
Subscribe
eNewsletter
Ready to get certified?
Free CDCES Coach App
eNewsletter
Free CDCES Coach App
Free Med Pocket Cards
For last week’s practice question, we quizzed participants on Gestational Diabetes: Diabetes Care in the Fourth Trimester. 51% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question

MT is a 29-year-old with Type 1 diabetes who is currently 14 weeks pregnant. She uses a continuous glucose monitor (CGM) with concurrent fingersticks and uploads her glucose data weekly. Her CGM settings was already set to the recommended time in
range and the latest CGM report shows the following: time in range (TIR): 67%, time below range: 6%, time above range: 27%.
Based on current ADA Standard of Care, which of the following statements is most accurate regarding her CGM values?
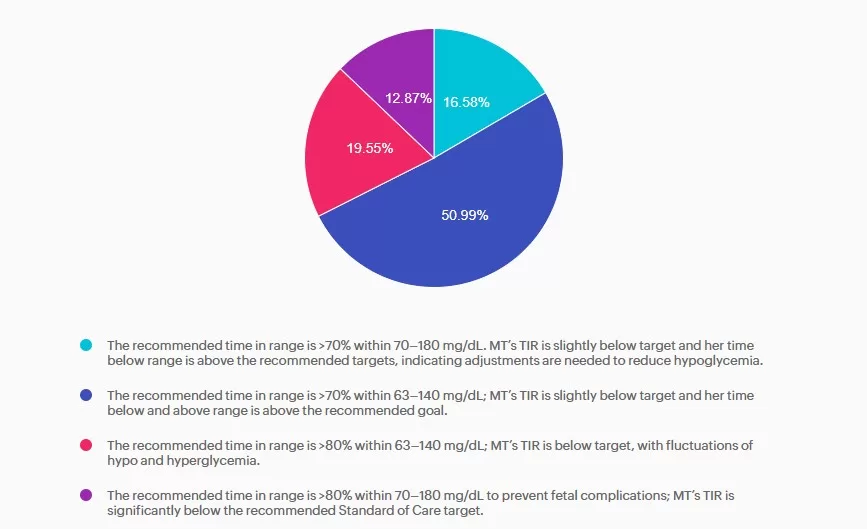
Answer A is incorrect: 16.58% chose this answer, “The recommended time in range is >70% within 70–180 mg/dL. MT’s TIR is slightly below target and her time below range is above the recommended targets, indicating adjustments are needed to reduce hypoglycemia.” Answer A is incorrect. The answer uses non-pregnancy CGM target range of 70–180 mg/dL. Pregnancy target range for individuals with type 1 diabetes are lower, keep reading for the best answer.
Answer B is correct: 51% chose this answer, “The recommended time in range is >70% within 63–140 mg/dL; MT’s TIR is slightly below target and her time below and above range is above the recommended goal.” Answer B is correct. Based on the 2025 ADA Standards of Care the recommended time in range targets for individuals with type 1 diabetes during pregnancy is >70% between 63-140 mg/dL, < 4% under 63 mg/dL with < 1 % under 54 mg/dL, and < 25% over 140 mg/dL.
Answer C is incorrect: 19.55% chose this answer, “The recommended time in range is >80% within 63–140 mg/dL; MT’s TIR is below target, with fluctuations of hypo and hyperglycemia.” Answer C is incorrect. The time in range target is above the evidenced-based
minimum and MT is having frequent hypoglycemia in addition to hyperglycemia, both outside the goal ranges.
Answer D is incorrect: 12.87% chose this answer, “The recommended time in range is >80% within 70–180 mg/dL to prevent fetal
complications; MT’s TIR is significantly below the recommended Standard of Care target.” Answer D is incorrect. The recommended target range for individuals with type 1diabetes during pregnancy is 63-140 mg/dL as stated above.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
with Coach Beverly Thomassian RN, MPH, CDCES, BC-ADM
Course credits through AMA PRA Category 1 Credits™, ACPE, ANCC, and CDR!
This course is included in our Level 2 | Standards of Care Intensive
This Level 2 course fulfills the annual ADA Standards of Care component required for CDCES certification renewal. They also count toward your CDCES and BC-ADM certification CE requirements.
Join Coach Bev for an in-depth exploration of the 2026 ADA Standards! This is our most popular course of the year, offering the perfect opportunity to immerse yourself in the essential content featured in this comprehensive 300-page clinical guidebook.
This course, updated annually, is an essential review for anyone in the field of diabetes. Join Coach Beverly as she summarizes the annual updates to the American Diabetes Association’s (ADA) Standard of Medical Care in Diabetes. This course provides critical teaching points and content for healthcare professionals involved in diabetes care and education.
