
Subscribe
eNewsletter
Ready to get certified?
Free CDCES Coach App
eNewsletter
Free CDCES Coach App
JR is 67 with type 1 diabetes and was discharged a few months ago after receiving a coronary artery bypass. JR is on insulin pump therapy and a CGM, with a recent A1C of 6.7%. Their blood pressure is 129/78.
Other recent labs include:
JR’s medications include: insulin, atorvastatin 80mg, atenolol 50mg, and aspirin therapy. JR has met with the dietitian and is trying to eat healthfully. They have lost 5 pounds over the past few months.
Based on the 2023 ADA Standards of Care and JR’s history, which of the following is considered best practice?
Click Here to Test your Knowledge
Our annual Valentine’s sale is our way of thanking you, our dedicated community of diabetes health care professionals and advocates, for your service and love.
To celebrate, we are spreading the love with a 15% discount off
ALL Online Courses & Virtual Conference from Feb 10-17, 2023. Use code LOVE15 at checkout.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.

For last week’s practice question, we quizzed participants on the best action for a safe surgery. 51% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question:
PZ is having elective surgery in the morning. Diabetes medications include 20 units glargine (Semglee) at hs, metformin BID and empagliflozin (Jardiance).
According to 2023 ADA Standards, what are the best actions for a safe surgery?
Answer Choices:
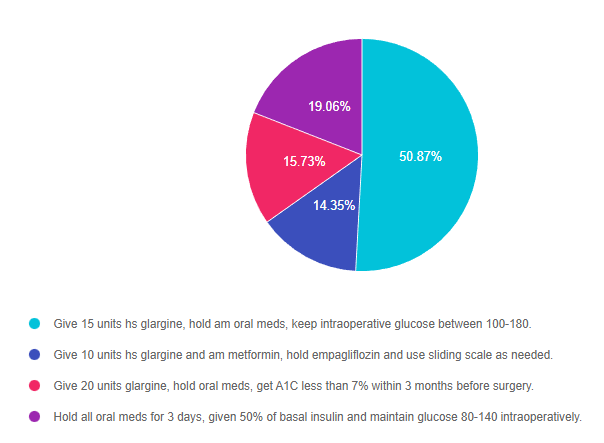
Answer 1 is correct. 50.87% chose this answer, “Give 15 units hs glargine, hold am oral meds, keep intraoperative glucose between 100-180.” YES, GREAT JOB! The ADA Standard 16 on Hospitalization has been updated with new perioperative glucose goals and preop medication adjustments. To prevent intraoperative hypoglycemia, the glucose goal was increased to 100-180. In addition, they recommend reducing basal insulin by 20-25% the night before surgery and holding all oral meds the morning of surgery. SGLT-2s are held for 3-4 days before surgery to decrease risk of DKA in the perioperative period. In this vignette, we reduced PZ’s basal insulin from 20 units to 15 units (25% decrease) and held all oral meds the morning of surgery. In addition, the 2023 Standards recommend achieving an A1C less than 8% before elective surgeries. Since about 20% of people undergoing surgery have diabetes, these guidelines are super helpful and important to improve post surgical outcomes.
Answer 2 is incorrect. 14.35% of you chose this answer, “Give 10 units hs glargine and am metformin, hold empagliflozin and use sliding scale as needed.” This is answer is close and partly correct, because it recommends holding the oral medications. However, the first part of the answer is incorrect since a basal insulin reduction of 50% is too aggressive. People release lots of counterregulatory hormones during surgery, so they still need at least 75% of their usual basal insulin dose to prevent intraoperative hyperglycemia. If the person uses NPH basal insulin, they would need to reduce the evening dose by 50%. Since about 20% of people undergoing surgery have diabetes, these guidelines are super helpful and important to improve post surgical outcomes.
Answer 3 is incorrect. 15.73% of respondents chose this answer, “Give 20 units glargine, hold oral meds, get A1C less than 7% within 3 months before surgery.” This is answer is close and partly correct, because it recommends holding the oral medications. However, the first part of the answer is incorrect since the basal insulin needs to be reduced by 20-25% to prevent intraoperative hypoglycemia. In addition, the 2023 Standards recommend achieving an A1C less than 8% (not 7%) before elective surgeries. Since about 20% of people undergoing surgery have diabetes, these guidelines are super helpful and important to improve post surgical outcomes.
Finally, Answer 4 is incorrect. 19.06% chose this answer, “Hold all oral meds for 3 days, given 50% of basal insulin and maintain glucose 80-140 intraoperatively.” This entire answer is incorrect for the following reasons. Oral meds are held the day of surgery, except for SGLT2i’s, which are held for 3-4 days pre-op. As far as basal insulin, the ADA guidelines recommend giving 75-80% of usual dose, except for NPH insulin, which is reduced by 50%. Lastly, the intraoperative glucose target is 100 -180. Since about 20% of people undergoing surgery have diabetes, these guidelines are super helpful and important to improve post surgical outcomes.
