
Subscribe
eNewsletter
Ready to get certified?
Free CDCES Coach App
eNewsletter
Free CDCES Coach App
Wow! This is fantastic news. I sit for the CBCDE Exam for the 7th time next year, and I am definitely going to take advantage of this remote feature! ~ Coach Beverly
The Certification Board for Diabetes Care & Education (CBDCE) is now offering the opportunity to take your Certified Diabetes Educator (CDCES) exam remotely!
By the end of this year, you will have the option to take your certification exam using their new Live Remote Online Proctoring (LRP) platform.

LRP is a secure and non-invasive platform that uses professional proctors and technology to monitor candidates live while they complete the Certification Examination for Diabetes Care and Education Specialists (Exam). This method of test delivery allows the candidate to take the exam from their home, office or a remote site, using their own computer. The process is secure, easily accessible, and monitors testing activity and records all aspects of the exam testing session.
During your exam appointment, you will be connected with a moderator who will guide you through the process and be there throughout your entire exam. You will need to share your screen and broadcast yourself during your entire exam. Your workspace should be quiet, tidy, and free of any study notes/materials.
No electronics, besides the computer you are taking the test on are allowed. However, since there may be math questions, a basic calculator is allowed after clearance by the moderator. A 10-minute break is an option, but no changes to completed test questions are allowed after the break. In addition, the moderator will need to rescan your workspace to make sure it is free of study notes and materials. After you take the exam, you will instantly get a report of your results.
To connect to the LRP platform, you will need a computer with a webcam and microphone. The CBDCE recommends that you run compatibility tests before your exam to ensure your equipment is compatible.
To learn more about LRP, watch the 4-minute video below and read the Guide to Live Remote Online Proctoring (LRP)

Join us to get ready to succeed a the CDCES Exam. This course will transform your test anxiety into calm self-confidence and test-taking readiness.
Topics covered include:
We will review sample test questions and the reasoning behind choosing the right answers.
After registering, you will receive a confirmation email containing information about joining the webinar.
Intended Audience: This FREE webinar is designed for individuals or groups of diabetes educators, including RNs, RDs, Pharmacists, Nurse Practitioners, Clinical Nurse Specialists, Physician Assistants and other health care providers interested in achieving excellence in diabetes care and becoming Certified Diabetes Care and Education Specialists®.
Can’t make it live? All paid registrants are guaranteed access to the video presentation, handouts and podcasts.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
JR is 43 years old with newly discovered type 2 diabetes.
According to the ADA Standards, which of the following actions needs to be taken with a new type 2 diabetes diagnosis?
Click here to test your knowledge!
Want to learn more about this topic? Enroll in our

This 2 hours course provides a detailed overview of the pathophysiology of type 2 diabetes, prevention strategies, and cardiovascular risk reduction. In addition, we highlight type 2 treatment approaches including nutrition, activity, oral and injectables medications plus screening and treatment guidelines for micro and macrovascular disease. Through case studies and discussion, we highlight strategies to focus on a person-centered approach along with attention to psychosocial care for people living with diabetes.
Objectives:
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.

For our May 18th Question of the Week, 76% of respondents chose the best answer, which is awesome! We still want to “take a closer look” at this question.
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer below: Answer Question
Question: CT was diagnosed with type 2 diabetes three years ago. The current medication regimen includes 1000 mg of metformin twice daily and 70 units of glargine at night. CT wears an intermittent sensor, and you look at the glucose trends together on CT’s phone app. You both agree that there are consistent postmeal spikes up to 250 almost every day after lunch and dinner. The lowest blood sugar readings are in the 100s. BMI is 33.8 and CT says, “I never feel full”. The most recent A1C is 8.2%, urinary albumin creatinine ratio less than 30.
Based on this information, what intervention would be most likely help CT get to recommended ADA targets?
