
Subscribe
eNewsletter
Ready to get certified?
Free CDCES Coach App
eNewsletter
Free CDCES Coach App
One of the most frequently asked questions about the CDCES Exam is the following:
In this years exam handbook, the CBDCE provided clarification on this high anxiety topic.
Immediately – New diagnostic criteria or specific guidelines impacting diabetes care and education and/or treatment of diabetes which are released nationally and identified as effective immediately may be including in the examination at any time.
One Year – New medical advances, guidelines, or pharmaceuticals will be included in CDCES Exam no sooner than one year after the information is released.
If you have already studied the ADA 2020 Standards of Care, you will be set for the 2021 CDCES Exam. Since there are no new diagnostic criteria or specific guidelines that are dramatically different from the 2020 Standards of Care.
The one exception is that there are updated diabetes management guidelines for the older population as outlined in our Older People Level 2 Course and you can review in the ADA Standards of Care, section 12.
Please see ADA Standards Summary of Revisions for more detailed information on updates for 2021.
Great. Please plan on studying the 2021 ADA Standards of Care, which includes all of the same content as the 2020 Standards with some additions and updates.
We are all rooting for your success! For More info:
Join our Prep for CDCES Webinar FREE for lots of great info and to get ready!
Join our Diabetes Ed Specialist Conference

Whether you are new to diabetes or a seasoned expert, you’ll benefit from this virtual conference with the latest research plus critical content that you can immediately apply to your clinical practice.
Entire Program Fee: $399
Program Flyer: Download
Dates: April 15-17
Live Webinar Schedule: All webinars start and end times are in Pacific Standard Time
Program Schedule & Expert Bios
If you are interested in taking the CDCES or BC-ADM exam or are seeking a state of the art review of current diabetes care, this course is for you. Our team of expert faculty has been fine-tuning this course for over fifteen years, and we know what you need. In addition to informative lectures, we also use group activities and case studies to highlight the essential knowledge, skills, and strategies needed to succeed in diabetes education today!
In this course, the same speakers will cover the same content as outlined in the Live Seminar. For more details see our Virtual DiabetesEd Specialist Conference Schedule and Faculty.
Prepare for CDCES or BC-ADM certification or earn hours for renewal.
Come join our Virtual DiabetesEd Specialist Program.
Your registrations include access to all the Online Sessions plus Bonus Courses through December 31st, 2021.
This virtual program includes:
3 day live webinar courses from April 15th-17th (20 CEs) + enrollment in our Bonus Bundle (14.0+ CEs) from now through December 2021.
View full Conference Schedule and Faculty.
Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
The ADA Standards inform our practice and are critical for certification exams success. We invite you to join our Level 2 course series.
Coach Beverly updates these Level 2 courses throughout the year. Your registration includes the recorded courses and an invitation to the live webinars – see dates below. Please be reassured that the 2020 courses are still accurate and relevant for this years’ exam and your clinical practice.
You can purchase and view all of these courses immediately. With your registration, you are automatically invited to the Live Webinar update.
Each course includes: Video presentation, podcast, handouts and resources. We hope you can join us!
| Record Date or Upcoming Date | Topic and Standards of Care |
| Feb 2, 2021 | Standards of Care Overview Annual Update All Standards |
| 2021 | Assessing Coping Skills 1.5 CEs 2021 Includes Standards 1 and 5 | Pop Health & Promoting Well Being |
| 2021 | Hyperglycemic Crisis 1.0 CEs Standard 15 | Diabetes Care in the Hospital |
| 2020 | Meds Management for Type 2 – 1.5 CEs Standard 9 | Pharmacologic Approaches to Glycemic Tx |
| April 28, 2021 | Critical Assessment of People with Diabetes 2.0 CEs Standard 4 | Comprehensive Medical Eval |
| April 21, 2021 | Lower Extremity Assessment 1.5 CEs Standards 11 | Foot Care |
| 2021 | Older Adults and Diabetes 1.5 CEs Standard 12 |Older Adults |
| 2020 | Setting up a Successful Diabetes Program 1.5 CEs Standard 5 | Facilitating Behavior Change |
| 2020 | Microvascular Complications, Eye, Kidney Nerve Disease 1.5 CEs | Standards 11- Micro Complications |
| 2020 | Women |Diabetes and Pregnancy 1.5 CEs Standards 14 | Management of Diabetes in Pregnancy |
| 2020 | Hospital and Hyperglycemia 1.5 CEs Standard 15 | Diabetes Care in Hospital |
| 2020 | Tots to Teens – Diabetes Standards 1.5 CEs Standard 13 | Children and Adolescents |
| 2020 | Hyperglycemia, Heart & Vessel Disease 1.5 CEs Standards 10 | CV Disease and Risk Management |