Thank you so much for reading this “Rationale of the Week”.
We invite you to join Coach Beverly on May 30, 2023 – Hospital and Hyperglycemia 1.5 CEs
This course, updated annually, is an essential review for anyone in the field of diabetes. Join Coach Beverly as she summarizes the 2023 updates to the American Diabetes Association’s Standards of Medical Care in Diabetes and provides critical teaching points and content for healthcare professionals involved in diabetes care and education.
Objectives:
Intended Audience: This course is a knowledge-based activity designed for individuals or groups of diabetes professionals, including RNs, RDs, Pharmacists, Nurse Practitioners, Clinical Nurse Specialists, Physician Assistants, and other health care providers interested in staying up to date on current practices of care for people with prediabetes, diabetes, and other related conditions.
Don’t worry if you can’t make it live. Your registration guarantees access to the recorded version in the Online University.
All hours earned count toward your CDCES Accreditation Information

Can’t join all the sessions live? No problem. Your registration guarantees you access to the recorded lectures for a full year.
This bundle is specifically designed for healthcare professionals who are studying for the Board Certified in Advanced Diabetes Management (BC-ADM) or the Certified Diabetes Care and Education Specialist (CDCES) certification exam.
Intended Audience: This library of critical information is designed for individuals or groups of diabetes specialists, including RNs, RDs, Pharmacists, Nurse Practitioners, Clinical Nurse Specialists, Physician Assistants, and other health care providers interested in staying up to date on current practices of care for people with diabetes and preparing for the BC-ADM or the CDCES certification Exam.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
Starting in 2023, the Inflation Reduction Act, limits insulin out-of-pocket costs at $35 for a month for each insulin product covered by an individual’s Medicare Part D prescription drug plan or Medicare Advantage plan.

Under a Medicare Part D prescription drug plan, if insulin is a covered insulin product, the $35 cap for a month’s supply for each insulin product applies, beginning on January 1, 2023.
A covered insulin product is one that is included in a Part D sponsor’s formulary.
This includes any new insulin products that become available during the plan year. An insulin product might also be considered covered in other instances and there can be changes in covered products during the year.
In addition, under Medicare Part B, if insulin is delivered through a traditional pump that is covered under the durable medical equipment benefit, the cost-sharing amount for a person with Medicare is capped at $35 for a month’s supply of insulin beginning July 1, 2023.
The cap applies only to insulin products on a plan’s formulary, or the list of covered medications.
Unfortunately, most drug plans don’t cover the more than 70 insulin products on the market. And some plans actually charge less than $35 a month for particular products, but those lower copays are difficult to ferret out on the Medicare Plan Finder. Adding to the complexity of making a choice of plans, many people with diabetes use several prescription drugs besides insulin.
End result: Finding the lowest-cost, most effective plan that covers all of a participant’s medicines among the 20 or more plans that might be offered in someone’s zip code can be complicated, at least for 2023.

Strategies to succeed? Medicare officials and the local offices that support beneficiaries strongly recommend getting help. “People with Medicare who take insulin are encouraged to call 1-800-MEDICARE or to contact their State Health Insurance Assistance Programs (SHIP) for help comparing coverage and costs this year,” Meena Seshamani, M.D., director of CMS’s Center for Medicare, said in an emailed statement. This is just a one-year glitch, the Centers for Medicare & Medicaid Services says, so it’s best handled by those with practice navigating the Plan.
Experts suggest Medicare recipients make a list of all their prescriptions, including the dosages and how often they are refilled. Then go to Medicare.gov and create an account — it allows individuals to store their drug list securely, which can speed up the task of finding a plan.
Then they have two choices:
The best bet is to call the state agency to find the county or other local office and contact a trained counselor who can analyze plan options. SHIPs objective is to provide comprehensive, unbiased information on Medicare. The counselor will make sure, for example, that any Medicare Advantage plan you consider actually covers the insulin products you need.
Don’t worry if you can’t make our webinars live. Your registration guarantees access to the recorded version in the Online University.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
JL is 19 and has type 1 diabetes, drinks a “few beers” on the weekends with their college friends. JL uses an insulin pump, but mostly relies of fingerstick checks to monitor blood sugars. According to their log, JL experienced a few low blood glucose levels the past weekend of 62, 49 and 51.
Based on the ADA Standards, what is the most important recommendation for JL?