Answer Choices:
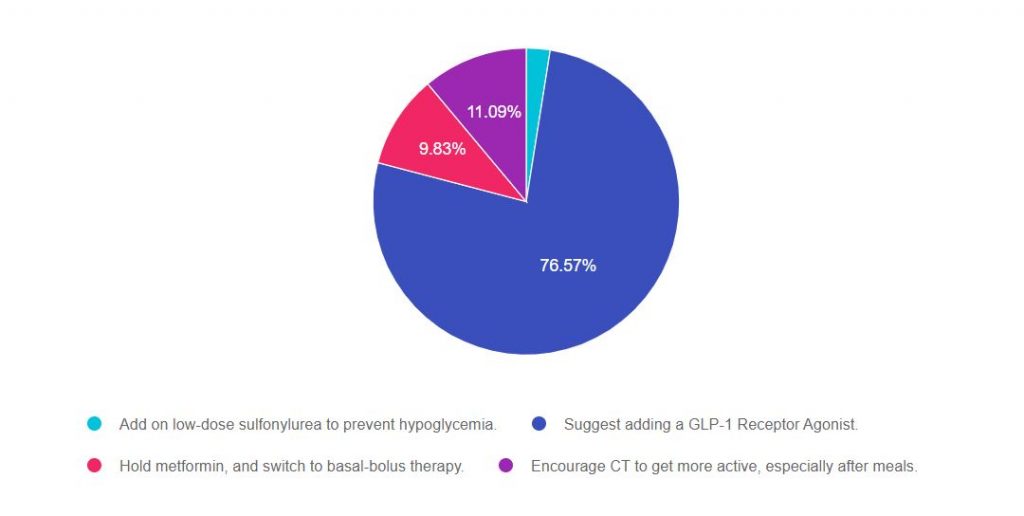
As shown above, the most common choice was option 2, the second most common answer was option 4, then option 3, and finally option 1.
If you are thinking about taking the certification exam, the content of this practice test question will set you up for success. The exam will present questions that require test takers to be familiar with the stepwise approach to type 2 diabetes management in a variety of settings and situations.
For a complete listing of diabetes medications, please Download our Medication PocketCards.
Answer 1 is incorrect, 2.51% chose this answer, “Add on low-dose sulfonylurea to prevent hypoglycemia.” Although we might consider this option, we can quickly identify a “tacked on” second half of the answer that makes it a wrong choice. One of the major side effects of sulfonylureas is hypoglycemia, so adding this class of medication wouldn’t prevent hypoglycemia, it would actually increase the risk of low blood sugars.
Answer 2 is correct, 76.57% of you chose this answer, “Suggest adding a GLP-1 Receptor Agonist.” GREAT JOB! Given the fact that CT is on 70 units of basal plus metformin and is experiencing postmeal spikes up to 250 almost every day after lunch and dinner and “never feels full”, adding a GLP-1 is the best choice. Adding a GLP-1 will decrease post meal hyperglycemia and postprandial glucose. In addition, GLP-1s can decrease appetite and increase feelings of satiation. Before suggesting addition of this medication class, it is important to consider insurance coverage and out of pocket cost, since cost could be a barrier.
Answer 3 is incorrect, 9.83% of you chose this answer, “Hold metformin, and switch to basal-bolus therapy.” According to the ADA, when initiating basal bolus insulin therapy for people with type 2 diabetes, they recommend continuing metformin to decrease insulin resistance. The ADA also suggests considering adding a GLP-1 RA or SGLT-2 Inhibitor before switching to basal bolus therapy.
Answer 4 is incorrect, 11.09% of you chose this answer, “Encourage CT to get more active, especially after meals.” While activity is important, this goal is very vague and not really actionable. In addition, “getting active after meals” will certainly improve health and is a great recommendation, but is not likely to drop the A1c to less than the goal of 7% or help with appetite.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Want to learn more about this topic? Join us for our upcoming

Why are glucose levels elevated in the morning? When should insulin be started? What is the next step to get A1c to target?
During this course Coach Beverly addresses each of these glucose mysteries and more, using a person-centered approach. She describes a stepwise approach to evaluate glucose patterns and correct common issues encountered by people living with type 2 diabetes.
By attending this webinar, you will gain confidence in evaluating glucose patterns and making recommendations for improvement.
Objectives
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
For the past year, as the only diabetes nurse educator at a local FQHC clinic, I have had to fine-tune my nutrition coaching skills. We are hoping to hire a dietitian soon, but in the meantime, I am trying to find my nutrition groove as I work with Spanish-speaking clients, kids to elders, and everyone in between.
For many years, I shied away from using the plate method and mostly relied on dietary recalls and figuring out changes needed to improve the health quotient of their current meal plan.