Topics:
Course Objectives:
Upon completion of this activity, participants will be able to:
For last week’s practice question, we quizzed participants on RT forgetting their insulin, and what would be the best response. 63.10% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
RT has type two diabetes and has been maintaining a time and range of 70% or greater. However, when they show up at the office, the last week’s time in range dropped to 30%. You ask what was different this week from the previous few months. RT tells you they went on a five day fishing trip and forgot their insulin.
What’s the best response?
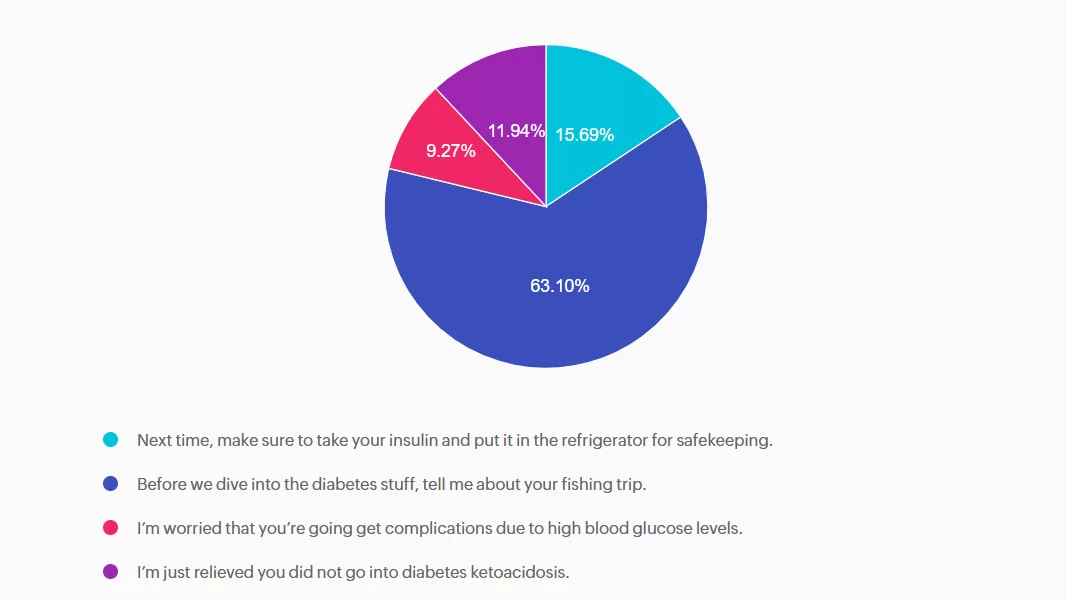
Answer A is incorrect: 15.69% chose this answer, “Next time, make sure to take your insulin and put it in the refrigerator for safekeeping.” This approach goes under the compliance model, where the healthcare professional only provides one way instruction without considering the individuals insights and problem solving skills. We want to work toward a person-centered collaborative approach to foster connection.
Answer B is correct: 63.10% chose this answer, “Before we dive into the diabetes stuff, tell me about your fishing trip.” Great job! This is the best answer. By asking RT about their fishing trip first, you let them know you are interested in their life experiences and this helps to establish a connection. After hearing about the trip, we might pivot and say something like, “Do you want to discuss strategies to bring your insulin on your next fishing trip?”
Answer C is incorrect: 9.27% chose this answer, “I’m worried that you’re going get complications due to high blood glucose levels.” Although this statement shows concern, it is unlikely that RT will get diabetes complications from not taking their insulin for a few days. This statement could lead to feelings of shame and failure, and may close the door to making a meaningful connection.
Answer D is incorrect: 11.94% chose this answer, “I’m just relieved you did not go into diabetes ketoacidosis.” This statement could evoke feelings of guilt and shame, that could close the door to future communication. And if RT has type 2 diabetes, the chance of DKA is minimal. Instead of focusing on the HCP feelings, let’s check in with RT and explore problem solving strategies for future trips that would work for them.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
For last week’s practice question, we quizzed participants on Diabetes Tech and Diabetes Distress. 99.36% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Kyle is a 55-year-old man with type 2 diabetes for ten years. He was recently diagnosed with retinopathy in both eyes. His grandmother lost her eyesight due to diabetes. Due to this family history, he is very concerned about his new diagnosis. He uses a Libre continuous glucose monitor (CGM) to monitor his blood sugar levels. During your visit, he is preoccupied with checking his Libre CGM and tells you that he uses his glucometer to verify CGM readings at least four to six times per day. When you ask him about this, he reports that he can’t focus on his work or home life if he isn’t over 90% time in range.
As a diabetes care and education specialist, what is the best approach to this situation?