Click Here to Test your Knowledge
Can’t join all the sessions live? No problem. Your registration guarantees you access to the recorded lectures for a full year.
This bundle is specifically designed for healthcare professionals who are studying for the Board Certified in Advanced Diabetes Management (BC-ADM) or the Certified Diabetes Care and Education Specialist (CDCES) certification exam.
Intended Audience: This library of critical information is designed for individuals or groups of diabetes specialists, including RNs, RDs, Pharmacists, Nurse Practitioners, Clinical Nurse Specialists, Physician Assistants, and other health care providers interested in staying up to date on current practices of care for people with diabetes and preparing for the BC-ADM or the CDCES certification Exam.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
For last week’s practice question, we quizzed participants on Diabetes and NASH. 41% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question:
The provider referred RT, a 72-year-old with type 2 diabetes and non-alcoholic fatty steatohepatitis (NASH), for an appointment with the diabetes care and education specialist. RT is frightened because their brother died of liver cancer.
Which of the following is the most accurate statement regarding NASH and diabetes?
Answer Choices:
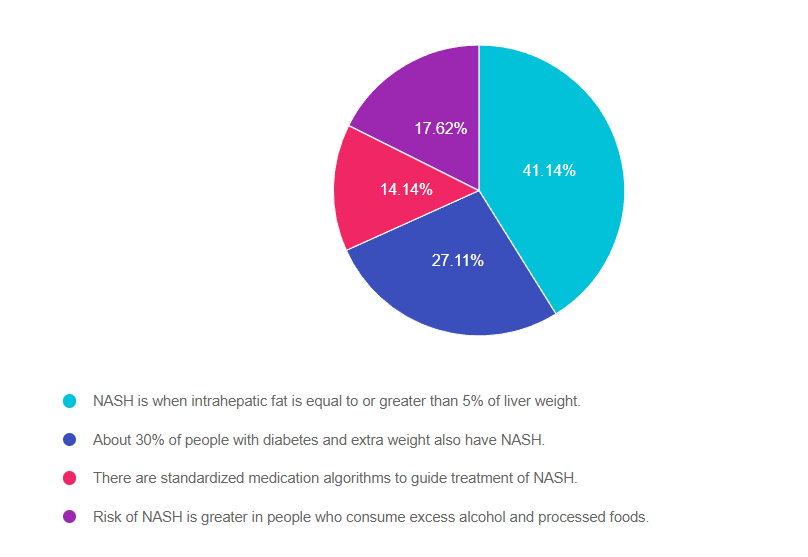
Answer 1 is correct. 41.14% chose this answer, “NASH is when intrahepatic fat is equal to or greater than 5% of liver weight.” GREAT JOB! According to ADA Standard 4, “NASH is defined histologically as having more than 5% hepatic steatosis and associated with inflammation and hepatocyte injury (hepatocyte ballooning), with or without evidence of liver fibrosis”.
Answer 2 is incorrect. 27.11% of you chose this answer, “About 30% of people with diabetes and extra weight also have NASH.” This is a juicy answer, but it is an underestimate of the current problem. Recent studies in adults in the U.S. estimate that more than 70% of people with type 2 diabetes have non alcoholic fatty liver disease (NAFLD). The more serious, steatohepatitis, is estimated to affect more than 50% of people with type 2 diabetes with NAFLD and it appears to be a driver for the development of fibrosis.
Answer 3 is incorrect. 14.14% of respondents chose this answer, “There are standardized medication algorithms to guide the treatment of NASH.” According to ADA Standard 4, at present, there are no FDA-approved drugs for the treatment of NASH. Therefore, treatment for people with type 2 diabetes and NASH is centered on the dual purpose of treating hyperglycemia and weight loss. Pioglitazone and some glucagon-like peptide 1 receptor agonists (GLP-1 RAs) have been shown to be effective to treat steatohepatitis, may slow fibrosis progression, and decrease cardiovascular disease.
Finally, Answer 4 is incorrect. 17.62% chose this answer, “Risk of NASH is greater in people who consume excess alcohol and processed foods.” Nonalcoholic steatohepatitis [NASH] indicates liver inflammation in the absence of ongoing or recent consumption of significant amounts of alcohol (defined as ingestion of >21 standard drinks per week in men and >14 standard drinks per week in women over a 2-year period preceding evaluation) or the presence of other secondary causes of fatty liver disease. NASH is not a result of excess alcohol intake and is usually associated with genetics, body weight and insulin resistance.
Thank you so much for reading this “Rationale of the Week”.
We also invite you to join our Online Courses for more information (see info below)
Hope you can join our Diabetes Boot Camp in February and our other Level 2 Courses.