However, as people walk into my clinic room, I am surprised by how many are drawn to the oversized healthy plate place-mats sitting on my display table. They ask, “Can I eat these foods?” This sparks a lively and constructive conversation on new approaches to eating.
Based on this enthusiastic response, after I complete the dietary recall, I jump into our food conversation using the plate method. Whether am I coaching kids to elders on healthy eating, this approach seems to get the best response. If needed, I will dive into more detail around carb serving sizes and matching carbs to insulin.
Using the plate method allows me to keep it person-centered and help them include their favorite foods to maintain the pleasure of eating.
This teaching tool is ideal because it has appealing pictures of the different foods that make it easy to provide a quick review of the food groups and their impact on blood sugars and overall health.
In addition, these plates represent a variety of cultures and eating styles, and come in several languages. Here is the one in Spanish I use all the time.
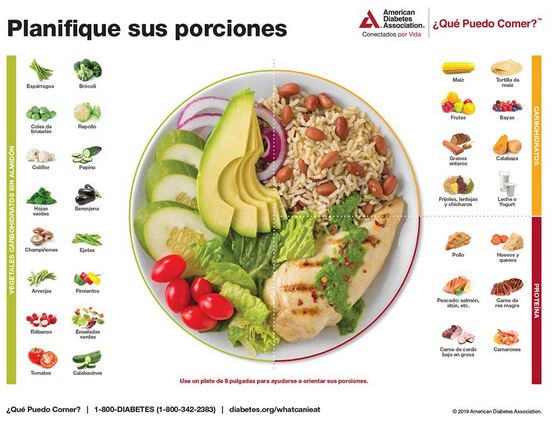
Take a vegetable tour: I start on the left side of this place mat, which has pictures of a variety of healthy high fiber vegetables, which I emphasize are low in calories and packed with nutrients. Then I ask which vegetables are they currently eating and provide encouragement to continue and expand their veggie choices, if possible. “Enjoy an abundance of these super foods, that fill you up, feed your good bacteria, decrease inflammation, help manage blood sugars and support a healthy weight.”
Next stop – CARBS and Beans – There is a lot of misinformation around the carbohydrate group and many people tend to lump them in the “bad food” category. We discuss the carbs they are consuming and discuss some they might be missing out on, like fruits or tortillas, thinking they were off-limits. I encourage 3 servings of fruit daily, (the size of a closed fist) spread throughout the day.
Beans, the magical fruit! I make an intentional effort to sing the praises of beans. They are the inexpensive, fiber-packed nutrition superstars and they are so versatile.
A big focus with carbs is portion sizes. The actual amount of carbs someone is consuming is really easy to underestimate. For this part, I DO pull out my rubber food models, which are as popular as ever.
Canned and Frozen veggies are good for you. Many people may not have access to fresh vegetables or refrigeration. Canned vegetables and soups are often a cheaper, more realistic option. They can choose low sodium if they have hypertension or they can rinse off salty, often less expensive canned vegetables. If they have access to a freezer, frozen veggies offer as many nutrients (and sometimes more) than fresh vegetables, especially if they have been on the shelf for a while.
I encourage starting meals with soups, salads, or water if they are trying to lose weight.
Protein and meats – Our discussion focuses on serving sizes and healthy ways to prepare low fat or skinless meats. If their LDL cholesterol is above target, we will include a discussion on meat alternatives and review cheese consumption.
Sugary Beverages, Sweet Treats, and Snacks – Coffee with a little cream and sugar is fine, but those coffee drinks topped with whip cream can pack lots of carbs and unwanted calories. Replacing sports drinks and sodas with water or unsweetened tea can make a huge difference in glucose levels and body weight.
Mindless muching. I find many people munching on snacks and sweet treats (especially in the evenings) out of boredom or in response to stress. Helping people ask themselves, “Am I really hungry?” before that first bite can make a big difference. Also keeping track of the emotion associated with “mindless snacking” can help people discover other strategies to deal with uncomfortable feelings.
The plate method is simple, engaging of fun. We can customize the plate based on their food favorites and help individuals and families improve their health and feel better!
Get Started on the ADA Diabetes Food Hub – Sign up to save recipes, create a personalized grocery list, and more.
