Ready to get certified?
Free CDCES Coach App

Subscribe
eNewsletter
Embark Trial Reveals Results – Spoiler Alert
The results of the EMBARK Trial are in! Spoiler Alert: These findings will change your practice approach.
As a Diabetes Educator who participated in the EMBARK trial, I have first-hand experience with the three different approaches used in this study to address diabetes distress and glucose levels for adults living with type 1 diabetes. I am surprised by the findings and excited to share them.
But before I describe the study and its results, there is a spoiler alert—the research results might compel you to adjust your practice approach.
First, let’s start with some background information.
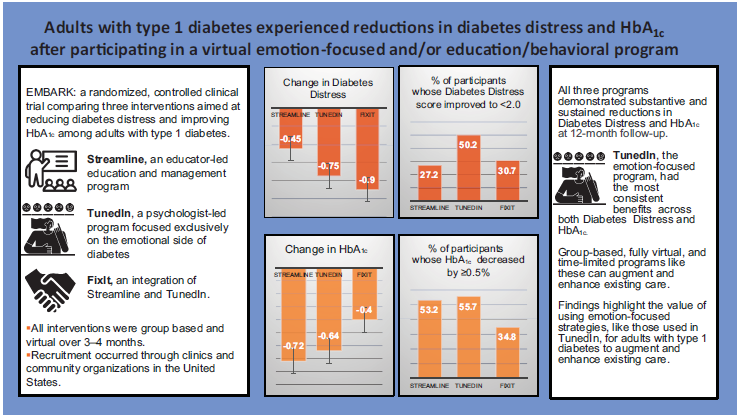
The EMBARK (Behavioral Approaches to Reducing Diabetes Distress and Improving Glycemic Control) study was a 12-month randomized, controlled intervention trial for adults with type 1 diabetes. It directly compared the impact of three highly focused interventions designed to reduce both Diabetes Distress and A1C levels among adults with Type 1 Diabetes.
The trial divided participants into three groups: Streamline, FixIt, and TunedIn. As a diabetes educator, I participated in the Streamline and FixIt study groups. As part of the study protocol, each participant completed the Diabetes Distress Scale and the results were shared with the study facilitators.
- In the Streamline educator-led intervention, we instructed individuals with type 1 to get glucose to target through group training, phone calls, and the use of unique glucose logs that promote problem-solving and self-discovery. The group training provided a brief diabetes review focused on basal insulin and bolus dosing and timing, followed by a structured five-step program to identify and resolve the specific glucose challenges identified by each participant.
- The Diabetes Educators weren’t involved in the TunedIn intervention group. TunedIn was a psychologist-led program that exclusively targeted the problematic feelings, beliefs, and expectations that underlie diabetes distress. The psychologists led a virtual group workshop followed by individual phone calls, during which they discussed areas of distress and guided participants through a structured conversation to address and reduce distress.
- The third group, FixIt, involved both diabetes educators and diabetes psychologists and combined both the Streamline and TunedIn approaches into a single, integrated program.
Which Intervention Worked Best?
As a diabetes educator involved in the Streamline and FixIt groups, I was sure that the FixIt group would have the best outcomes, given that they received the “Rolls-Royce” of interventions, which included several group sessions and one-on-one coaching by a team of psychologists and diabetes educators. However, I was wrong. The psychologist-led “TunedIn” had the best overall outcomes.
Results: TunedIn, an emotion-focused program, had the most consistent overall benefits when considering both Diabetes Distress and A1C (see infographic below).
The findings suggest the value of using emotion-focused strategies, like those in TunedIn, to reduce diabetes distress and enhance management among adults with diabetes. In truth, the findings reveal that all three groups experienced improvement in A1C and Diabetes Distress. These results suggest that both management- and emotion-focused group programs for adults with type 1 diabetes can lead to significant and clinically meaningful reductions in Diabetes Distress and A1C.
As healthcare professionals, we tend to focus on problem-solving around lifestyle, medications, and glucose levels. The results of this study confirm our intuition to prioritize addressing emotions to support individuals living with diabetes.
Let’s reprioritize our checklist of diabetes topics and move into the heart of providing effective diabetes care by assessing and addressing distress.
This emotion-based approach aligns with the 2024 American Diabetes Standards, which recommend annually assessing Diabetes Distress. These important study results remind and prompt us to assess and address Diabetes Distress to improve diabetes care outcomes. The ADA created a wonderful resource, the ADA Behavioral Health Toolkit, which houses diabetes distress and other screening tools for easy reference.
We can incorporate three main approaches underlying this study into our clinical practice (from Embark Trial Article).
- Take a diabetes education and management approach that focuses on fostering self-management change. This strategy assumes that people will become less distressed as they engage more effectively with their management.
- Incorporate an emotional approach. One key to improving glycemic outcomes is to directly address the feelings, beliefs, and expectations that underlie diabetes distress and serve as barriers to management change. This strategy recognizes that diabetes distress acts as a brake on the application of existing diabetes knowledge and skills and on one’s ability to benefit from new educational and behavioral interventions. By releasing the diabetes distress brake through emotion-focused intervention, the negative cycle can be efficiently ended.
- Use an integrated approach that combines an education and management approach with a diabetes distress emotion-centered approach. This capitalizes on the strengths of each, leading to a more effective and efficient strategy for reducing diabetes distress and improving glycemic management.
The year I spent coaching study participants in the Embark Trial significantly changed my approach to diabetes self-management coaching. In preparation for the study intervention, we were fortunate to be mentored by two experts in the field of diabetes distress: Susan Guzman, PhD, and Larry Fisher, PhD. Their wisdom and role-modeling of empowering individuals to discover new approaches to self-management were truly remarkable.
As a result of the Embark training and the Study results, I have finally given myself permission to make addressing the emotional aspects of diabetes a priority. ~Coach Beverly
(image from Embark Trial Study).
Embark Trial Study
Danielle M. HesslerLawrence FisherSusan GuzmanLisa StryckerWilliam H. PolonskyAndrew AhmannGrazia AleppoNicholas B. ArgentoJoseph HenskeSarah KimElizabeth StephensKatherine GreenbergUmesh Masharani; EMBARK: A Randomized, Controlled Trial Comparing Three Approaches to Reducing Diabetes Distress and Improving HbA1c in Adults With Type 1 Diabetes. Diabetes Care 2024; dc232452. https://doi.org/10.2337/dc23-2452
If you are interested in providing a FREE Diabetes Distress program led by a team of experts for the health care professionals in your facility, Please download this Diabetes Distress Flyer for more info!