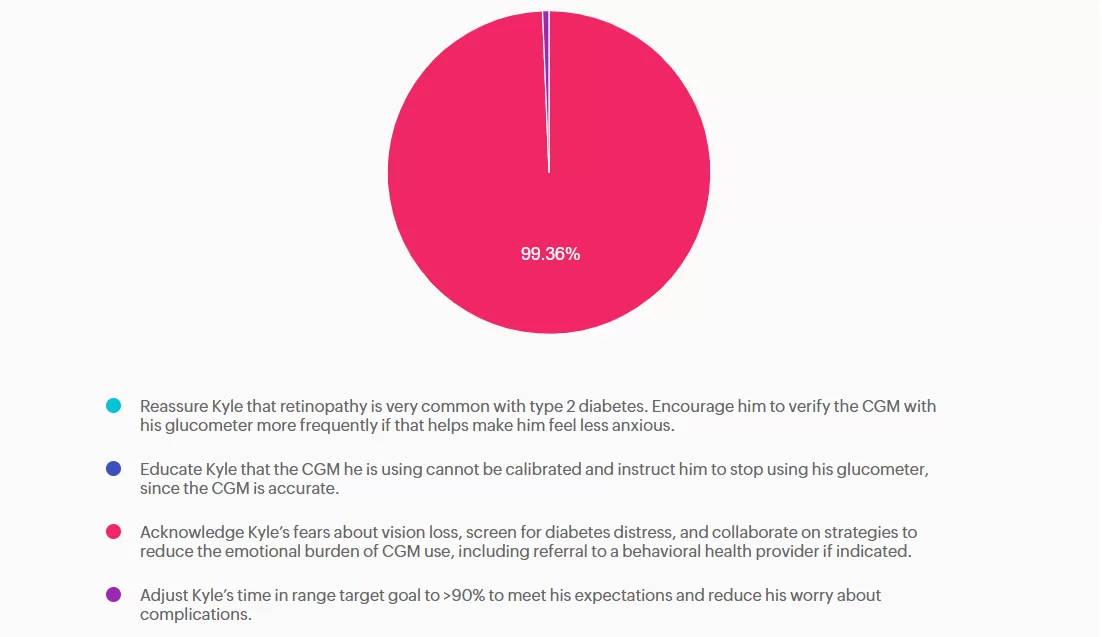
Answer A is incorrect: 0% chose this answer, “Reassure Kyle that retinopathy is very common with type 2 diabetes. Encourage him to verify the CGM with his glucometer more frequently if that helps make him feel less anxious.” This is incorrect. Although diabetes retinopathy is a common complication of diabetes, it is not inevitable, and the risk can be reduced by maintaining optimal glycemic control. Additionally, verifying blood glucose levels with a glucometer when there appears to be no issue with his CGM will not alleviate his anxiety.
Answer B is incorrect: 0% chose this answer, “Educate Kyle that the CGM he is using cannot be calibrated and instruct him to stop using his glucometer, since the CGM is accurate.” This is incorrect. Though his particular CGM cannot be calibrated, fingerstick blood glucose readings are the gold standard when CGM readings are unexpectedly out of range.
Answer C is correct: 99.36% chose this answer, “Acknowledge Kyle’s fears about vision loss, screen for diabetes distress, and collaborate on strategies to reduce the emotional burden of CGM use, including referral to a behavioral health provider if indicated.” This is correct. Kyle is demonstrating symptoms of diabetes distress due to fear of ocular complications, perfectionism, and technology overwhelm. The ADA Standards of Care 2025 recommend routine screening for diabetes distress and other psychosocial concerns at least annually or when complications arise.
Answer D is incorrect: 0.64% chose this answer, “Adjust Kyle’s time in range target goal to >90% to meet his expectations and reduce his worry about complications.” This is incorrect: The time in range goal for most adults living with diabetes is >70%. Adjusting his time-in-range goal to >90% will not work to reduce his obsessive behavior.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!

Get 30% Off Your Entire Order!
From November 30th to December 2nd, use the code “Cyber30″ for 30% off at checkout!
Save the date and shop our sale
For last week’s practice question, we quizzed participants on FIB-4 of 2.83. 48.09% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
AR lives with type 2 diabetes, and their waistline is 41 inches. Since their ALT and AST levels are elevated, you know they are at risk for steatosis (MASH). You quickly calculate their Fibrosis-4 Index (FIB-4), by plugging in AR’s Age, AST, ALT, platelet count into the FIB-4 calculator. AR’s result is 2.83.
According to the ADA Standards, with a FIB-4 value of 2.83, which action is required?