This is our last post of 2020! We want to thank all of you for your support and participation in our Question and Rationale of the Week! We will see you in 2021 with more exciting questions and rationales. Can’t wait!
Our December 22nd Question asked how to best treat a blood pressure of 162/94 according to ADA Standards of Care. Less than half of respondents, chose the best answer.
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer below: Answer Question
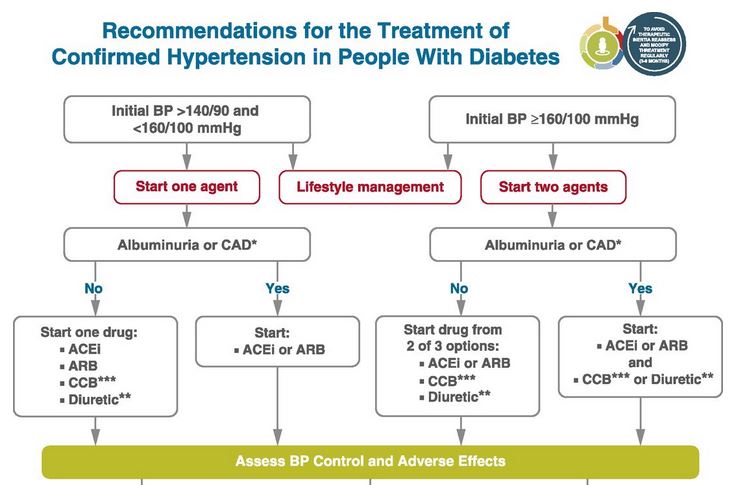
Question: JR is 63, has diabetes, and has a B/P of 162/94 which is repeated on a separate visit. JR also has albuminuria. What would be the recommended pharmacological approach based on the ADA Standards of Care?
Answer Choices:
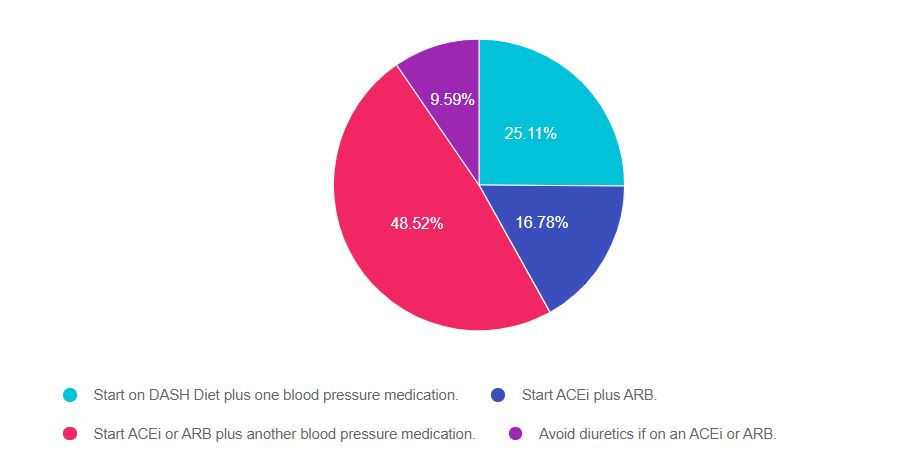
As shown above, the most common choice was option 3, the second most common answer was option 1, then option 2, and finally option 4.
If you are thinking about taking the certification exam, the content of this practice test question will set you up for success. Being familiar with the ADA Standards of Care is critical to pass either the CDCES or BC-ADM exam. The section of CV risk management is especially important, since the leading cause of death in diabetes is heart disease.
Answer 1 is incorrect. 25.11% chose this answer. “Start on DASH Diet plus one blood pressure medication.” Starting this person on the DASH meal plan along with a BP medication are both correct, however, given the extreme hypertension, more action is required.
Answer 2 is incorrect. 16.78% of you chose this answer. “Start ACEi plus ARB.” According to the ADA Standards, it is not recommended to use both of these agents together. The standards recommend to use EITHER an ACEi or ARB plus another blood pressure agent (diuretic, Calcium Channel Blocker, etc) to treat hypertension (see image below).
Answer 3 is correct, 48.52% of you chose this answer “Start ACEi or ARB plus another blood pressure medication.” According to ADA Standards (see image below), a confirmed BP where either the systolic is 160 or greater and the diastolic is 100 or greater, requires the initiation of 2 anti-hypertensive medications. Of course, we would request home blood pressure monitoring, review symptoms of orthostatic hypotension, and encourage lifestyle interventions.
Diabetes specialists have a tremendous opportunity to reduce CV events by being familiar with the standards and advocating on behalf of our clients for needed interventions.
Answer 4 is incorrect, 9.59% of you chose this answer. “Avoid diuretics if on an ACEi or ARB.” ADA standards include adding a diuretic to an ACEi or ARB if blood pressure is not at target (see image below).
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
This series is designed for health care professionals who are interested in getting started in diabetes education and for those actively working toward becoming a Certified Diabetes Care and Education Specialist. Each course in this series provides the critical building blocks and foundation for those entering the diabetes field. Plus, they prepare you to advance to our Level 2 Standards of Care Intensive Courses.
Join us for our 2021 Live Webinar Updates. All courses air at 11:30 a.m. (PST)

