2012-2015.
Read more here about Lorena and Cracking the Cultural Code
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]
We are excited to share our guest blog post by multicultural nutrition expert, Lorena Drago, MS, RD, CDCES. In addition to creating an amazing 6-week series that provides participants with tools, including live cook-alongs, that highlight the foods and traditions from the six largest Hispanic subgroups in the U.S. Lorena is a great story teller, plus, she is offering a $30 discount for her program series which starts November 2nd. Thanks Lorena for your sense of humor and your determination to get this spicy conversation going!
All Hispanic people like spicy foods, right?
Actually…
Funny story. I was eating a family-style meal with colleagues recently and took a bite from a dish that was spicy hot. I said, “Ooo – not for me. This is too hot.”
They looked at me and asked incredulously, “Aren’t you Latina?”
Yes, I am.
“Didn’t you grow up eating hot and spicy foods?”
No, I did not. I am Colombian.
“Don’t you eat hot foods in Colombia?”
No, we don’t. What we eat depends on the region in which you live. We have nine regions in Colombia, and I was raised in the Caribbean region. Therefore, the food that I tend to eat differs from the Pacific, Andean, Amazonian and other regions in the country.
We laughed over this, and a conversation about culture and food preferences ensued.
Many of us make assumptions about what our clients, including Hispanics, eat. What if you had a solid understanding of the food and culinary preferences of the six major Hispanic subgroups in the U.S.? You can! It’s time to Crack the Cultural Code!
This 6-week program is for YOU; dietitians, nurses, pharmacists, and for all those who provide counseling to the Hispanic population and are asked, “what can I eat now?” Join us if you wish to improve healthcare outcomes for the Hispanic clients you serve who are at risk of chronic diseases, including diabetes. This program will provide you with the tools to counsel clients from the six largest Hispanic subgroups in the U.S. Improve health outcomes. Learn the nuances, food preferences and culinary know-how to confidently counsel your Hispanic clients.
Register now: “Breaking the Cultural Code: How to Counsel the Hispanic Population, Featuring the Cultures and Cuisines of Mexico, Puerto Rico, Dominican Republic, Cuba, El Salvador, and Guatemala” 12 CEUs available
Lorena specializes in the multicultural aspects of diabetes self-management education and is an expert in developing culturally and ethnically oriented nutrition and diabetes education materials. She founded, Hispanic Foodways which received the New York City Small Business Award in 2006. She developed the Nutriportion™ Measuring Cups that has the calorie and carbohydrate amounts of common foods embossed on each cup and the Nutriportion™ Hispanic Food Cards that have pictures and nutrition composition of common Hispanic foods.
Lorena served on the American Association of Diabetes Educators board of directors from 2006-2010, Chair for Latinos and Hispanics in Dietetics and Nutrition. She was Past President of the Metropolitan New York Association of Diabetes Educators in 2004. Lorena won the Diabetic Living People’s Choice Award in 2012 and Latinos & Hispanics in Dietetics and Nutrition Trinko Award in 2016.
She is the author of the book Beyond Rice and Beans: The Caribbean Guide to Eating Well with Diabetes published by the American Diabetes Association. She is a contributing author and co-editor of the book Cultural Food Practices published by the Academy of Nutrition and Dietetics and was print communications chair for the Diabetes Care and Education Specialty Practice Group of the Academy of Nutrition and Dietetics from 2012-2015.
Read more here about Lorena and Cracking the Cultural Code
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]
Our October 12th Question of the week quizzed test takers on the best strategy for a 90-year-old who states “they feel hungry” all the time. 76% of respondents, chose the best answer. We are excited to share this rationale of the week, so you can advocate for people living with diabetes.
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer below: Answer Question
Question: HM is living with type 2 diabetes and is 90 years old with a BMI of 32. HM’s most recent A1c was 9.6% and their GFR is 16. The provider stopped the metformin due to the diminished kidney function and HM is currently on no diabetes medications. To manage HM’s blood sugar, the provider ordered a low-calorie restrictive meal plan for HM. HM was a chef for 40 years and tells you, “they feel hungry” all the time. Based on this assessment, you decide to contact the provider.
Which of the following would be the best suggestion?