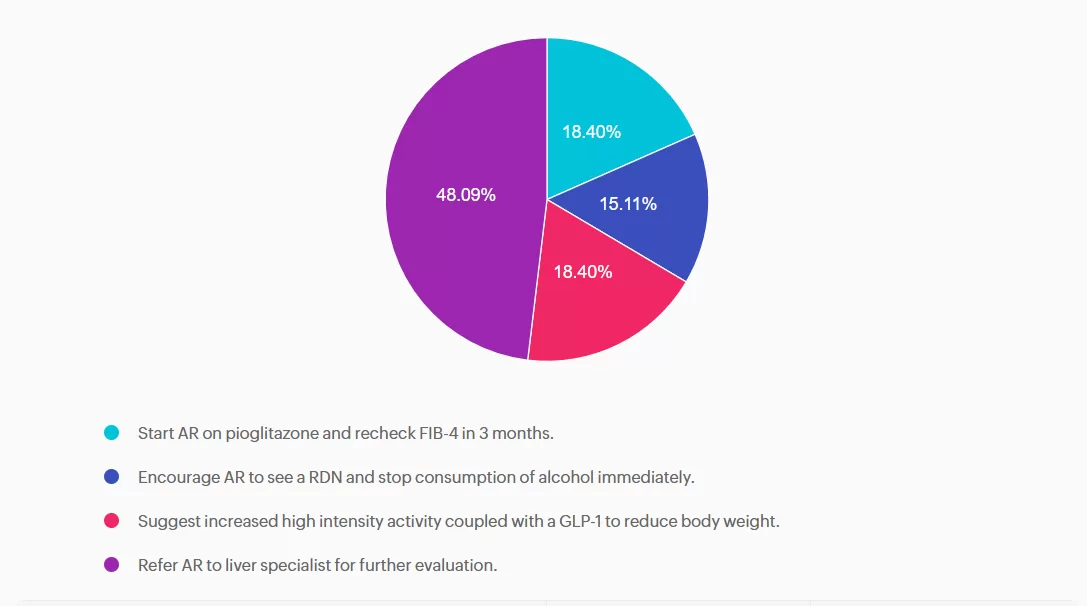
Answer A is incorrect: 18.4% chose this answer, “Start AR on pioglitazone and recheck FIB-4 in 3 months.” Although pioglitazone is a recommended treatment for steatosis, since AR’s FIB- is greater than 2.67, this indicates AR is at high risk for advanced fibrosis and a referral to a liver specialist is warranted.
Answer B is incorrect: 15.11% chose this answer, “Encourage AR to see a RDN and stop consumption of alcohol immediately.” Seeing a RDN is very important for AR to evaluate and customize an eating plan to address their steatosis and support quality of life. However, since AR’s FIB- is greater than 2.67, this indicates AR is at high risk for advanced fibrosis and a referral to a liver specialist is warranted.
Answer C is incorrect: 18.4% chose this answer, “Suggest increased high intensity activity coupled with a GLP-1 to reduce body weight.” Strength training and activity, coupled with a GLP-1 for GLP-1/GIP are important strategies to address steatosis. However, since AR’s FIB- is greater than 2.67, this indicates AR is at high risk for advanced fibrosis and a referral to a liver specialist is warranted.
Answer D is correct: 48.09% chose this answer, “Refer AR to liver specialist for further evaluation.” Great job! AR will require intensive intervention to decrease their risk of worsening steatosis, including MNT, targeted activities, and a referral to a liver specialist to determine the best treatment approach.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
For last week’s practice question, we quizzed participants on FDA approved treatment for MASH. 33.75% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
MJ just discovered that in addition to their type 2 diabetes and a BMI of 31, they also have MASH.
Based on this diagnosis, which FDA approved medication would help address their steatosis?
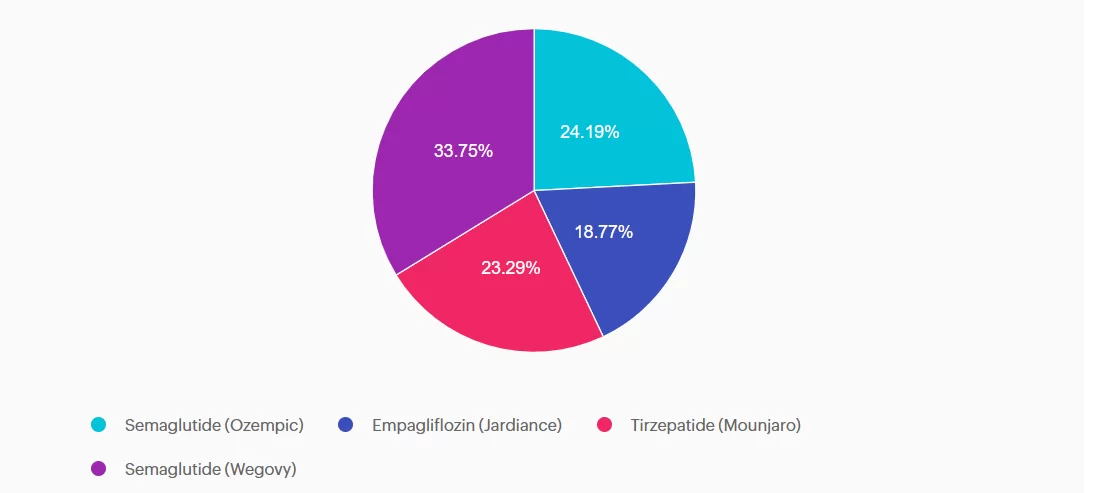
Answer A is incorrect: 24.19% chose this answer, “Semaglutide (Ozempic).” The diabetes approved version of semaglutide (Ozempic) does not yet have FDA approval as a medication that is used for treatment of MASH.