Instructor: Beverly Thomassian RN, MPH, CDCES, has been Board Certified in Advanced Diabetes Management for over 20 years. She is an Associate Clinical Professor at UCSF and Touro University and a nationally recognized diabetes expert.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]
Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.

Our December 15th Question of the week was tricky and over 59% of respondents, chose the best answer.
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer below: Answer Question
Question: JL is a 78-year-old with type 2 diabetes who has been taking metformin 1000mg BID for the past year. JL checks BG each morning and says it usually ranges from 100 – 138. Her most recent A1c came back at 9.6% and the provider started her on dapagliflozin (Farxiga) 5 mg daily two days ago. JL arrives at the clinic in a panic and says has been checking her blood glucose 3 times a day it has “jumped up to 236 and 242”. The diabetes specialist double-checked and verified random glucose of 249. What is the best explanation?
Answer Choices:

As shown above, the most common choice was option 3, the second most common answer was option 2, then option 1, and finally option 4.
If you are thinking about taking the certification exam, the content of this practice test question will set you up for success. This question lures test takers into trying to make an answer fit. Get rid of wrong answers first and choose the best answer.
Answer 1 is incorrect. 15.53% chose this answer. “Dapagliflozin is associated with transient hyperglycemia.” Dapagliflozin (Farxiga) is a SGLT-2 Inhibitor, also known as a “glucoretic”. It causes excretion of glucose from the renal tubules and is not associated with transient hyperglycemia. As a matter of fact, no diabetes medications cause hyperglycemia.
Answer 2 is incorrect. 17.54% of you chose this answer. “Double-check kidney function to verify GFR is adequate.” It is true that people need to have a GFR of 45 or greater to take Dapagliflozin (Farxiga). However, an inadequate GFR is not associated with glucose spikes. Also, the test question gives no data on GFR, so this makes this a very unlikely best answer.
Answer 3 is correct, 59.44% of you chose this answer “Discovery of hyperglycemia due to random BG checks.” Here are the Diabetes Specialist’s notes regarding JL.
JL stopped by the office today worried about sudden blood sugar elevations of 273 in 284 after starting a new medication on Friday for diabetes.
Dr. started JL on Dapagliflozin (Farxiga) half pill once a day and the patient has been taking it for two days now. JL is nervous about continuing to take it because JL thinks that is causing her blood sugars to elevate. The patient also takes metformin daily.
Before, the patient was only checking her blood sugar once a day and it was always in the morning. Her morning blood sugars were in the 120- 140 range. However, now JL is checking her blood sugars throughout the day and discovered that blood sugars are actually much higher than JL thought because was only checking in the morning. In the office I checked blood sugar it was 251. JL denied fever or cough.
Reassured JL that it was not the Dapagliflozin (Farxiga) causing high blood sugar. Focused on the benefits of Dapagliflozin (Farxiga) including lower blood sugar, lower blood pressure and protection against heart and kidney disease. Reviewed briefly the importance of limiting carbohydrates and juices or sodas until we can get her blood sugars closer to target.
Answer 4 is incorrect, 7.50% of you chose this answer. “Hyperglycemia due to the initiation of steroid therapy.” This is another juicy answer, but since the question doesn’t mention JL is on steroids, this is not the best answer.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
This series is designed for health care professionals who are interested in getting started in diabetes education and for those actively working toward becoming a Certified Diabetes Care and Education Specialist. Each course in this series provides the critical building blocks and foundation for those entering the diabetes field. Plus, they prepare you to advance to our Level 2 Standards of Care Intensive Courses.
Join us for our 2021 Live Webinar Updates. All courses air at 11:30 a.m. (PST)
Instructor: Beverly Thomassian RN, MPH, CDCES, has been Board Certified in Advanced Diabetes Management for over 20 years. She is an Associate Clinical Professor at UCSF and Touro University and a nationally recognized diabetes expert.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]
Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
JZ is excited for 2021 and wants to work on some New Years resolutions. Which of the following would be considered a SMART behavioral goal for the New Year?
Click here to test your knowledge!
This series is designed for health care professionals who are interested in getting started in diabetes education and for those actively working toward becoming a Certified Diabetes Care and Education Specialist. Each course in this series provides the critical building blocks and foundation for those entering the diabetes field. Plus, they prepare you to advance to our Level 2 Standards of Care Intensive Courses.
Join us for our 2021 Live Webinar Updates. All courses air at 11:30 a.m. (PST)
Instructor: Beverly Thomassian RN, MPH, CDCES, has been Board Certified in Advanced Diabetes Management for over 20 years. She is an Associate Clinical Professor at UCSF and Touro University and a nationally recognized diabetes expert.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]
Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
The Winter Solstice, on December 21, marked the shortest day in the Northern Hemisphere. People in New York got just over 9 hours 15 minutes of sun, while those in Anchorage Alaska got fewer than 5.5 hours.