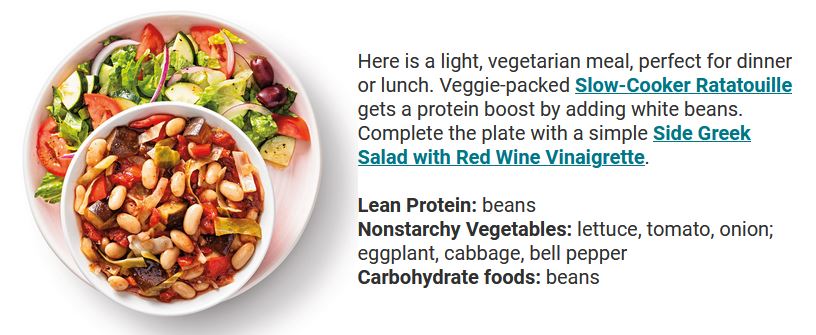
Please visit the ADA’s Diabetes Food Hub recipe page.
They have an abundance of recipes based on budget, preferred foods, time of day, etc… Plus, they also provide the nutrition facts, and it’s FREE!
ADA website: https://www.diabetesfoodhub.org/
Check out Awesome photos and ideas modeling the “Diabetes Plate Method”
USDA Plate Method Website has lots of great info
THE EXCHANGE LIST for Diabetes
Join us for our live streaming of our brand new course

Determining basal and bolus rates for multiple daily injections or insulin pumps can seem overwhelming. This 90-minute course provides participants with a step-by-step approach to determine basal rates, bolus ratios and how to problem solve when blood glucose levels aren’t on target. During this 90-minute course, Coach Beverly will provide abundant case studies to give participants hands-on practice and build confidence when calculating insulin doses for a variety of situations.
Objectives:
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
Managing diabetes can be tough! Something that people rarely talk about is how tough type 1 diabetes can be and how many people find diabetes to be stressful and challenging.
That’s why we are excited to share an opportunity for people living with type 1 diabetes to join a new NIH-supported study that is part of a collaboration between T1D Exchange and the University of California, San Francisco (UCSF).
I have had the pleasure of working as an Embark facilitator for the past year.
I can personally share with you that this program offers so much meaningful hands-on problem solving and support for those who join. Participants not only receive practical information but gain valuable insights into approaches for self-care.
I highly recommend this program to anyone with type 1 diabetes who is feeling frustrated and tired and ready to make changes with the help of a supportive team!
The program begins with a group workshop (8-12 adults with type 1 diabetes) (held virtually online on a Saturday), followed by online video group meetings and/or individual phone calls with either a psychologist or Certified Diabetes Educator.
The program interventions are strictly behavioral, meaning that participants will not be asked to change or try any new medications or devices.
Participants will receive gift cards for their time and there are no costs to you or to your insurance. There is no age limit to taking part, you just need to be 19 years or older!
If you know people living with type 1 diabetes, please share this information with them. Our hope is that they will be interested in learning more about this exciting new program.
Research Participants Needed:
Are you…
– An adult (19 years +)
– Diagnosed with Type 1 Diabetes for at least 1 year
– Unhappy with your recent Hemoglobin A1C of 7.5% or higher
– Feeling overwhelmed, frustrated, “burned out” with living with diabetes
If you answered YES to the above questions, you may qualify to participate in EMBARK. The purpose of this study is to work compassionately to help you better manage your distress with diabetes and to reach your management goals.
Or you can call: 1-855-850-3599 (toll free) or email us at: [email protected]. Thank you, UCSF EMBARK Team
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
CT was diagnosed with type 2 diabetes three years ago. The current medication regimen includes 1000 mg of metformin twice daily and 70 units of glargine at night. CT wears an intermittent sensor, and you look at the glucose trends together on CT’s phone app. You both agree that there are consistent postmeal spikes up to 250 almost every day after lunch and dinner. The lowest blood sugar readings are in the 100s. BMI is 33.8 and CT says, “I never feel full”. The most recent A1C is 8.2%, urinary albumin creatinine ratio less than 30.
Based on this information, what intervention would be most likely help CT get to recommended ADA targets?
Click here to test your knowledge!
Want to learn more about this topic? Join us for our
Why are glucose levels elevated in the morning? When should insulin be started? What is the next step to get A1c to target?