Answer B is incorrect: 18.77% chose this answer, “Empagliflozin (Jardiance).” Although empagliflozin will reduce blood glucose and can help with weight loss, it is not FDA approved for treatment of MASH.
Answer C is incorrect: 23.29% chose this answer, “Tirzepatide (Mounjaro).” Tirzepatide (Mounjaro) is approved for treatment of diabetes, helps with weight loss and is FDA approved for sleep apnea. However it is not FDA approved for treatment of MASH.
Answer D is correct: 33.75% chose this answer, “Semaglutide (Wegovy).” The weight loss approved version of semaglutide (Wegovy) has FDA approval as a medication that is used for treatment of MASH.
Please see our new “Indications for GLP-1/GIP” Cheat Sheet for a complete run down.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!

🌟Updated Schedule: ADA Boot Camp, Tech, MNT & More
Live in Beautiful San Diego – Oct 22-23, 2026
Re-Ignite your Passion & Prepare for Diabetes Certification Exams
🎓 Earn 30+ CEs: AMA PRA Category 1 Credits™, ACPE, ANCC, and CDR!
📅
2-Day Conference
Oct 22–23, 2026
⏱️
15.5 Live CEs
+ 17 bonus CEs
🏅
CDCES & BC-ADM
Exam Prep + Renewal
📍
San Diego, CA
1.7 mi from airport
The field of diabetes care is expanding and evolving rapidly. This unique training conference will keep you on the cutting edge plus prepare you for certification exams. It also fulfills the Standards of Care renewal requirement. Join us for two days of intensive education that is fun and inspiring. Add on the optional Day 3 (Engaging the Disengaged), to complete your conference exeperience.
Coach Beverly and Diana Isaacs, PharmD, BC-ADM, CDCES co-lead an exciting day that brings the ADA and AACE Standards to life. Gain fresh insights, practical tools, and a deeper understanding of the latest in person-centered diabetes care. After attending, you will be empowered to share the latest in diabetes care with your colleagues and the people in your care.
Take your knowledge to the next level with this intensive deep-dive into insulin therapy, dosing and pattern management with Dr. Diana Isaacs. Next, stay for the diabetes tech show-and-tell as Diana demonstrates the specs of the latest pumps and sensors. After lunch, nutrition whiz Christine Craig, MS, RDN, CDCES expertly details the latest in MNT and provides real strategies on translating this content to your clinical practice. You will have a chance to put it all together as Coach Beverly leads you through a series of case studies that integrates content from Day 1 and Day 2.
On Saturday, join this exceptional day-long program led by William H. Polonsky, PhD, CDCES & Susan Guzman, PhD (Behavioral Diabetes Institute) that reveals psychosocial forces behind diabetes self-management — tools to break through resistance and inspire change.
Read more below
📜 Essentials
Registration
+ Printed Syllabus
$559.00
🌟 Deluxe
Essentials
+ ADA Standards Book
$589.00
🏆 Complete – Best Value!
Deluxe
+ ADCES Review Guide e-Book
$669.00

Transform how you engage patients with diabetes — master behavior change, reduce distress, and overcome medication hesitancy.
Why do so many patients know what they should do — but still struggle to do it?
The answer lies in the psychology of diabetes.
In this transformative full-day course, world-renowned experts William H. Polonsky, PhD, CDCES, and Susan Guzman, PhD, from the Behavioral Diabetes Institute reveal the hidden psychosocial forces that drive — or derail — diabetes self-management.
You’ll walk away with a completely new toolkit for breaking through patient resistance, dissolving medication hesitancy, and creating clinical encounters that actually inspire change!
For last week’s practice question, we quizzed participants on Lifestyle Therapy for MASLD and MASH. 83% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
PJ has had type 2 diabetes for 8 years and is here for a follow-up visit. Labs indicate A1c at 7.2%, lipids at target, eGFR of 78 mL/min/1.73m², and urine albumin-to-creatinine ratio (UACR) of 65 mg/dL. Blood pressure at the office visit today was 142/86, which is consistent with home monitored values. PJ confirms taking medications, metformin and simvastatin. PJ inquires about recently completed lab work.
According to the ADA Standards of Care, what would be an appropriate next step in the diabetes care plan?
