Ready to get certified?
Free CDCES Coach App

Subscribe
eNewsletter
Question of the Week | Euglycemic DKA – What is Best Intervention?


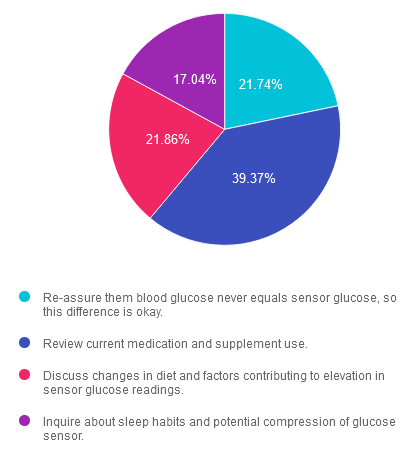
Rationale of the Week | Why are CGM readings higher than BG readings?

Want to learn more about this question?
Virtual DiabetesEd Training Conference – Join us Live on April 17th – 19th 2024 at 11:30 AM PST

Join Coach Beverly and Team for two and a half days of knowledge-sharing, fun, and “aha” moments for our Virtual DiabetesEd Training Conference April 17th – 19th, 2024.
Attendees will leave this conference with new tools and a refreshed understanding of the latest advances in person-centered diabetes care. Our team highlights the ADA Standards of Care, medications, behavior change, technology, medical nutrition therapy, and more!
Our instructors co-teach the content to keep things fresh and lively.
Friend Discount: 3 or more only $449 per person. Email us at [email protected] with the name and email of each registrant to get the discount!
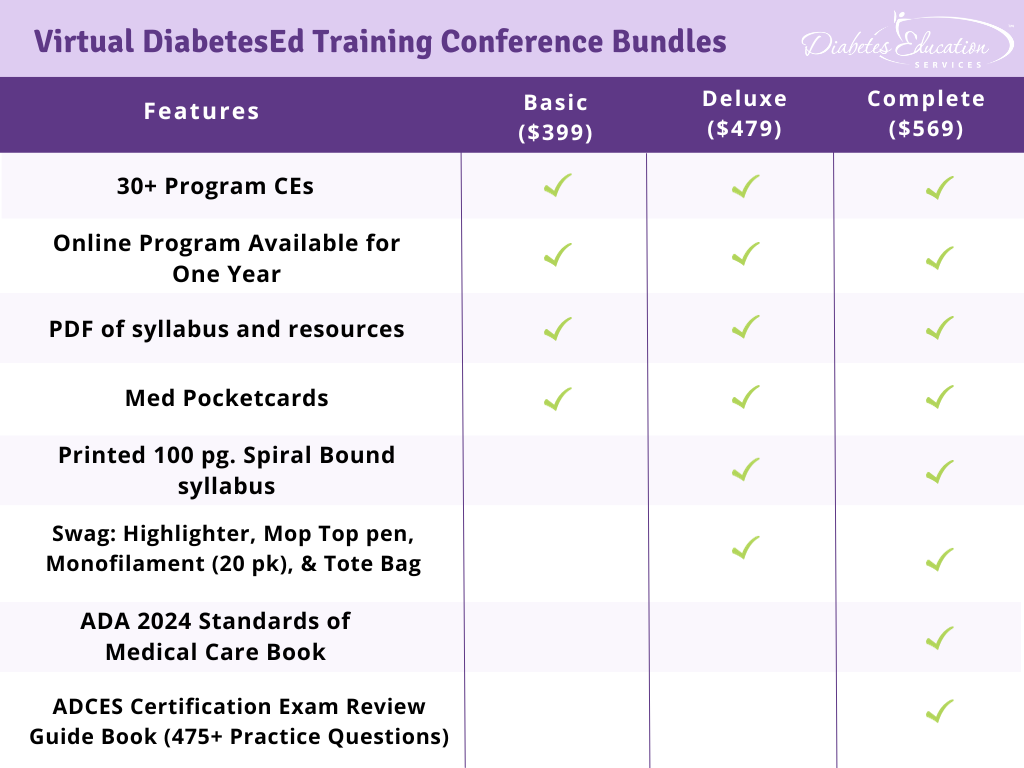
Program Details
- Dates: April 17-19th, 2024
- Registration Fee: $399-$569 (see more about reg. options below)
- Friend Discount: For 3 or more people, each person saves $50 off their registration. Email us at [email protected] with the name and email of each registrant to get the discount!