During this course Coach Beverly addresses each of these glucose mysteries and more, using a person-centered approach. She describes a stepwise approach to evaluate glucose patterns and correct common issues encountered by people living with type 2 diabetes.
By attending this webinar, you will gain confidence in evaluating glucose patterns and making recommendations for improvement.
Objectives
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
Most of you, 69%, chose the best answer for our May 11th Question of the Week. Great job! We wanted to “take a closer look” into this question.
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer below: Answer Question
Question: RT is 33 years old and has had diabetes for the past 20 years. RT uses an insulin pump and CGM and works hard to keep A1cs less than 7%. Their most recent A1c increased to 7.9% and RT sets up an appointment with the diabetes specialist for help. After downloading the report, the specialist thinks they have discovered the reason behind the increasing A1c.
Which of the following would most likely explain the A1c increase?
Answer Choices:
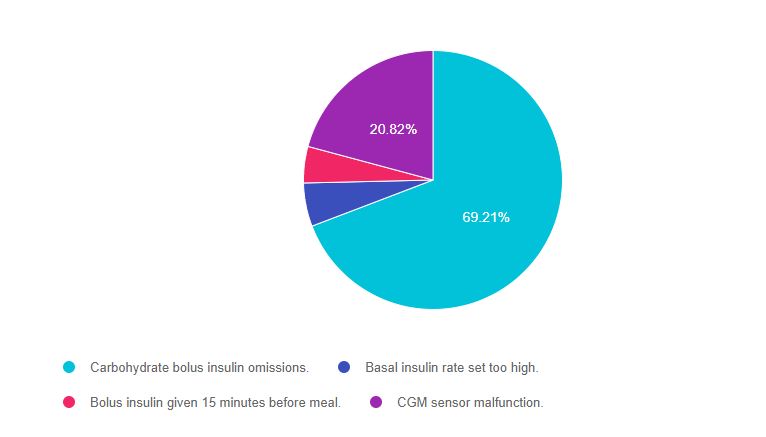
As shown above, the most common choice was option 1, the second most common answer was option 4, then option 2, and finally option 3.
If you are thinking about taking the certification exam, the content of this practice test question will set you up for success. The exam will present questions that require test takers to be familiar with diabetes technology and helping people with problem solving and getting glucose to target.
Answer 1 is correct, 69.21% chose this answer, “Carbohydrate bolus insulin omissions.” GREAT JOB! Skipping coverage for carbs, even once a day, can lead to a 1% increase in A1c. When discussing the data download with RT, the diabetes specialist will recognize all the actions that RT is doing correctly. Then, the specialist will share their observations that it seems RT sometimes skips bolusing for carb intake. The specialist can pause and see what RT says or the specialist could say something like, “can you tell me more about what is happening around these meals?”
Answer 2 is incorrect, 5.43% of you chose this answer, “Basal insulin rate set too high.” Getting to the correct basal rate is important to maintain glucose levels on target. If the basal rate is set too high, this means that RT would be getting too much insulin. This would result in hypoglycemia and a drop in A1c.
Answer 3 is incorrect, 4.55% of you chose this answer, “Bolus insulin given 15 minutes before meal.” The timing of bolus insulin before meals can make a big difference in getting glucose to target. Giving bolus insulin 15 minutes before meals can actually improve glucose levels since it allows the insulin peak to more closely match the post meal glucose elevation.
Answer 4 is incorrect, 20.82% of you chose this answer, “CGM sensor malfunction.” This is a juicy answer, but it doesn’t match the intent of the question. If the question said, “according to the CGM download the estimated A1c is 7.0% and the lab A1c is 7.9%” then we might consider this answer. However, we have no indication that the CGM sensor wasn’t working, nor do we have any data from the CGM to consider. That’s why this juicy answer is not the best one.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Determining basal and bolus rates for multiple daily injections or insulin pumps can seem overwhelming. This 90-minute course provides participants with a step-by-step approach to determine basal rates, bolus ratios and how to problem solve when blood glucose levels aren’t on target. During this 90-minute course, Coach Beverly will provide abundant case studies to give participants hands-on practice and build confidence when calculating insulin doses for a variety of situations.
Objectives:
Can’t join live? No worries, we will record the webinar and post it to the Online University!