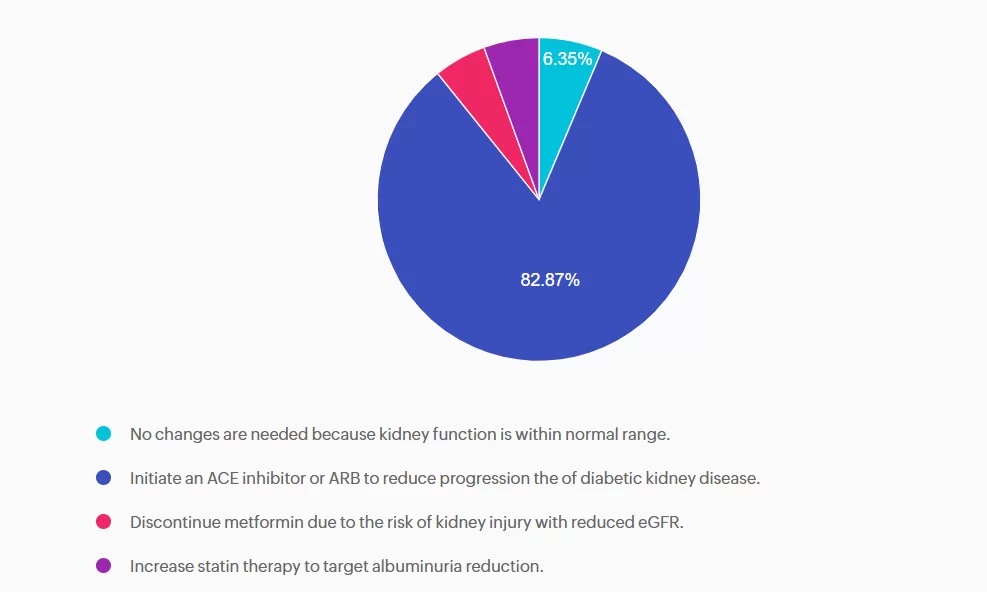
Answer A is incorrect: 6.35% chose this answer, “No changes are needed because kidney function is within normal range.” A is incorrect. Although eGFR indicates stage 2 kidney disease, the elevated UACR, ≥30 mg/g, confirms moderately increased risk and recommendation to treat. Additionally, PJ’s blood pressure is also above the target. Intervention is needed to protect kidney and cardiovascular health.
Answer B is correct: 83% chose this answer, “Initiate an ACE inhibitor or ARB to reduce progression the of diabetic kidney disease.” PJ has a mildly decreased eGFR, but UACR is elevated above 30 mg/g, indicating a recommendation to treat. Additionally, intervention is needed to optimize blood pressure. According to the ADA Standards of Care in Diabetes, individuals with diabetes, hypertension, and moderately increased albuminuria should be treated with an ACE inhibitor or angiotensin receptor blocker. The use of sodium-glucose cotransporter 2 (SGLT2) inhibitors or glucagon-like peptide 1 agonists (GLP1-RA), with demonstrated benefits, could also be considered to reduce CKD progression.
Answer C is incorrect: 5.25% chose this answer, “Discontinue metformin due to the risk of kidney injury with reduced eGFR.” Metformin is safe to continue unless eGFR falls below 30 30 mL/min/1.73m². PJ’s kidney function is adequate for continued use. However, consideration to add a change to SGLT2 or GLP1 with kidney benefit could also promote additional A1c reduction.
Answer D is incorrect: 5.52% chose this answer, “Increase statin therapy to target albuminuria reduction.” Statins are recommended for ASCVD prevention, but they do not reduce albuminuria. Lipids are within normal range, and albuminuria should be addressed with an ACE inhibitor/ARB or potentially a SGLT2 inhibitor or GLP-1 RA.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!

Explore the magnificent world of diabetes and the gut — from periodontal disease to the microbiome and everything in between.
Join Coach Beverly Thomassian, RN, MPH, CDCES, BC-ADM, for a fascinating journey through gastrointestinal health from top to bottom. This course covers fatty liver disease, gastroparesis, intestinal complications of diabetes, the gut microbiome, and more — giving you the knowledge to better support whole-body health.
For last week’s practice question, we quizzed participants on insulin. 96% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
R.S. is a 60-year-old with type 2 diabetes who was recently placed on insulin lispro at meals. He has taken insulin glargine once a day for five years. Previously, non-insulin medications have been ineffective or not tolerated. He continues to have hyperglycemia despite the addition of insulin lispro. During his diabetes education visit today, he shared that he has not been taking his mealtime insulin lispro because he does not want to inject it in front of his grandchildren, who live with him. He feels overwhelmed by these additional injections but wants to get his blood glucose levels under better control so he can have the energy to play with his grandchildren and avoid losing his eyesight like his mother did.
As the diabetes care and education specialist, which of the following would be the most appropriate first step in addressing R.S.’s concerns?