- CEs: 30+ CEs | 18 units for Virtual Conference plus 10+ Bonus CEs. CEs can be applied toward CDCES’s initial application or renewal.
- Speakers: View Conference Faculty
Registration Options
Question of the Week | JR is out of lispro (Humalog) insulin and is panicking.

April 2024 eNews | Does Yogurt Reduce Risk of Type 2 Diabetes? Liver Disease & Diabetes: A Call to Action, First Over-the-Counter CGM!
Happy April
|
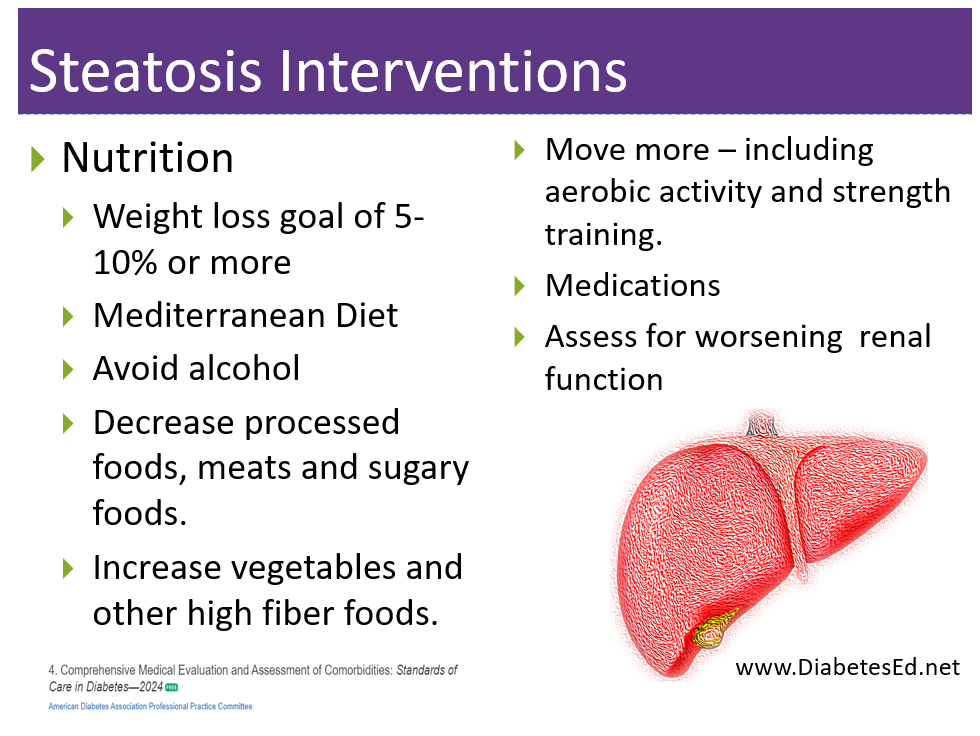
With the emerging sunshine and nature in bloom, it feels like a personal invitation to awaken from the winter slumber and take an outdoor stroll or enjoy the simple pleasure of planting. To celebrate Earth Day on April 22nd, we highlight how to incorporate native plants into daily life and support healthy ecosystems. Our nutrition expert explores how yogurt decreases the risk of type 2 diabetes and dives into the science of this century’s old favorite food. We discuss the importance of screening for undetected liver disease to provide early and focused treatment to prevent progression to liver failure. In addition, we feature a new FDA approved medication that treats liver disease and fibrosis with a list of diabetes medications that also offer effective treatment. The new over-the-counter sensor, Stelo, is FDA-approved and should be available for purchase in late summer. We examine its features and limitations. Our first “Connect with Coach Beverly” was a big hit, so we are offering it again in April. You are invited to submit your questions and join our lively discussion. For our Question of Week Section, we ask, “Why don’t the CGM and meter reading match? And “What is the best treatment for steatosis?” Test your knowledge and prepare for exam success. We are thrilled to offer our Free Webinars on CDCES and BC-ADM Prep, plus a bunch of other great programs. Hope to see you there. |
|
Sending notes of joy and health, Coach Beverly and Bryanna |
Featured Articles
- Does Yogurt Reduce Type 2 Risk?