Can’t join all the sessions live? No problem. Your registration guarantees you access to the recorded lectures for a full year.
This bundle is specifically designed for healthcare professionals who are studying for the Board Certified in Advanced Diabetes Management (BC-ADM) or the Certified Diabetes Care and Education Specialist (CDCES) certification exam.
Intended Audience: This library of critical information is designed for individuals or groups of diabetes specialists, including RNs, RDs, Pharmacists, Nurse Practitioners, Clinical Nurse Specialists, Physician Assistants, and other health care providers interested in staying up to date on current practices of care for people with diabetes and preparing for the BC-ADM or the CDCES certification Exam.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
February is the month we celebrate love.
In my opinion, love is at the center of providing diabetes care and education. We open our hearts as we carefully listen to people share their stories about living with diabetes. We celebrate successes and grieve losses alongside the individuals we serve every day. We speak our hearts when we advocate for evidence-based care that enhances well-being and improves outcomes.
In celebration of the compassionate contributions of diabetes care and education specialists, we are excited to announce our “Spreading the Love” Sale during the week of Valentine’s Day.
This month, we are delighted to share our updated Diabetes Education Services logos, celebrating 25 years of growth, connection, and inspiration. Keep your eyes open for website and online communications that include our freshened-up logo coupled with a 25.
For this month’s newsletter, we highlight the new Medicare $35 Insulin cap, discuss how treatments to delay type 1 diabetes might lead to childhood screening, announce a new SGLT-2i and of course test your knowledge with our Question and Rationale of the Week.
Lastly, we are offering two “Making a Difference” Scholarships, which provide a pair of deserving recipients with free registration for our Virtual DiabetesEd Training Course in late April.
It has been a complete joy to serve our community and provide meaningful courses, newsletters, blogs, cheat sheets, and content that makes a real difference in people’s lives since 1998. Who knows what we will come up with in the next 25 years?
With gratitude for our amazing community,
Coach Beverly and Bryanna
Featured Articles
Upcoming Webinars

Whether you are new to diabetes or a seasoned expert, you’ll benefit from this virtual conference with the latest research plus critical content that you can immediately apply to your clinical practice.
If you are seeking a state-of-the-art review of current diabetes care, this course is for you. Our team has been fine-tuning this course for over fifteen years, and we know what you need. This program can also be a great addition to your CDCES or BC-ADM exam study plan.
Group discounts are available!*
Download Course Flyer | Download Schedule
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
PZ is having elective surgery in the morning. Diabetes medications include 20 units glargine (Semglee) at hs, metformin BID and empagliflozin (Jardiance).
According to 2023 ADA Standards, what are the best actions for a safe surgery?
Click Here to Test your Knowledge
This course, updated annually, is an essential review for anyone in the field of diabetes. Join Coach Beverly as she summarizes the 2023 updates to the American Diabetes Association’s Standards of Medical Care in Diabetes and provides critical teaching points and content for healthcare professionals involved in diabetes care and education.
Objectives:
Intended Audience: This course is a knowledge-based activity designed for individuals or groups of diabetes professionals, including RNs, RDs, Pharmacists, Nurse Practitioners, Clinical Nurse Specialists, Physician Assistants, and other health care providers interested in staying up to date on current practices of care for people with prediabetes, diabetes, and other related conditions.
Don’t worry if you can’t make it live. Your registration guarantees access to the recorded version in the Online University.
All hours earned count toward your CDCES Accreditation Information
Can’t join all the sessions live? No problem. Your registration guarantees you access to the recorded lectures for a full year.
This bundle is specifically designed for healthcare professionals who are studying for the Board Certified in Advanced Diabetes Management (BC-ADM) or the Certified Diabetes Care and Education Specialist (CDCES) certification exam.
Intended Audience: This library of critical information is designed for individuals or groups of diabetes specialists, including RNs, RDs, Pharmacists, Nurse Practitioners, Clinical Nurse Specialists, Physician Assistants, and other health care providers interested in staying up to date on current practices of care for people with diabetes and preparing for the BC-ADM or the CDCES certification Exam.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
This course will transform your test anxiety into calm self-confidence and test-taking readiness.

“Becoming a Certified Diabetes Care and Education Specialist (CDCES) is one of the best professional and personal decisions I have ever made.” – Coach Beverly Thomassian, RN, MPH, CDCES, BC-ADM
Beverly has custom-designed this course bundle to prepare you for your CDCES Exam. This bundle includes our CDCES Online Prep Bundle (featured above) plus the ADCES (formerly AADE) Review Guide – 5th Edition – Revised. This bundle includes Levels 1 through 3 (AKA Boot Camp), toolkits, plus the ADCES Review Guide.
Included in this bundle is:
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.