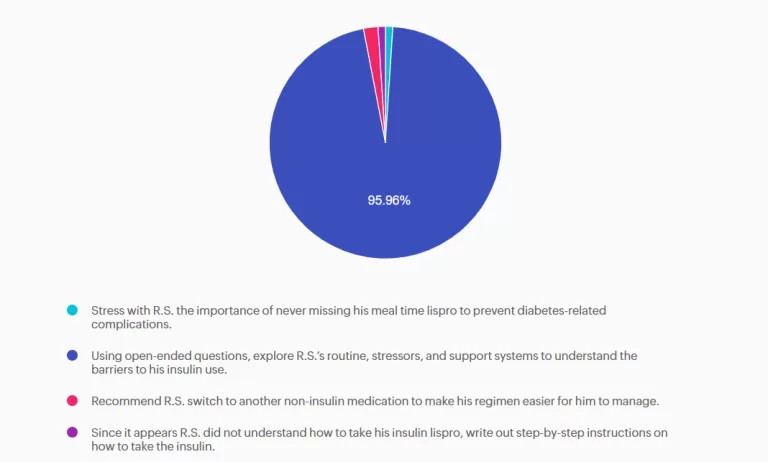
Answer A is incorrect: 1% chose this answer, “Stress with R.S. the importance of never missing his meal time lispro to prevent diabetes-related complications.” R.S. is aware that his glycemic control is important, and he is already aware of the risk of diabetes-related complications. Counseling him on this would not help him be successful with his insulin management.
Answer B is correct: 96% chose this answer, “Using open-ended questions, explore R.S.’s routine, stressors, and support systems to understand the barriers to his insulin use.” R.S. is struggling with barriers to successful insulin management. A holistic approach would be to ask open-ended questions about his current routine, stressors, and support systems to gain a better understanding of these barriers. This information can lead to a personalized plan of care to help improve glycemic control.
Answer C is incorrect: 2% chose this answer, “Recommend R.S. switch to another non-insulin medication to make his regimen easier for him to manage.” He has already attempted other non-insulin therapies, and these were either ineffective or not tolerated. Changing his regimen would not be successful at improving his glycemic control and quality of life.
Answer D is incorrect: 1% chose this answer, “Since it appears R.S. did not understand how to take his insulin lispro, write out step-by-step instructions on how to take the insulin.” R.S. appears to understand how to take his insulin lispro at meals. Writing out the instructions would not improve his situation. It is not a lack of knowledge, but the multiple barriers in his life that are keeping him from being able to implement this new medication regimen.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!

Invite a colleague to our DiabetesEd Seminar in San Diego and get $75 off each registration.
Use code FriendDiscountSD during check out to save.
30+ CEs with Expanded Accreditation!

Join our expert team for engaging, interactive sessions that bring the ADA Standards of Care to life—covering medications, behavior change, technology, and more. Ideal for CDCES or BC-ADM exam prep, this course also includes a 4-hour Virtual Medical Nutrition Therapy Toolkit and bonus content that also meets CDCES renewal requirements.
Upon completion of this activity, participants should be able to:

Diana Isaacs, PharmD, BCPS, BCACP, CDCES, BC-ADM, FADCES, FCCPCES

Beverly Thomassian, RN, MPH, CDCES, BC-ADM
Our expert team transforms complex diabetes science into clear, practical insights—keeping it real, engaging, and fun!
Program Faculty Disclosures:
Partners for Advancing Clinical Education (Partners) requires every individual in a position to control educational content to disclose all financial relationships with ineligible companies that have occurred within the past 24 months. Ineligible companies are organizations whose primary business is producing, marketing, selling, re-selling, or distributing healthcare products used by or on patients.
All relevant financial relationships for anyone with the ability to control the content of this educational activity are listed below and have been mitigated according to Partners policies. Others involved in the planning of this activity have no relevant financial relationships.
Faculy Bios & Disclosures:
 Coach Beverly Thomassian RN, MPH, CDCES, BC-ADM – CEO of DiabetesEd Services
Coach Beverly Thomassian RN, MPH, CDCES, BC-ADM – CEO of DiabetesEd ServicesDisclosures:
Beverly Thomassian has no financial disclosures
Bio:
 Diana Isaacs, PharmD, BCPS, BCACP, CDCES, BC-ADM, FADCES, FCCPCES
Diana Isaacs, PharmD, BCPS, BCACP, CDCES, BC-ADM, FADCES, FCCPCES
Disclosures:
Dr. Diana Isaacs has the following relevant financial relationships:
Bio:
Diana Isaacs was awarded 2020 ADCES Diabetes Educator of the Year for her educational platform promoting the use of CGM for people with diabetes and other innovations. She serves in leadership roles for several pharmacies and diabetes organizations. She has numerous diabetes publications and research projects with a focus on medications, CGM and diabetes technology.