- Liver Disease & Diabetes: A Call to Action:
- First OTC Sensor FDA Approved
- Earth Day Celebration
- Coach Beverly Connects – Airs April 23rd
- Question of the Week #1
- Question of the Week #2
Upcoming Webinars
- Microvascular Disease – Reducing Risk on April 11th
- Cardiovascular Disease & Diabetes – April 13
- Virtual DiabetesEd Training Conference – April 17-19
- ReVive 5 – May 22nd & 29th
Upcoming Events – See the complete calendar listing
Virtual DiabetesEd Training Conference – Join us Live on April 17th – 19th 2024 at 11:30 AM PST
Join Coach Beverly and Team for two and a half days of knowledge-sharing, fun, and “aha” moments for our Virtual DiabetesEd Training Conference April 17th – 19th, 2024.
Attendees will leave this conference with new tools and a refreshed understanding of the latest advances in person-centered diabetes care. Our team highlights the ADA Standards of Care, medications, behavior change, technology, medical nutrition therapy, and more!
Our instructors co-teach the content to keep things fresh and lively.
Friend Discount: 3 or more only $449 per person. Email us at [email protected] with the name and email of each registrant to get the discount!
Program Details
- Dates: April 17-19th, 2024
- Registration Fee: $399-$569 (see more about reg. options below)
- Friend Discount: For 3 or more people, each person saves $50 off their registration. Email us at [email protected] with the name and email of each registrant to get the discount!
- CEs: 30+ CEs | 18 units for Virtual Conference plus 10+ Bonus CEs. CEs can be applied toward CDCES’s initial application or renewal.
- Speakers: View Conference Faculty
- Conference Schedule >
- Conference Flyer >
Click Here for Registration Options
Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and our CPEU courses have received Prior Approval* from the Commission of Dietetic Registration (CDR), Provider DI002. Since our CPEU courses received Prior approval* from the CDR, these CPEU courses satisfy the CE requirements for the CDCES /BC-ADM regardless of your profession!
The use of DES products does not guarantee the successful passage of the certification exam. CBDCE and ADCES do not endorse any preparatory or review materials for the CDCES or BC-ADM exams, except for those published by CBDCE & ADCES.
AHHA Study – Recruiting People Living with Type 2 Diabetes
Innovative Diabetes Education Program: AHHA Study
A NEW research opportunity for people with Type 2 Diabetes
Are you a diabetes health care professional or person with diabetes who is ready to get on track with your diabetes?
We want to encourage you to let your community know about an exciting research opportunity.
We are inviting people diagnosed with type 2 diabetes less than 5 years ago, who live anywhere in the U.S., with a most recent A1C of 7.5% or higher to click this link below to see if they qualify for the study.
If so, the Behavioral Diabetes Institute is conducting a research study examining how innovative new approaches to diabetes education might help to improve glucose outcomes and quality of life outcomes. Participants will be randomly assigned to take part in one of two different live, online, group education programs. Each group program will be lively and informative, and will meet once weekly for 5 weeks in a row.
Also, half of the participants will receive a continuous glucose monitor and free testing supplies.
To find out more and see if you might qualify, click below to apply. Or for more information, email them at [email protected] or call us at 858-336-8693.
Get Started – Pre-Qualify Here
Rationale of the Week | Which statement is accurate regarding treatment of steatosis?
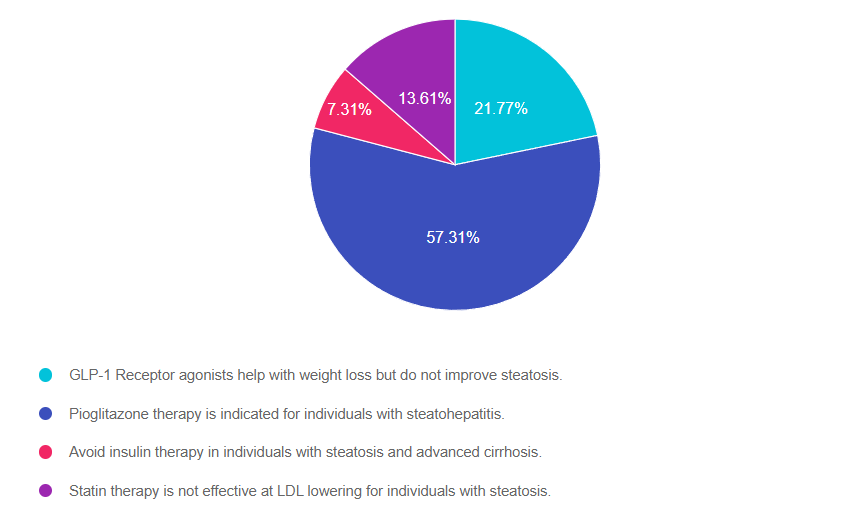
Answer 1 is incorrect. 21.77% chose this answer. “GLP-1 Receptor agonists help with weight loss but do not improve steatosis.” This juicy answer is tempting, but it is not the best answer. GLP-! RA’s, lower blood glucose levels and they also promote significant weight loss. This results in less glucose toxicity and a decrease in hepatic fat storage. Plus, they decrease the risk of cardiovascular disease which is co-associated with steatosis. See our Meds for Liver Disease Blog for more info.
