Ready to get certified?
Free CDCES Coach App

Subscribe
eNewsletter
Lifestyle and Nutrition Strategies Across CKM Syndrome Stages




Faculty Bios & Disclosures
Our expert team transforms complex diabetes science into clear, practical insights—keeping it real, engaging, and fun!
Program Faculty Disclosures:
Partners for Advancing Clinical Education (Partners) requires every individual in a position to control educational content to disclose all financial relationships with ineligible companies that have occurred within the past 24 months. Ineligible companies are organizations whose primary business is producing, marketing, selling, re-selling, or distributing healthcare products used by or on patients.
All relevant financial relationships for anyone with the ability to control the content of this educational activity are listed below and have been mitigated according to Partners policies. Others involved in the planning of this activity have no relevant financial relationships.
Faculy Bios & Disclosures:
 Coach Beverly Thomassian RN, MPH, CDCES, BC-ADM – CEO of DiabetesEd Services
Coach Beverly Thomassian RN, MPH, CDCES, BC-ADM – CEO of DiabetesEd ServicesDisclosures:
Beverly Thomassian has no financial disclosures
Bio:
 Diana Isaacs, PharmD, BCPS, BCACP, CDCES, BC-ADM, FADCES, FCCPCES
Diana Isaacs, PharmD, BCPS, BCACP, CDCES, BC-ADM, FADCES, FCCPCES
Disclosures:
Dr. Diana Isaacs has the following relevant financial relationships:
- Consultant, advisor, and speaker for Abbot Labratories, Dexcom, Medtronic, Insulet, Lilly, Cequr, Sanofi, and Undermyfork
- Board member at Association for Diabetes Care and Education Specialists
Bio:
Diana Isaacs was awarded 2020 ADCES Diabetes Educator of the Year for her educational platform promoting the use of CGM for people with diabetes and other innovations. She serves in leadership roles for several pharmacies and diabetes organizations. She has numerous diabetes publications and research projects with a focus on medications, CGM and diabetes technology.
Expanded Accreditation
Activity Start and End Date: 10/22/25 – 10/23/2025
Estimated time to complete the activity: 15 hours and 30 minutes
_____________________________________
Jointly provided by Partners for Advancing Clinical Education and Diabetes Education Services
![]()
![]()
Joint Accreditation Statement:
![]() In support of improving patient care, this activity has been planned and implemented by Partners for Advancing Clinical Education (Partners) and Diabetes Education Services. Partners is jointly accredited by the Accreditation Council for Continuing Medical Education (ACCME), the Accreditation Council for Pharmacy Education (ACPE), and the American Nurses Credentialing Center (ANCC), to provide continuing education for the healthcare team.
In support of improving patient care, this activity has been planned and implemented by Partners for Advancing Clinical Education (Partners) and Diabetes Education Services. Partners is jointly accredited by the Accreditation Council for Continuing Medical Education (ACCME), the Accreditation Council for Pharmacy Education (ACPE), and the American Nurses Credentialing Center (ANCC), to provide continuing education for the healthcare team.
Physician Continuing Education:
Partners designates this enduring material for a maximum of 15.50 AMA PRA Category 1 Credit(s)™. Physicians should claim only the credit commensurate with the extent of their participation in the activity.
Nursing Continuing Professional Development:
The maximum number of hours awarded for this Nursing Continuing Professional Development activity is 15.50 contact hours.
Pharmacy Continuing Education:
Partners designates this continuing education activity for 15.50 contact hour(s) (1.550 CEUs) of the Accreditation Council for Pharmacy Education.
(Universal Activity Number – JA4008073-9999-25-206-L01-P)
Type of Activity: Application
For Pharmacists: Upon successfully completing the activity evaluation form, transcript information will be sent to the NABP CPE Monitor Service within 4 weeks.
Dietitian Continuing Education:
This program offers 15.50 CPEUs for dietitians.
Interprofessional Continuing Education:
![]() This activity was planned by and for the healthcare team, and learners will receive 15.50 Interprofessional Continuing Education (IPCE) credit for learning and change.
This activity was planned by and for the healthcare team, and learners will receive 15.50 Interprofessional Continuing Education (IPCE) credit for learning and change.
For additional information about the accreditation of this activity, please visit https://partnersed.com.
Question of the Week | Managing Overnight Hypoglycemia: Best Plan?



