Ready to get certified?
Free CDCES Coach App

Subscribe
eNewsletter
Does Yogurt Reduce the Risk of Type 2 Diabetes?
 Does Yogurt Reduce the Risk of Type 2 Diabetes?
Does Yogurt Reduce the Risk of Type 2 Diabetes?
by Christine Craig, MS, RD, CDCES
On March 1st, 2024, the FDA announced they “do not object” to the use of the qualified health claim: “Eating yogurt regularly, at least 2 cups (3 servings) per week, may reduce the risk of type 2 diabetes according to limited scientific evidence.”1
When I learned of this announcement, my curiosity perked up; my obsession with yogurt started in the late nineties during a microbiology project in which I plated different over-the-counter yogurts and compared the growth.
I was fascinated by the relationship between probiotics and health, and I learned from my research that not all yogurts were created equal. The ADA Standards of Care have recognized the health of the microbiome is essential for preventing and treating diabetes and still, to date, no specific recommendation has been stated regarding inclusion of yogurt. Probiotics have many beneficial effects, including enhancing the immune system, treating diarrhea, lowering cholesterol, and treating IBD and IBS.
But what about yogurt and diabetes prevention? We know there is more to the microbiome health than just yogurt, but are there specific yogurts we can consider recommending? How can we apply these recommendations practically across eating patterns using person-centered care?
What does the FDA consider yogurt?
The term yogurt likely originates from the Turkish term “yogurmak”, which means to thicken, coagulate, or curdle.2 Although modern times have updated how it is packaged (including many flavors, stabilizers, and texture enhancements), yogurt originated from 5000-10,000 BC when milk was packed into stomach lining sacks, and the curdling process that resulted, served as a natural preservative.2 Today, yogurt is defined by the FDA as a cultured food of one or more basic dairy ingredients, cultured with lactobacillus bulgaricus (l. bulgaricus) and streptococcus thermophilus bulgaricus (s. thermophilus). Probiotic yogurts may contain additional strains of bacteria, such as bifidobacterium lactis or lactobacillus acidophilus but, on the shelf, you can find yogurts with many other probiotic strain additives.
Yogurt, by definition, has a pH of 4.6 or lower and is allowed to be treated after culturing to inactivate viable microorganisms and extend shelf-life.3 However, those treated after culturing must state on the label “does not contain live and active cultures,” and those containing “live and active cultures” must have a minimum of 106 CFU at self-life expectation. Nutritionally, yogurt is a good source of calcium, phosphorus, potassium, Vitamin A, B2, and B12 and has about 8 grams of protein per cup in conventional yogurts.
What is the evidence for diabetes prevention?
Five meta-analyses and additional observation studies were reviewed within the petition to the FDA.4 The most recent, 2016 meta-analysis reviewed 22 prospective cohort studies completed within 4 countries of origin.5 Eleven of the studies evaluated yogurt and they reported a 14% lower type 2 diabetes risk when including at least 80 grams of yogurt per day (~1/3 cup). They found greater significance and confidence within subpopulations, including women or older (>60) adults. Most studies included conventional yogurts with mixed fat content (some including low-fat while others regular-fat). The amount of added sugar or product type (plain vs. sugar-sweetened yogurt) was not reported. We cannot state a specific type of yogurt that resulted the most significant difference. The FDA, in their statement, called out caution regarding high-sugar yogurt products due to potential concern of contributing to excessive sugar consumption, but no restriction was placed on the allowable claim due to the limited evidence.
The qualified health claim applies to food-based products and not supplements.4 We also need to find out if different types of yogurts, including higher protein or plant-based varieties, would have similar outcomes.
Glycemic Benefits of Yogurt in Type 2 Diabetes Management
A 2019 meta-analysis of yogurt’s effects and glycemic outcomes in persons diagnosed with type 2 diabetes reviewed nine randomized control trials.6 Yogurt types included mainly probiotic dairy yogurt (L. acidophilus, B. lactis) but also one from goat milk and one from kefir. They reported that probiotic yogurt showed no significant difference in improving HgbA1c, fasting insulin, fasting glucose, and insulin resistance. However, kefir did show a significant difference in A1c and fasting blood glucose reduction. Again, this meta-analysis did not differentiate between low and regular-fat yogurt nor plain and sweetened yogurts. The analysis also did not consider the synergistic effects of other foods to enhance outcomes nor measured microbiome changes. More studies are needed to include larger populations and differentiation of subpopulations that may show benefit.