Answer 2 is correct. 57.31% of you chose this answer. “Pioglitazone therapy is indicated for individuals with steatohepatitis.” Yes, this is the best answer. Pioglitazone (Actos) reduces blood glucose, and several studies demonstrate it is an effective treatment for steatosis and steatohepatitis. It also reduces the progression of fibrosis and cardiovascular risk. Since pioglitazone can cause fluid retention and weight gain, avoid using it in those with heart failure. See our Meds for Liver Disease Blog for more info.
Answer 3 is incorrect. About 7.31% of respondents chose this. “Avoid insulin therapy in individuals with steatosis and advanced cirrhosis.” With advanced cirrhosis, many of the oral medications may not be safe to use. The ADA recommends using insulin therapy, since it is safe and effective for people experiencing cirrhosis. Since people with cirrhosis are at higher risk of hypoglycemia, close monitoring of glucose levels is recommended. See our Meds for Liver Disease Blog for more info.
Finally, Answer 4 is incorrect. 13.61% chose this answer. “Statin therapy is not effective at LDL lowering for individuals with steatosis.” Lipid-lowering and antihypertensive meds need to be prescribed in people with steatosis as indicated. Statins are safe in individuals with steatohepatitis but avoid their use in those with decompensated cirrhosis. See our Meds for Liver Disease Blog for more info.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Question of the Week | Why are CGM readings higher than BG readings?

Person-Centered Coaching; A Step-by-Step Approach
Person-Centered Coaching – A Step-by-Step Approach
People with diabetes experience a myriad of feelings as they utilize new technologies and try to make sense of all the data and new information. As diabetes healthcare providers, we can learn to address these feelings through person centered coaching and help individuals take steps to get to their best health. This approach not only acknowledges the individual’s feelings but also empowers them to take steps towards their optimal health.
This article equips healthcare professionals with a dozen practical coaching strategies. These strategies are designed to instill confidence in individuals with diabetes, fostering their belief in their ability to successfully self-manage their condition.

Using a person-centered approach, we can identify the individual’s strengths and expertise and then leverage this information to open a door of possibilities. Our choice of communication techniques can spark behavior change in people living with diabetes.
Adopting a person-centered approach may require a significant adjustment for some healthcare providers. In traditional care, the provider assumes the role of the captain, steering the ship, providing the fuel, and plotting the course. However, in person-centered coaching, the provider becomes the rudder, guiding the individual while they steer their own course towards better health.
For this conversation, we imagine someone struggling with technology-related diabetes distress after switching from checking blood sugars using a meter to trying to make sense of the data being generated by their new CGM.
DO: Mindfully Listen to the individuals’ problems and fears.
The first strategy is carefully listening to the person’s fears and concerns. If someone struggles with nutrition, meds, or behavioral changes, listen to the struggle and try not to push, advise, or fix it. Listen and reflect on what you think is happening for the first few minutes.
For example, reflecting back could go something like this:
“Taking insulin each meal is hard for you because you are worried about taking too much.” OR
“It’s hard not to constantly check your blood sugar on your CGM because you are worried that it is going above range.” OR
“It sounds like you blame yourself for having blood sugars that are above target.”
Listening and reflecting on the individual’s struggles is the first phase of energizing the visit.
DO: Focus on curiosity before exploring possible changes in behavior.
With a person-centered approach, spend more time in the “curiosity” phase before moving to the “action” phase.”
We might ask the person who feels worried about elevated blood sugars, “I am curious to learn more about your feelings when blood sugars go above target.”