Faculty Bios & Disclosures
Program Faculty Disclosures:
Partners for Advancing Clinical Education (Partners) requires every individual in a position to control educational content to disclose all financial relationships with ineligible companies that have occurred within the past 24 months. Ineligible companies are organizations whose primary business is producing, marketing, selling, re-selling, or distributing healthcare products used by or on patients.
All relevant financial relationships for anyone with the ability to control the content of this educational activity are listed below and have been mitigated according to Partners policies. Others involved in the planning of this activity have no relevant financial relationships.
Faculy Bios & Disclosures:
Lawrence Fisher, Ph.D., ABPP, Professor Emeritus, UCSF
- Consultant, advisor, and speaker for Eli Lilly
Speaker Interview:
Bio:
Dr. Fisher has been a professor in the Department of Family & Community Medicine at the University of California, San Francisco for over 25 years, and he is the Director of The Behavioral Diabetes Research Group at UCSF.
He has a Diplomate in Clinical Psychology from the American Board of Professional Psychology and is a former Associate Editor of Diabetes Care. He has conducted multiple cross-sectional and longitudinal NIH- and ADA-supported clinical research with adults with diabetes and their families.
His recent work focuses on diabetes distress and depression, disease management, and how adults and families struggle over time to manage chronic health conditions. He has won two major UCSF School of Medicine teaching awards, was nominated for the UCSF Postdoctoral Scholars Association Outstanding Mentorship Award, and has received a certificate from the American Psychological Association in “Recognition for Substantial Contributions to the Field of Family Psychology and Health.”
In 2012 he received the Richard Rubin Award from the American Diabetes Association. He maintains an active clinical practice at UCSF, has published over 190 peer-reviewed articles on diabetes and related topics, and frequently speaks to both professional and lay groups at local, national, and international meetings and workshops.
 Susan Guzman, PhD
Susan Guzman, PhD
- Consultant, advisor, and speaker for Abbot Labratories and Embecta
Dr. Guzman is a clinical psychologist specializing in diabetes. In 2003, Dr. Guzman co-founded the Behavioral Diabetes Institute (BDI), the first non-profit organization devoted to the emotional and behavioral aspects of living with diabetes.
At BDI, she serves as the Director of Clinical Education, developing and leading programs for people with diabetes and healthcare professionals. She has helped develop and facilitate diabetes distress group interventions for two NIH-funded research studies for adults with type 1 diabetes.
Dr. Guzman is passionate about helping to change the conversations in diabetes away from shame, blame, and judgment to those based on facts, empathy, and engagement. She has been part of a joint ADA/ADCES effort to address problematic language and messages in diabetes.
Coach Beverly Thomassian RN, MPH, CDCES, BC-ADMBeverly Thomassian has no financial disclosures
Speaker Interview:
Bio:
Expanded Accreditation
Activity Start and End Date: 7/15/2025 to 7/22/2027
Estimated time to complete the activity: 6 hours and 15 minutes
Jointly provided by Partners for Advancing Clinical Education and Diabetes Education Services
![]()
![]()
Joint Accreditation Statement:
![]() In support of improving patient care, this activity has been planned and implemented by Partners for Advancing Clinical Education (Partners) and Diabetes Education Services. Partners is jointly accredited by the Accreditation Council for Continuing Medical Education (ACCME), the Accreditation Council for Pharmacy Education (ACPE), and the American Nurses Credentialing Center (ANCC), to provide continuing education for the healthcare team.