Answer Choices:
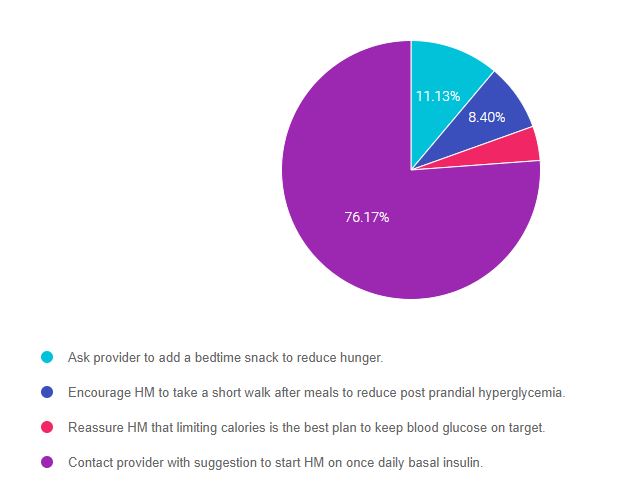
As shown above, the most common choice was option 4, the second most common answer was option 1, then option 2, and finally option 3.
If you are thinking about taking the certification exam, it is helpful to know the goals of care and considerations for people with diabetes across the lifespan. This practice test question will set you up for success. Test writers anticipate possible answers based on the details in the question. They will wave those “juicy answers” that seem so familiar to you, right under your nose. Your job is to weed through the to choose the BEST answer.
Answer 1 is incorrect. 11.13% chose this answer, “Ask provider to add a bedtime snack to reduce hunger.” While it is true that HM is hungry, a bedtime snack is not the best solution since it might contribute to already elevated blood sugars. We need to figure out a way to get blood glucose levels to goal while providing adequate nutrition.
Answer 2 is incorrect. 8.40% of you chose this answer, “Encourage HM to take a short walk after meals to reduce post prandial hyperglycemia.” Post meal walks are an excellent way to decrease post meal blood sugars, but they most likely won’t be enough to get HM out of glucose toxicity. Given that HM’s A1c is 9.6%, the average blood sugars are around 230 mg/dl. HM will need more than post meal jaunts to get blood glucose to target.
Answer 3 is incorrect. 4.30% of respondents chose this answer, “Reassure HM that limiting calories is the best plan to keep blood glucose on target.” In this situation, we need to consider quality of life issues. Given that HM is 90 years old and they were a chef, limiting calories to the point of hunger is not a strategy that considers HM’s needs, values and wants. A better approach would be to create a person-centered solution.
Finally, Answer 4 is correct. 76.17% chose this answer, “Contact provider with suggestion to start HM on once daily basal insulin.” YES, GREAT JOB. In this situation we requested that the provider start HM on 10 units of 70/30 insulin in the morning. This simple intervention will help HM in numerous ways:
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Want to learn about this question and more as you’re studying for the CDCES Exam?
This bundle includes our CDCES Online Prep Bundle (featured above) plus the ADCES Review Guide – 5th Edition-Revised. The online bundle includes Level 1, Level 2, and Level 3 (Boot Camp), plus two bonus courses. The ADCES Review Guide offers over 480+ practice questions and is a fantastic independent study tool and comprehensive resource for the Diabetes Care and Education Specialist Exam.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
JR is 26 years old with newly diagnosed diabetes. JR keeps missing appointments and when you finally get a hold of them on the phone, they start crying and say “my life is a mess”. JR is struggling with addiction, periods of houselessness and extra weight in addition to diabetes.
Based on this information, what is the most likely barrier to JR engaging in self-care?
Click here to test your knowledge!
Want to learn about this question?
Adverse childhood experiences (ACE) are associated with an increased risk of diabetes, heart disease, cancer and a variety of other health consequences for adults. This session reviews how diabetes care and education specialists can provide screening, assessment, and trauma-informed care to individuals who experienced ACEs and are living with toxic stress. We will explore strategies to address ACES and improve outcomes for individuals and communities. Throughout, we will focus on supporting self-care with a focus on recognizing and promoting resilience.
Topics include:
Watch Webinar for FREE
This option does not come with CEs.
Purchase for $19
This includes access to the recorded version of this webinar on your Online University Student Portal and 1.0 CE.
Intended Audience: This course is a knowledge-based activity designed for individuals or groups of diabetes educators, including RNs, RDs, Pharmacists, Nurse Practitioners, Clinical Nurse Specialists, Physician Assistants, and other health care providers interested in enhancing their diabetes medication knowledge.
Instructor: Beverly Thomassian RN, MPH, CDCES, BC-ADM is a working educator and a nationally recognized diabetes expert.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.