Can we suggest any yogurt variety?
In 2023, the US yogurt market grew to a 9.38-billion-dollar industry, with growth in yogurt varieties, including higher protein (Greek, Icelandic type, etc.) and plant-based dairy-alternative yogurt products. Higher protein yogurt varieties are generally lower in sugar and almost double the protein at 15-18 grams per serving, they contain about 10-20% of Vitamin D and Calcium. Plant-based yogurts vary in comparable nutrient content, ranging from 11-20 (or more) grams of carbohydrate, 1-8 grams of protein per serving, 2-20% Calcium, 0-10% Vitamin D, and 0-40% B12, and they typically contain live active cultures.7 To date, limited studies have been conducted on these products and health outcomes. The variety of yogurt products on the shelf does not match the data evaluated within the FDA petition meta-analysis. Yet, it is essential to support individuals with or at risk of diabetes who choose a plant-based dairy alternative that meets their specific nutrient needs.
The ADA Standards of Care and referenced dietary patterns including the Mediterranean Diet, DASH diet, and general healthful eating patterns recommend including 2-3 servings of dairy per day. These eating patterns also recommend limiting added sugars and high-fat dairy. The meta-analysis results do not provide enough information to suggest a specific type of yogurt, so we can work with individuals to learn their dietary patterns and determine if yogurt may be a good substitute or encouraged current food choice. We can assess an individual’s total fat and sugar intake to determine if yogurt is a significant contributor and can find an appropriate option that supports overall dietary patterns and individual metabolic goals. The microbiome’s health is dynamic, and specific food recommendations will likely be synergistic.
Like a healthy plate, no single food or one-size-fits-all approach is appropriate and as we learn more, many functional food options can be relevant to recommend.
References:
1. FDA Announces Qualified Health Claim for Yogurt and Reduced Risk of Type 2 Diabetes. Downloaded on March 12, 2024 from https://www.fda.gov/food/cfsan-constituent-updates/fda-announces-qualified-health-claim-yogurt-and-reduced-risk-type-2-diabetes
2. Hadjimbei E, Botsaris G, Chrysostomou S. Beneficial Effects of Yoghurts and Probiotic Fermented Milks and Their Functional Food Potential. Foods. 2022 Sep 3;11(17):2691.
- CFR-Code of Federal Regulations Title 21: Food and Drugs: Part 131 Milk and Cream. Downloaded on March 13th, 2024. https://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfcfr/CFRSearch.cfm?fr=131.200&SearchTerm=yogurt
- Petition for the Authorization of a Qualified Health Claim for Yogurt and Reduced Risk of Diabetes downloaded on March 12, 2024 from https://www.regulations.gov/document/FDA-2019-P-1594-0001
- Gijsbers L, Ding EL, Malik VS, de Goede J, Geleijnse JM, Soedamah-Muthu SS. Consumption of dairy foods and diabetes incidence: a dose-response meta-analysis of observational studies. Am J Clin Nutr. 2016 Apr;103(4):1111-24
- Barengolts E, Smith ED, Reutrakul S, Tonucci L, Anothaisintawee T. The Effect of Probiotic Yogurt on Glycemic Control in Type 2 Diabetes or Obesity: A Meta-Analysis of Nine Randomized Controlled Trials. Nutrients. 2019 Mar 20;11(3):671.
- Craig WJ, Brothers CJ. Nutritional Content and Health Profile of Non-Dairy Plant-Based Yogurt Alternatives. Nutrients. 2021 Nov 14;13(11):4069.

Diabetes Disparities in the Black Community

Question of the Week | Best action to address sudden Hyperglycemia due to Cellulitis?