For the past three year, Dr. Isaacs has served as a contributing author for the 2023 ADA Standards of Care.
As the Program Coordinator and clinical pharmacist specialist in the Cleveland Clinic Diabetes Center, Dr. Isaacs brings a wealth of clinical knowledge combined with extensive research and speaking experience to this program.
Activity Start and End Date: 10/22/25 – 10/23/2025
Estimated time to complete the activity: 15 hours and 30 minutes
_____________________________________
Jointly provided by Partners for Advancing Clinical Education and Diabetes Education Services
![]()
![]()
Joint Accreditation Statement:
![]() In support of improving patient care, this activity has been planned and implemented by Partners for Advancing Clinical Education (Partners) and Diabetes Education Services. Partners is jointly accredited by the Accreditation Council for Continuing Medical Education (ACCME), the Accreditation Council for Pharmacy Education (ACPE), and the American Nurses Credentialing Center (ANCC), to provide continuing education for the healthcare team.
In support of improving patient care, this activity has been planned and implemented by Partners for Advancing Clinical Education (Partners) and Diabetes Education Services. Partners is jointly accredited by the Accreditation Council for Continuing Medical Education (ACCME), the Accreditation Council for Pharmacy Education (ACPE), and the American Nurses Credentialing Center (ANCC), to provide continuing education for the healthcare team.
Physician Continuing Education:
Partners designates this enduring material for a maximum of 15.50 AMA PRA Category 1 Credit(s)™. Physicians should claim only the credit commensurate with the extent of their participation in the activity.
Nursing Continuing Professional Development:
The maximum number of hours awarded for this Nursing Continuing Professional Development activity is 15.50 contact hours.
Pharmacy Continuing Education:
Partners designates this continuing education activity for 15.50 contact hour(s) (1.550 CEUs) of the Accreditation Council for Pharmacy Education.
(Universal Activity Number – JA4008073-9999-25-206-L01-P)
Type of Activity: Application
For Pharmacists: Upon successfully completing the activity evaluation form, transcript information will be sent to the NABP CPE Monitor Service within 4 weeks.
Dietitian Continuing Education:
This program offers 15.50 CPEUs for dietitians.
Interprofessional Continuing Education:
![]() This activity was planned by and for the healthcare team, and learners will receive 15.50 Interprofessional Continuing Education (IPCE) credit for learning and change.
This activity was planned by and for the healthcare team, and learners will receive 15.50 Interprofessional Continuing Education (IPCE) credit for learning and change.
For additional information about the accreditation of this activity, please visit https://partnersed.com.
The use of DES products does not guarantee the successful passage of the certification exam. CBDCE and ADCES do not endorse any preparatory or review materials for the CDCES or BC-ADM exams, except for those published by CBDCE & ADCES.
For last week’s practice question, we quizzed participants on RT forgetting their insulin, and what would be the best response. % of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Grace is a 38-year-old female who has lived with type 1 diabetes for 20 years. She is a nurse and works variable shifts. She voices concern today about her hemoglobin A1c being elevated at 8.4% over the past 6 months. She is doing everything she can to manage her diet, daily exercise routine, and reports rarely missing insulin doses. She is currently using a Dexcom G7 CGM.
She has never pursued insulin pump therapy because she was fearful that she would no longer be in control of her diabetes if she used a pump. She is now interested in an automated insulin delivery system and asks you which pump is “best” for controlling blood sugar.
What is the best way to answer this question?
Answer A is incorrect: % chose this answer, “Discuss the insulin pump options that connect with the Dexcom G7 CGM. This will help simplify her transition to pump therapy by minimizing the learning curve when starting an AID system.” Although some insulin pumps are compatible with the Dexcom CGM, switching to a different CGM supplier should not restrict clients from selecting the insulin pump that best suits their needs.
Answer B is incorrect: % chose this answer, “Acknowledge Grace’s interest in insulin pump technology and recommend that she wait until more advanced insulin pump algorithms are available that are easier to use.” Automated insulin delivery systems offer advanced automation. Waiting for future technology will not help Grace improve glycemic control now.
Answer C is incorrect: % chose this answer, “Recommend that Grace use a tubeless pump as it will suit her better due to her work as a nurse and active lifestyle. This will help to avoid tubing issues or the insertion site becoming dislodged.” The type of pump, with or without tubing, is a personal decision and is not based solely on occupation.
Answer D is correct: % chose this answer, “Review with Grace the details of all the available insulin pumps, algorithms, and compatible CGMs so she can make a personalized decision based on her preferences and lifestyle.” Choosing the right insulin pump is a highly personalized decision. Each insulin pump has different variables and CGM connectivity that must be considered. Grace will need to be educated on the available options so she can determine which insulin pump will work best for her.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!