In support of improving patient care, this activity has been planned and implemented by Partners for Advancing Clinical Education (Partners) and Diabetes Education Services. Partners is jointly accredited by the Accreditation Council for Continuing Medical Education (ACCME), the Accreditation Council for Pharmacy Education (ACPE), and the American Nurses Credentialing Center (ANCC), to provide continuing education for the healthcare team.
Physician Continuing Education:
Partners designates this enduring material for a maximum of 6.25 AMA PRA Category 1 Credit(s)™. Physicians should claim only the credit commensurate with the extent of their participation in the activity.
Nursing Continuing Professional Development:
The maximum number of hours awarded for this Nursing Continuing Professional Development activity is 6.25 contact hours.
Pharmacy Continuing Education:
Partners designates this continuing education activity for 6.25 contact hour(s) (.625] CEUs) of the Accreditation Council for Pharmacy Education.
(Universal Activity Number – UAN JA4008073-9999-25-198-H01-P)
Type of Activity: Application
For Pharmacists: Upon successfully completing the activity evaluation form, transcript information will be sent to the NABP CPE Monitor Service within 4 weeks.
Dietitian Continuing Education:
This program offers 6.25 CPEUs for dietitians.
Interprofessional Continuing Education:
![]() This activity was planned by and for the healthcare team, and learners will receive 6.25 Interprofessional Continuing Education (IPCE) credit for learning and change.
This activity was planned by and for the healthcare team, and learners will receive 6.25 Interprofessional Continuing Education (IPCE) credit for learning and change.
Disclosure of Unlabeled Use:
This educational activity may contain discussion of published and/or investigational uses of agents that are not indicated by the FDA. The planners of this activity do not recommend the use of any agent outside of the labeled indications. The opinions expressed in the educational activity are those of the faculty and do not necessarily represent the views of the planners. Please refer to the official prescribing information for each product for discussion of approved indications, contraindications, and warnings.
Disclaimer:
Participants have an implied responsibility to use the newly acquired information to enhance patient outcomes and their own professional development. The information presented in this activity is not meant to serve as a guideline for patient management. Any procedures, medications, or other courses of diagnosis or treatment discussed or suggested in this activity should not be used by clinicians without evaluation of their patient’s conditions and possible contraindications and/or dangers in use, review of any applicable manufacturer’s product information, and comparison with recommendations of other authorities.
Instructions for Credit
Participation in this self-study activity should be completed in approximately 6 hours and 15 minutes. To successfully complete this activity and receive CE credit, learners must follow these steps during the period from 7/15/2025 to 7/22/2027.
- Review the objectives and disclosures
- Study the educational content in Online University
- After review of content, a module within the course in the Online University will list a link to Partners for Advancing Clinical Education’s website
- Visit Partners for Advancing Clinical Education website listed in course in the Online University
- Complete the activity evaluation through Partners for Advancing Clinical Education website
For additional information about the accreditation of this activity, please visit https://partnersed.com.
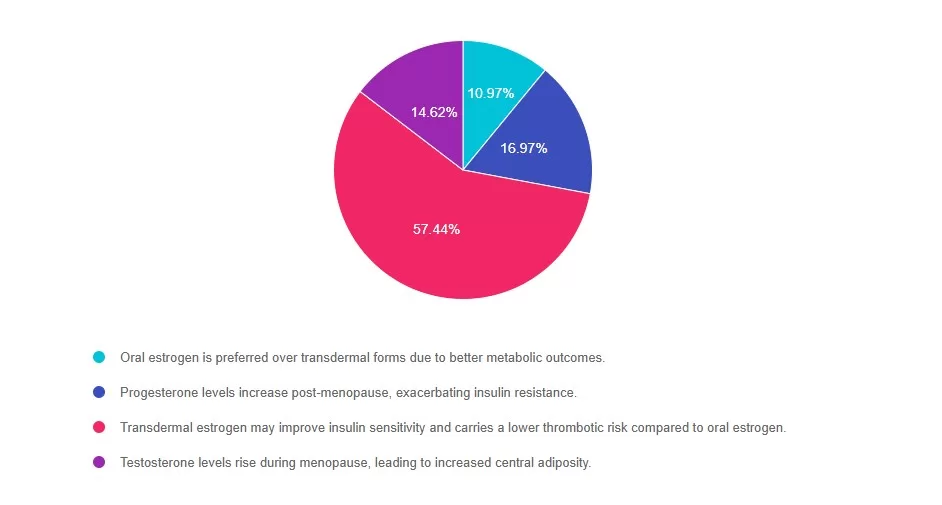
Rationale of the Week | Current Hormone Therapy Guidance in T2D