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
In preparation for my updating my class “Basal Bolus Therapy in the Hospital Setting“, a quick google search on the latest trends in hospital and diabetes care highlighted this just-published article to my immediate attention.
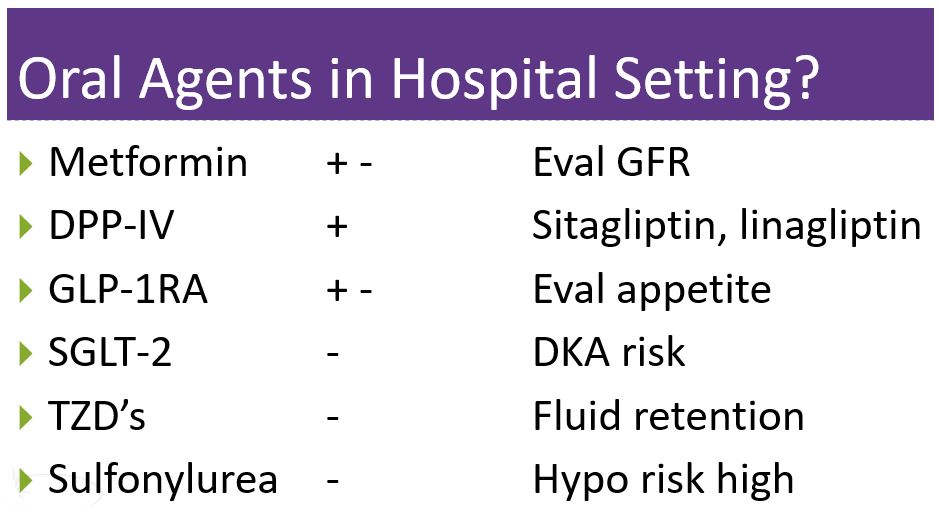
Management of diabetes and hyperglycemia in the hospital – Lancet 2021: 9 174-288 published in March 2021, provides evidence-based information and easy-to-use algorithms on managing hyperglycemia in the inpatient setting. It also addresses the use of CGM and insulin pumps in hospitals.
For this blog, I want to discuss some changes in approaches to hospital management, that I think is long overdue!
Take a look at the algorithm below and see if you agree with my takeaways below.
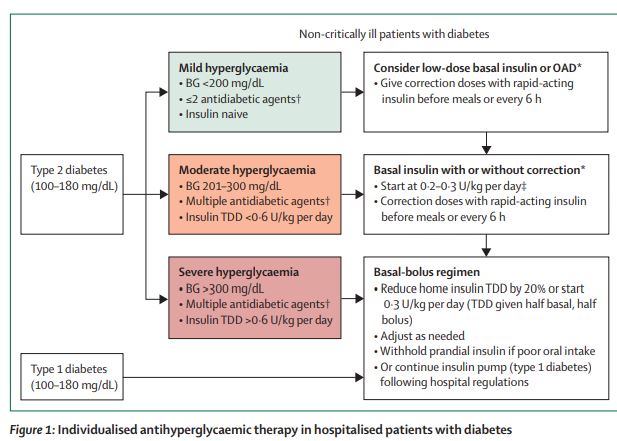
As a hospital-based diabetes nurse for a few decades, I have watched the evolution of inpatient diabetes management. With this new article, it feels like we have reached a more thoughtful middle ground, based on evidence and clinical experience.
Certainly, the insulin sliding scale alone is not effective to manage glucose levels. But this nuanced approach of considering orals with low dose basal insulin for those at risk of hypoglycemia and using basal/bolus for those who are more insulin resistant makes good sense to me.
What do you think?
I have more takeaways to share! Join Coach Beverly for her Basal Bolus Therapy in the Hospital Setting Webinar on May 6th at 11:30. And don’t worry if you can’t join us live, you will have access to the recorded version for a year after purchase.
Why are glucose levels elevated in the morning? When should insulin be started? What is the next step to get A1c to target?
During this 60-minute course Coach Beverly addresses each of these glucose mysteries and more, using a person-centered approach. She describes a stepwise approach to evaluate glucose patterns and correct common issues encountered by people living with type 2 diabetes.
By attending this webinar, you will gain confidence in evaluating glucose patterns and making recommendations for improvement.
Objectives
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.