RL is 83, has Latent Autoimmune Diabetes, and takes degludec 17 units every morning along with metformin 500 XR twice daily. RL tells you that their left leg was suddenly swollen and red, so they went to urgent care and were started on a course of antibiotics. In the meantime, their CGM is showing elevated blood sugars in the 200 to 350 range during the day but often less than 100 at night. RL weighs 70kg, with a BMI of 23.4.
Based on this information, what action do you suggest?
- Decrease carbohydrate intake by 20-25% until the infection subsides.
- Increase the degludec by 20% to get blood glucose levels to target.
- Encourage RL to walk after meals to decrease post prandial blood sugar levels.
- Suggest initiation of bolus insulin once or twice daily.
Click Here to Test your Knowledge
Want to learn more about this question?
Virtual DiabetesEd Training Conference – Join us Live on April 17th – 19th 2024 at 11:30 AM PST

Join Coach Beverly and Team for two and a half days of knowledge-sharing, fun, and “aha” moments for our Virtual DiabetesEd Training Conference April 17th – 19th, 2024.
Attendees will leave this conference with new tools and a refreshed understanding of the latest advances in person-centered diabetes care. Our team highlights the ADA Standards of Care, medications, behavior change, technology, medical nutrition therapy, and more!
Our instructors co-teach the content to keep things fresh and lively.
Friend Discount: 3 or more only $449 per person. Email us at [email protected] with the name and email of each registrant to get the discount!
Program Details
- Dates: April 17-19th, 2024
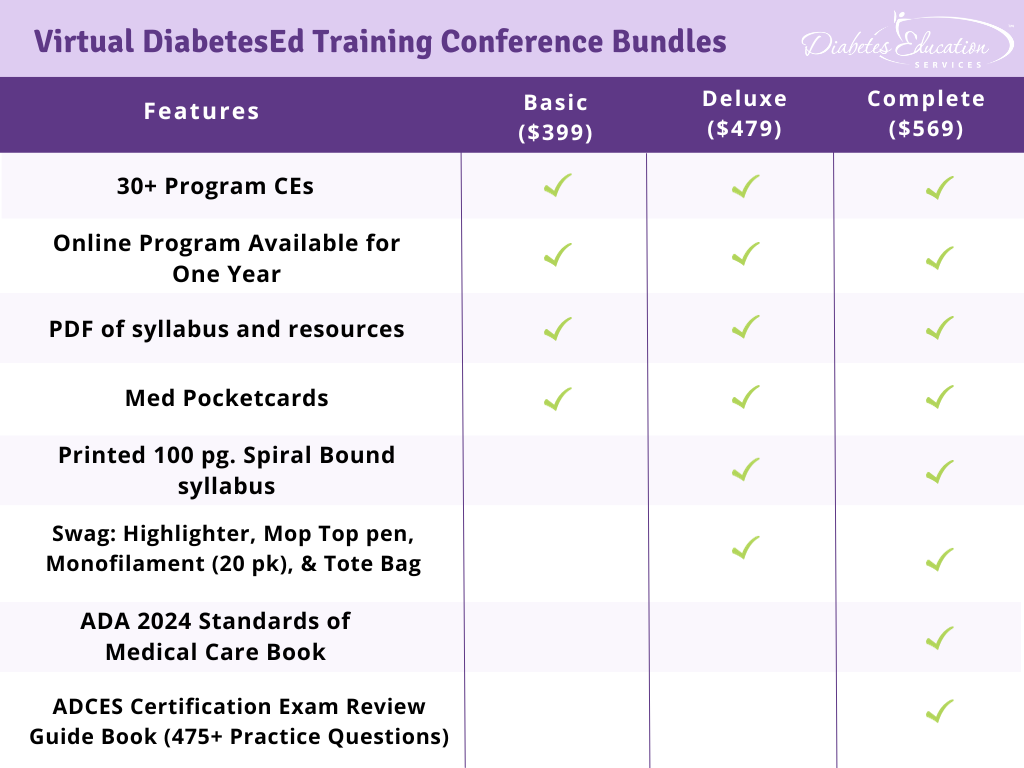
- Registration Fee: $399-$569 (see more about reg. options below)
- Friend Discount: For 3 or more people, each person saves $50 off their registration. Email us at [email protected] with the name and email of each registrant to get the discount!