Beyond Blood Glucose: Empowering Health Through a Holistic Lens

Question of the Week | Diabetes Burnout Despite BG in Target?

Gut to the Butt Webinar – Join for FREE & Earn CE | June 25th

Save the Date for an Advancements in Diabetes Webinar
From the Gut to the Butt – Exploring the GI System
Wednesday, June 25, 2025 3 pm Eastern
(2 pm Central | 1 pm Mountain | 12 pm Pacific | 11 am Alaska)
This session offers 1 hour of CME/CE/CPEU/CPE
 Presented by:
Presented by:
Beverly Thomassian, RN, MPH, CDCES, BC-ADM
President, Diabetes Education Services
Diabetes Nurse Specialist, Colusa Indian Health
Information about the webinar presentation:
This webinar is designed to encourage health care professionals to explore digestive co-conditions
associated with diabetes and take actions to prevent and address disorders of the GI system.
Participants will gain a more in-depth understanding of the interrelationship between glucose levels,
insulin resistance and the role of the liver, pancreas, and intestinal tract in overall health.
Join at:
Link: https://hhs-ihs.webex.com/hhs-ihs/j.php?MTID=m9eb2bbefe1c03867eefeb4634b5c3b7f
Webinar Number & Access Code: 2825 648 4919
Webinar Password: qPZt6bGCu77 (77986242 when dialing from a phone or video system)
Join by Phone: 1-415-527-5035
Download Information Flyer Here
Notes:
• Advancements in Diabetes webinars use the Webex platform; if you have difficulty joining, please visit Webex help.
• If joining from a browser, please use Microsoft Edge or Google Chrome.
• Be sure to join the session about 5 minutes before the start time.
• Registration is not required.
• There is no cost for participation in the webinar.
For additional information, please contact the Division of Diabetes at [email protected].
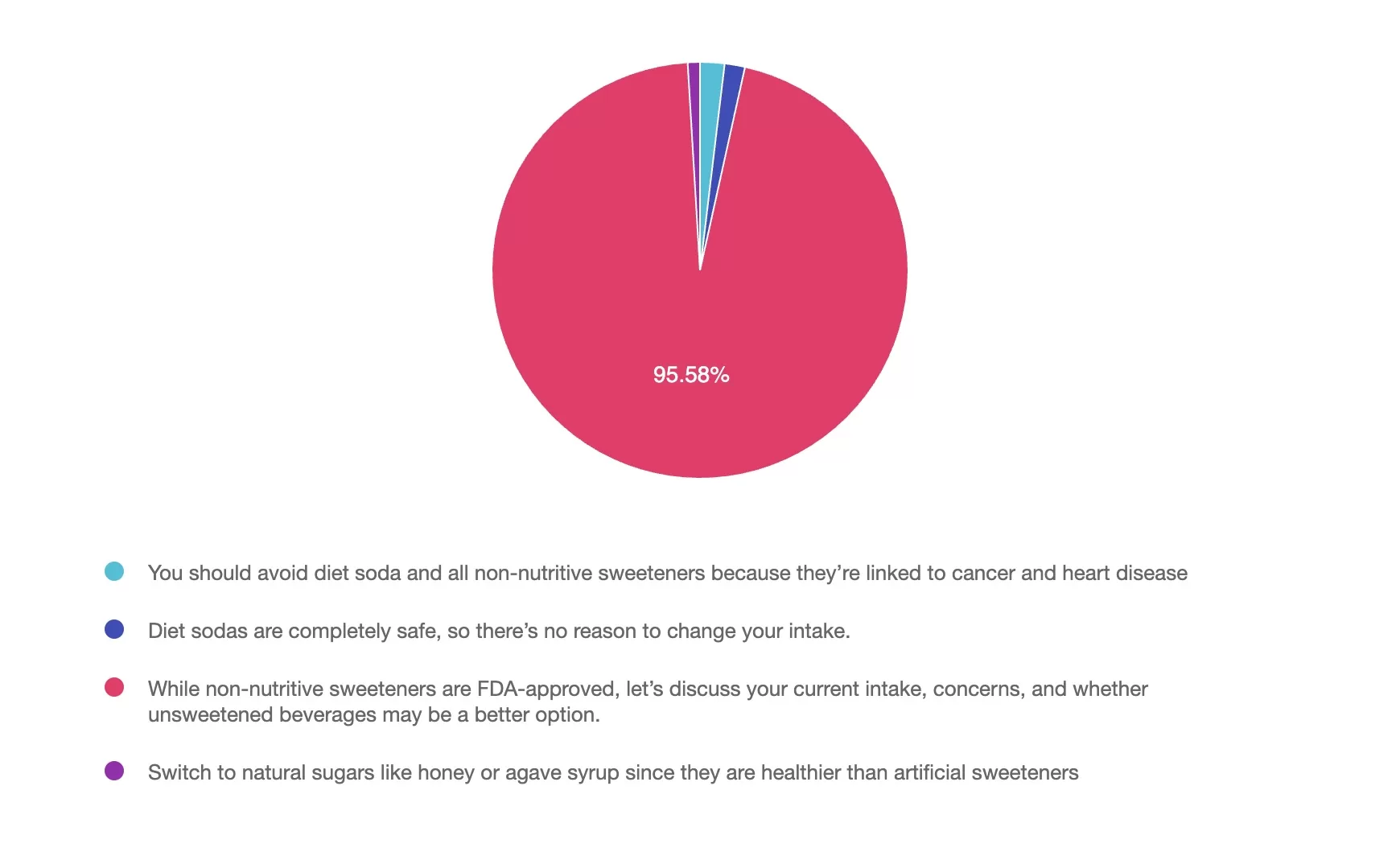
Rationale of the Week | T1D and Artificial Sweeteners: Safe Limits
How Landing in the Wrong Place Can Help You Find Your Way