Food Insecurity and Food Programs

3 Ways Companion Pets Can Support People with Diabetes

Structure & Routine

Animals like a routine and need structure. Many know when their feeding time or play/exercise time is and will alert you to when those times are coming up. A pet’s routine can also be used by people living with diabetes to schedule their own meal times, medication schedules, and times for exercise. In fact, 47% of pet owners surveyed said that their pets keep them more active.
The American Hearth Association has this great handout for ways pets can motivate us to be more active.
Isolation & Loneliness
A study published by BMC Public Health that assessed the relationship between loneliness and blood glucose control in diabetes found that “systolic blood pressure was significantly correlated with loneliness in patients with diabetes.”
For people living with diabetes, pets can provide company, love, and nonhuman social support. Having animals can also connect us with others, such as going to the park with your dog, riding horses with others, or joining a pet group on social media.
Stress Reduction & Mood

Last year, the American Heart Association conducted a survey for their Healthy Bond for Life program which showed that “95% of pet parents rely on their pets for stress relief.” For those who experience diabetes distress, spending time petting an animal, watching them play, and snuggling up with them may help in times of stress.
Animal-assisted interventions have also been shown to have positive outcomes for those experiencing depression, PTSD, and anxiety.
How to Keep You and Your Pet Healthy
While there are many benefits to owning a pet, it is important to be aware of how to keep you and your pet safe. The CDC’s “Healthy Pets, Healthy People” hub has helpful information and resources on pet safety.

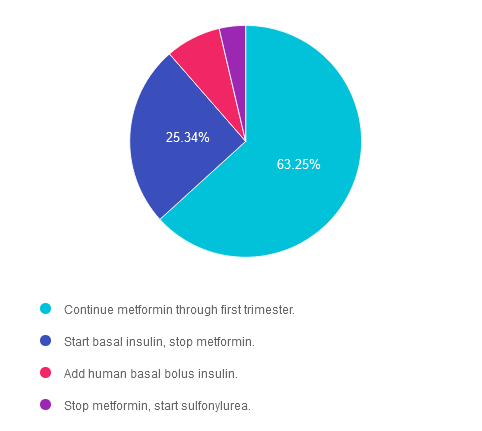
Rationale of the Week | KR is on Metformin & 4 Weeks Pregnant. Best action?

Question of the Week | What is the cause of this emergency room visit?

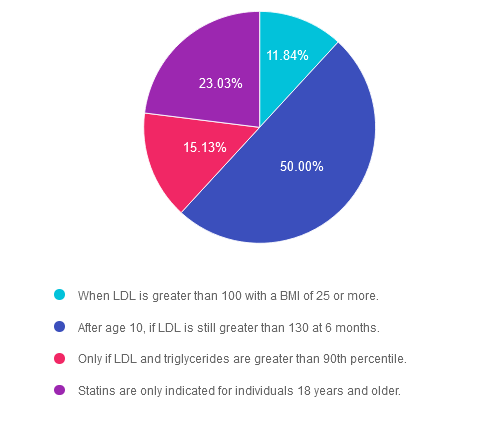
Rationale of the Week | Are statins indicated for Peds with Diabetes?
Question of the Week | KR is on Metformin & 4 Weeks Pregnant. Best action?
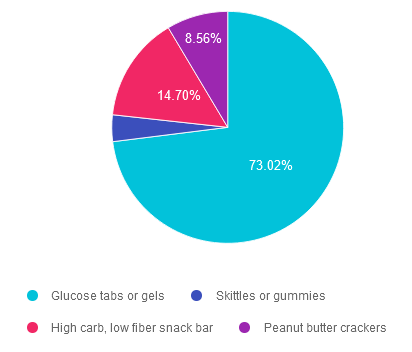
Rationale of the Week | Best treatment for Hypoglycemia with Gastroparesis