- CEs: 30+ CEs | 18 units for Virtual Conference plus 10+ Bonus CEs. CEs can be applied toward CDCES’s initial application or renewal.
- Speakers: View Conference Faculty
Registration Options
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and our CPEU courses have received Prior Approval* from the Commission of Dietetic Registration (CDR), Provider DI002. Since our CPEU courses received Prior approval* from the CDR, these CPEU courses satisfy the CE requirements for the CDCES /BC-ADM regardless of your profession!
The use of DES products does not guarantee the successful passage of the certification exam. CBDCE and ADCES do not endorse any preparatory or review materials for the CDCES or BC-ADM exams, except for those published by CBDCE & ADCES.
Big Change to CDCES Exam – Less Test Questions & Different Outline starting in July

We are excited to announce the most significant change to the CDCES Exam in the past 30 years (besides moving to computer testing from scantrons). If you plan on taking the CDCES exam after June 30, 2024, there will be fewer total questions and an increased focus on diabetes care and interventions.
The Certification Board for Diabetes Care and Education (CBDCE) handbook states that only 175 questions are needed, instead of 200, to evaluate if an individual has adequate expertise and mastery of the test content.
If you are taking the test through June 30, you can expect the same number of questions, 200 multiple-choice questions, using the current CDCES test outline.
Starting July 1, there will only be 175 test questions based on an updated test outline.
Regardless of when you take the exam, certain things will remain the same.
There will still be 25 questions that are NOT counted in the final test score. These questions are scattered throughout the exam and allow for collection of meaningful statistics about new questions, but are
not used in the determination of individual examination scores.
In addition, this exam results are based on a “scaled score” to ensure that different exam versions are equally challenging. The CBDCE has made no mention of a decrease in the four hours to complete the exam, and certificants can still take the exam at a testing site or choose live remote proctoring.
With the current CDCES test outline, effective through June 30, 2024, here is how the counted 175 questions are divided by content (There are 200 questions, but only 175 count toward the final score)
- Assessment of the Diabetes Continuum – 59 questions
- Interventions for Diabetes Continuum – 88 questions
- Disease Management – 28 questions
For more details, please see the current CDCES Exam Content Outline | January – June 2024 page 21.
Starting July 1, 2024, the test outline will have significant changes. Here is how the counted 150 questions are divided by content (There are 175 questions, but only 150 count toward the final score)
- Assessment – 37 questions
- Care and Interventions – 105 questions
- Standards and Practices – 8 questions
For more details, please see the CDCES Exam Content Outline | July 1, 2024
A lot of the changes are under “Care and Education Interventions” sections on the exam content outline effective July 1, 2024. For complete eligibility and certification information, the 2024 Certification Examination for Diabetes Educators Handbook contains detailed instructions on applying, study resources, and exam content outlines.
Should I take the CDCES exam before or after the changes?
This is a great question, and Coach Beverly suggests carefully self-evaluating your testing style. If the thought of muscling through 200 questions seems overwhelming and question fatigue is an issue, consider taking the shorter version in July. However, as with any new exam, there may be some kinks to iron out, and there could be a slight delay in receiving test results in the first few months after the exam’s release, based on my experience. When there has been a test update in the past, the CBDCE took a few weeks to send the test results to test takers for a short time period.
Coach Beverly suggests basing your decision on your level of readiness. After reviewing the exam outline content, if you feel very familiar with the topics listed, plus you are scoring 80% or greater on practice exams, moving forward with the exam is a great choice. Keep in mind that the exam covers a wide breadth of information, from birth to death, plus during pregnancy, and addresses chronic and acute care in various settings. This means you will need to create a study plan that assesses knowledge gaps along with a plan to address those gaps.
Will Your Online University Courses Prepare Students for the Updated Exam Content?
Yes, absolutely. We carefully consider the exam content outlines coupled with Coach Beverly’s test-taking experience when updating our program content.