As care providers, we may be slightly overanxious to get to the “action” phase, which involves action, planning, goal setting, and looking at specific foods and exercise prescriptions. It can be disorienting for providers to delay the “action” phase and spend most of the time exploring the “curiosity” phase, and there’s a perception that it takes longer. In fact, it’s probably more efficient with time. It’s a redistribution of the provider’s time in that more time is spent listening to the individual’s barriers and fears and responding to them.
Curiosity can provide comfort and open the door to insights.
DO: Listen for individual insights and ideas.
After reflecting on the person’s struggles and feelings, the next phase is the “building change” talk. It combines having the person express how a behavior change would benefit them and realistic ways to move to the action phase.
As genuinely curious providers, we ask, “What are your ideas about how you can improve this situation?” Then, the provider listens carefully to what the person shares.
Along with the struggles and barriers, the individual might say,
“I will try only to check my blood sugar levels before meals and two hours after a meal instead of twenty times a day” or
“I could try adjusting my insulin dose for a week to see how that affects my blood sugars.”
We want to fine-tune our listening skills so that we can pick up the scent of the trail. People often allude to what they’re willing to do and drop crumbs when they feel safe and heard during the conversation. All we need to do is pick up on the hints and encourage them down the path.
DO: Ask Questions and Collaborate.
Once the individual has identified their motivation and begins brainstorming ways to change behavior, the door is open for respectful collaboration. You’ll want to explore how much change the individual is willing and able to make at that time.
To keep it real and achievable, we start with a tiny step by saying,
“So, you think you could limit checking your blood sugars to about eight times a day?” or
“You think you could adjust your insulin dose for a week to see if that lowers post-meal blood sugars?” Let that sit; let the person describe their thoughts and feelings.
Then we might say, “How, if at all, do you see this plan fitting into your life?” We are careful to avoid any prescription or declaration and stick with asking questions.
If they volunteer—”I will limit checking my blood sugars on my CGM to eight times a day.” Or
“I will adjust my insulin dose to see if it lowers my post-meal blood sugars.”
We would absolutely reinforce and support these choices.
AVOID: Pressure, fix, or control.
A person-centered approach energizes individuals to take the lead in managing their condition, in step with their providers and supporters. We are careful to avoid forced solutions or controlling language. As providers, we feel we have these great ideas that will fix the person, if only…. However, the truth is, our job is to help the person with diabetes find their own answers and solutions.
Let’s stop “Shoulding” on people.
It’s time to let go of terms like “You must, you should, you have to, it’s better, it’s important, do it for me” since they fall under the category of “controlling motivation”—which can be hurtful and lead to the individual becoming defensive or shutting down. We avoid controlling language because it elicits resistance and defiance. The literature is quite clear about people doing something because someone made them feel guilty, ashamed, or pressured them. The long-term prognosis for behavior change using this approach is underwhelming.
DON’T employ Scare Tactics.
As providers, we genuinely care about people’s health and may try to energize behavior change using fear. Such as, “If you don’t get your A1C down, you are heading for dialysis or amputation.” or “Don’t you want to see your kids grow up?” We don’t generally motivate people by scaring them since research shows it is ineffective, and they may never return for that follow-up appointment.
In the short term, people are usually willing to make changes when they’re terrified—when they first get diagnosed—but that willingness wanes in a relatively short period. The question is how to energize the person when the initial fear has worn off.
In conclusion, Celebrate and Recognize Each Person’s Efforts.
Making behavior changes, like losing weight or adjusting lifelong eating habits, can be extremely difficult.
Find a way to recognize and affirm their efforts even if there is no or little change in clinical measures.
If someone’s A1C has not moved, but they decreased their CGM checks to eight times a day or adjusted their mealtime insulin, we can say, “Wow, I want to recognize the effort you put into this.”
Respond kindly and compassionately to their disappointment, frustration, and fear. It won’t fix the immediate problem but will help the person feel that their effort was well spent. It will help them feel heard instead of us just “fixing it.” Over time, your empathy will build bridges and trust, leading to long-term collaboration and better health.
Want to share this with your colleagues or have a copy for yourself?
Download a PDF of this Person Centered Step-By-Step Approach
About the author – Coach Beverly has been fine-tuning her guilt-free approach to diabetes education for over 30 years and has witnessed its impact on improving well-being and building connections.
Learn more about these effective communication approaches in our ReVive 5 Training Program.
Inspired by https://www.niddk.nih.gov/health-information/professionals/diabetes-discoveries-practice/motivational-interviewing-dos-dont