Our online course content is updated each year based on a review of the latest ADA Guidelines and the CBDCE’s exam content outline. If the ADA Standards include new or updated information that is listed in the exam outline, we plug in these new medications, MNT approaches, goals, screening guidelines etc. into the course content. A big chunk of the changes starting in July are under the “Care and Education Interventions” section. The good news is that our library of courses already focus on person-centered care and the interventions that are outlined in section II, in the Exam Content Outline | July 1, 2024.
Coach Beverly also retakes the exam every renewal cycle for her certification so she can have a student’s perspective on sitting for the exam while developing course content. We try to focus specifically on material that is relevant for the exam, considers the overall ADA Standards of Care and ultimately improves quality of care delivered to people living with diabetes.
Our goal is to provide evidence-based, clinically relevant content that will also prepare participants for exam success. We’ve got you covered.
Conflict of Interest clarification:
Our company Diabetes Education Services has no relationship with the CBDCE. All of the information posted in this blog is based on Coach Beverly’s careful review of the 2024 Certification Examination for Diabetes Educators Handbook.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and our CPEU courses have received Prior Approval* from the Commission of Dietetic Registration (CDR), Provider DI002. Since our CPEU courses received Prior approval* from the CDR, these CPEU courses satisfy the CE requirements for the CDCES /BC-ADM regardless of your profession!
The use of DES products does not guarantee the successful passage of the certification exam. CBDCE and ADCES do not endorse any preparatory or review materials for the CDCES or BC-ADM exams, except for those published by CBDCE & ADCES.
Meet Brent McMenomey – Customer Advocate and Brand Ambassador

To provide exceptional customer service as our company continues to grow, we are excited to introduce Brent McMenomey, the newest member of our team. Brent is a perfect fit for our Customer Advocate & Brand Ambassador position given his extensive background in customer service, graphic design, and marketing.
As your Customer Advocate, he will always be sure your questions are answered and your concerns addressed. He has decades of experience in troubleshooting issues, both service-related and technical, and is always happy to help!
Brent loves nature, as well as animal lover with 3 dogs (Freya, Sadie and Wesley), a few chickens and 15 finches. Brent also has a YouTube Channel dedicated to gardening and small home renovations called Visit Our Garden that he films and edits with his partner. Welcome Brent!
Virtual DiabetesEd Training Conference – Join us Live on April 17th – 19th 2024 at 11:30 AM PST
Join Coach Beverly and Team for two and a half days of knowledge-sharing, fun, and “aha” moments for our Virtual DiabetesEd Training Conference April 17th – 19th, 2024.
Attendees will leave this conference with new tools and a refreshed understanding of the latest advances in person-centered diabetes care. Our team highlights the ADA Standards of Care, medications, behavior change, technology, medical nutrition therapy, and more!
Our instructors co-teach the content to keep things fresh and lively.
Friend Discount: 3 or more only $449 per person. Email us at [email protected] with the name and email of each registrant to get the discount!
Program Details
- Dates: April 17-19th, 2024
- Registration Fee: $399-$569 (see more about reg. options below)
- Friend Discount: For 3 or more people, each person saves $50 off their registration. Email us at [email protected] with the name and email of each registrant to get the discount!
- CEs: 30+ CEs | 18 units for Virtual Conference plus 10+ Bonus CEs. CEs can be applied toward CDCES’s initial application or renewal.
- Speakers: View Conference Faculty
Registration Options
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and our CPEU courses have received Prior Approval* from the Commission of Dietetic Registration (CDR), Provider DI002. Since our CPEU courses received Prior approval* from the CDR, these CPEU courses satisfy the CE requirements for the CDCES /BC-ADM regardless of your profession!
The use of DES products does not guarantee the successful passage of the certification exam. CBDCE and ADCES do not endorse any preparatory or review materials for the CDCES or BC-ADM exams, except for those published by CBDCE & ADCES.
Question of the Week | What medication changes do you recommend?
RL was newly diagnosed 43 with type 2 diabetes 6 months ago with an initial A1C of 10.1%. They have no cardiovascular disease and their renal function is within normal limits. At a recent office visit, you notice RL’s A1C has dropped to 7.3, their BP is 112/78 and the LDL cholesterol is 103mg/dL. RL’s current medication regimen includes, rosuvastatin 10mg, empagliflozin 25mg, metformin 1000 BID, glargine 12 units and aspirin 81mg.
Based on this information, what changes to RL’s medication plan do you recommend to the provider?
- Consider increasing rosuvastatin and stopping ASA therapy.
- Consider stopping empagliflozin and starting GLP-1 RA to help with weight loss.
- Consider adding an ACE or ARB and increasing basal insulin.
- Consider increasing metformin and decreasing basal insulin.
Click Here to Test your Knowledge
Want to learn more about this question?
Virtual DiabetesEd Training Conference – Join us Live on April 17th – 19th 2024 at 11:30 AM PST
Join Coach Beverly and Team for two and a half days of knowledge-sharing, fun, and “aha” moments for our Virtual DiabetesEd Training Conference April 17th – 19th, 2024.
Attendees will leave this conference with new tools and a refreshed understanding of the latest advances in person-centered diabetes care. Our team highlights the ADA Standards of Care, medications, behavior change, technology, medical nutrition therapy, and more!
Our instructors co-teach the content to keep things fresh and lively.
Friend Discount: 3 or more only $449 per person. Email us at [email protected] with the name and email of each registrant to get the discount!
Program Details
- Dates: April 17-19th, 2024
- Registration Fee: $399-$569 (see more about reg. options below)
- Friend Discount: For 3 or more people, each person saves $50 off their registration. Email us at [email protected] with the name and email of each registrant to get the discount!
- CEs: 30+ CEs | 18 units for Virtual Conference plus 10+ Bonus CEs. CEs can be applied toward CDCES’s initial application or renewal.
- Speakers: View Conference Faculty
Registration Options
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and our CPEU courses have received Prior Approval* from the Commission of Dietetic Registration (CDR), Provider DI002. Since our CPEU courses received Prior approval* from the CDR, these CPEU courses satisfy the CE requirements for the CDCES /BC-ADM regardless of your profession!
The use of DES products does not guarantee the successful passage of the certification exam. CBDCE and ADCES do not endorse any preparatory or review materials for the CDCES or BC-ADM exams, except for those published by CBDCE & ADCES.
Rationale of the Week | Bone Fracture Prevention Based on 2024 ADA Standards

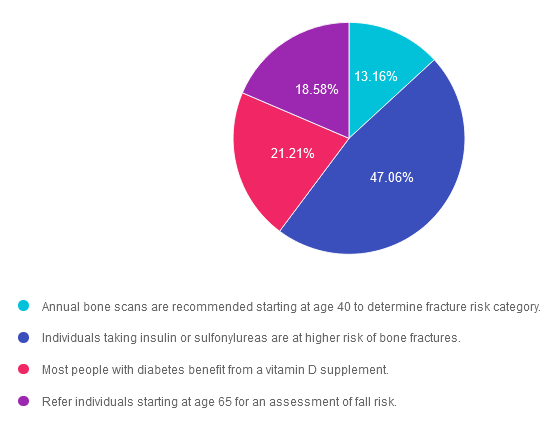
For last week’s practice question, we quizzed participants on bone fracture prevention based on ADA Standards. 47% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question: Since people with diabetes are at increased risk of fractures, the 2024 Standards have an increased focus on preventing bone fractures.
Which of the following is an accurate statement regarding diabetes and bone fractures?
Answer Choices:
- Annual bone scans are recommended starting at age 40 to determine fracture risk category.
- Individuals taking insulin or sulfonylureas are at higher risk of bone fractures.
- Most people with diabetes benefit from a vitamin D supplement.
- Refer individuals starting at age 65 for an assessment of fall risk.
Getting to the Best Answer
If you are thinking about taking the certification exam, this practice test question will set you up for success. Test writers anticipate possible answers based on the details in the question. They will wave those “juicy answers” right under your nose. Your job is to weed through the particulars, pluck out the most important elements and choose the BEST answer.
Answer 1 is incorrect. 13.16% chose this answer. “Annual bone scans are recommended starting at age 40 to determine fracture risk category.” This answer is tempting, but it doesn’t match the ADA Standards that recommend to, “Monitor bone mineral density using dual-energy X-ray absorptiometry of high-risk older adults with diabetes starting at age 65 and younger individuals with diabetes and multiple risk factors every 2–3 years.”
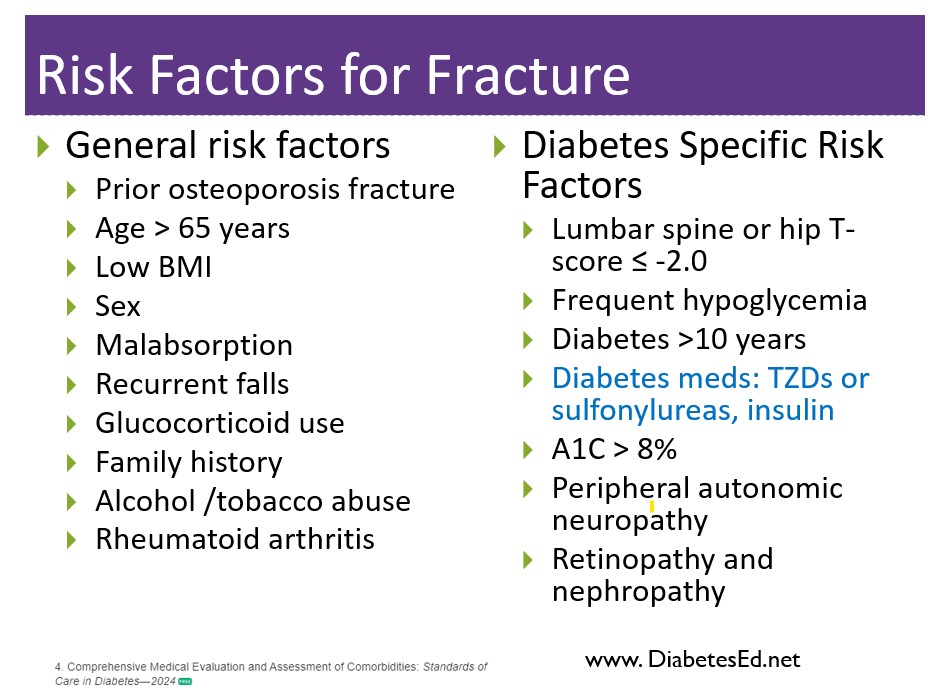
Answer 2 is correct. 47.06% of you chose this answer. “Individuals taking insulin or sulfonylureas are at higher risk of bone fractures.” Yes, this is the best answer. People taking medications that can cause hypoglycemia are at higher risk of falls. Clinicians need to consider the potential adverse impact on bone health when selecting pharmacological options to lower glucose levels in people with diabetes. Prioritizing medications with a proven safety profile for bones is recommended, particularly for those at elevated risk for fractures.
Answer 3 is incorrect. About 21.21% of respondents chose this. “Most people with diabetes benefit from a vitamin D supplement.” This answer is also tempting, but the ADA Standards of Care does not recommend vitamin therapy for “most people”. Vitamin therapy is based on an individual assessment of potential benefit.
Finally, Answer 4 is incorrect. 18.58% chose this answer. “Refer individuals starting at age 65 for an assessment of fall risk.” This answer is tempting, but the ADA recommends we individualize our approach and consider risk of falls and fractures on a ongoing basis. “Fracture risk should be assessed in older adults with diabetes as a part of routine care in diabetes clinical practice, according to risk factors and comorbidities”
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Learn more about Bone Fracture Prevention and ADA Standards
Virtual DiabetesEd Training Conference – Join us Live on April 17th – 19th 2024 at 11:30 AM PST
Join Coach Beverly and Team for two and a half days of knowledge-sharing, fun, and “aha” moments for our Virtual DiabetesEd Training Conference April 17th – 19th, 2024.
Attendees will leave this conference with new tools and a refreshed understanding of the latest advances in person-centered diabetes care. Our team highlights the ADA Standards of Care, medications, behavior change, technology, medical nutrition therapy, and more!
Our instructors co-teach the content to keep things fresh and lively.
Friend Discount: 3 or more only $449 per person. Email us at [email protected] with the name and email of each registrant to get the discount!
Program Details
- Dates: April 17-19th, 2024
- Registration Fee: $399-$569 (see more about reg. options below)
- Friend Discount: For 3 or more people, each person saves $50 off their registration. Email us at [email protected] with the name and email of each registrant to get the discount!
- CEs: 30+ CEs | 18 units for Virtual Conference plus 10+ Bonus CEs. CEs can be applied toward CDCES’s initial application or renewal.
- Speakers: View Conference Faculty
Registration Options
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and our CPEU courses have received Prior Approval* from the Commission of Dietetic Registration (CDR), Provider DI002. Since our CPEU courses received Prior approval* from the CDR, these CPEU courses satisfy the CE requirements for the CDCES /BC-ADM regardless of your profession!
The use of DES products does not guarantee the successful passage of the certification exam. CBDCE and ADCES do not endorse any preparatory or review materials for the CDCES or BC-ADM exams, except for those published by CBDCE & ADCES.
Question of the Week | RS Doesn’t Want to Get Weighed
RS arrives at their quarterly diabetes provider appointment and the medical assistant walks them to the scale, in the clinic hallway, to get their weight. RS politely explains that they feel uncomfortable being weighed but they are happy to share their stated weight. The medical assistant once again encourages RS to get on the scale and reassures RS that they don’t need to look at or know their weight. RS sighs, takes off their shoes and reluctantly gets on the scale to be weighed.
Which of the following best describes the end result of this situation?
- The medical assistant used a person-centered approach to respect the wishes of RS.
- RS exhibited non-adherence and reconsidered their request.
- According to the transtheoretical model, RS was in preparation stage and needed gentle encouragement.
- The clinic staff would benefit from an inservice on providing weight inclusive care.
Click Here to Test your Knowledge
Virtual DiabetesEd Training Conference – Join us Live on April 17th – 19th 2024 at 11:30 AM PST
Join Coach Beverly and Team for two and a half days of knowledge-sharing, fun, and “aha” moments for our Virtual DiabetesEd Training Conference April 17th – 19th, 2024.
Attendees will leave this conference with new tools and a refreshed understanding of the latest advances in person-centered diabetes care. Our team highlights the ADA Standards of Care, medications, behavior change, technology, medical nutrition therapy, and more!
Our instructors co-teach the content to keep things fresh and lively.
Friend Discount: 3 or more only $449 per person. Email us at [email protected] with the name and email of each registrant to get the discount!
Program Details
- Dates: April 17-19th, 2024
- Registration Fee: $399-$569 (see more about reg. options below)
- Friend Discount: For 3 or more people, each person saves $50 off their registration. Email us at [email protected] with the name and email of each registrant to get the discount!
- CEs: 30+ CEs | 18 units for Virtual Conference plus 10+ Bonus CEs. CEs can be applied toward CDCES’s initial application or renewal.
- Speakers: View Conference Faculty
- Dates: April 17-19th, 2024
- Registration Fee: $399-$569 (see more about reg. options below)
- Friend Discount: For 3 or more people, each person saves $50 off their registration. Email us at [email protected] with the name and email of each registrant to get the discount!
- CEs: 30+ CEs | 18 units for Virtual Conference plus 10+ Bonus CEs. CEs can be applied toward CDCES’s initial application or renewal.
- Speakers: View Conference Faculty
Registration Options
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and our CPEU courses have received Prior Approval* from the Commission of Dietetic Registration (CDR), Provider DI002. Since our CPEU courses received Prior approval* from the CDR, these CPEU courses satisfy the CE requirements for the CDCES /BC-ADM regardless of your profession!
The use of DES products does not guarantee the successful passage of the certification exam. CBDCE and ADCES do not endorse any preparatory or review materials for the CDCES or BC-ADM exams, except for those published by CBDCE & ADCES.