Lack of light can contribute to depression. The idea that people are more susceptible to depression in the winter months wasn’t picked up until the 1980’s when South African psychiatrist Norman Rosenthal moved to the US and noticed a change in his mood during the New York winters. Dr. Rosenthal, Dr. Al Lewy, and Dr. Thomas Wehr investigated and identified Seasonal Affective Disorder (SAD). In 1987 it was included in DSM.(1)
This winter 2020 is an extra dark one. A recent study showed that depression symptom prevalence was more than 3-fold higher during the COVID-19 pandemic than before. During the pandemic, many people are making a lower-income or have no income, have depleted their savings, and have more exposure to stressors, which were all associated with a greater risk of depression. (2)
Studies show that people with diabetes are more susceptible to depression. Depression is three times as prevalent in people with diabetes when assessed by self-report. The combination of diabetes and depression present a major clinical challenge as the outcomes of both conditions are worsened in the presence of the other. Quality of life is worse, diabetes self-management is impaired, the incidence of complications is increased, and life expectancy is reduced. (3)
Refer to mental health providers as needed. As I am writing this blog my sister texted me that she is feeling very sad, unmotivated, and just wants to sleep. Diabetes Education Services has resources to help us screen our clients for depression in the Psychological Care Assessment Resource Page.
Can food, in particular a golden spice, help those of us without the more serious clinical depression cope this winter with milder winter blues?
Turmeric is a plant with a very long history of medicinal use, dating back 4000 years. In parts of Southeast Asia, turmeric is used not only as a principal spice but also as a component in religious ceremonies.
Turmeric, derived from the root of Curcuma longa, a flowering plant of the ginger family, is a gold-colored spice commonly used in the Indian subcontinent, not only for health care but also for the preservation of food and as a yellow dye for textiles. Curcumin, which gives the yellow color to turmeric, was first isolated almost two centuries ago, and its structure as diferuloylmethane was determined in 1910.
Since the time of Ayurveda (1900 BCE) numerous therapeutic activities have been assigned to turmeric for a wide variety of diseases and conditions. Extensive research within the last half-century has proven that most of these activities, once associated with turmeric, are due to curcumin. Curcumin has been shown to exhibit antioxidant, anti-inflammatory, antiviral, antibacterial, antifungal, and anticancer activities. (4)
“Curcumin can influence several mechanisms in the body; in particular, it is a powerful natural anti-inflammatory and antioxidant. This has relevance to depression because people with depression have greater inflammation and oxidative stress, which can affect all major organs of the body, including the brain”, reports Adrian Lopresti, PhD., a clinical psychologist and researcher at the School of Psychology and Exercise Science at Murdoch University. (5)
Due to curcumin’s anti-inflammatory effect, a 2013 review of studies suggests that curcumin can decrease the level of glucose in the blood, as well as other diabetes-related complications. (6) 500-1000 mg of curcumin per day has been found to promote the anti-inflammatory effect. (7) 1 teaspoon of fresh turmeric has about 200 mg of curcuminoids. Curcumin’s bioavailability can be enhanced by 2000% by combining it with black pepper (piperine is the major active component). (8)
Try turmeric tea or add turmeric to scrambled eggs, to rice as it is cooking, to stews. You can also try my favorite before bed treat, Golden Milk.

Directions
Simply pour all ingredients into a small saucepan, whisk to combine ingredients. Heat until hot to the touch but not boiling – about 4 minutes. Enjoy warm.
Written by Dawn DeSoto RD, CDCES, our resident Nutrition Content Writer
References

We are updating this course to reflect the 2021 ADA Standards of Care. This presentation will include the latest information on Social Determinants of health, assessment strategies and approaches. We will explore the psychosocial issues that can discourage individuals from adopting healthier behaviors and provides strategies to identify and overcome these barriers.
Life studies are used to apply theory to real life situations. A great course for anyone in the field of diabetes education or for those looking for a new perspective on assessment and coping strategies.
Topics include:
This course is included in: Level 2 – Standards of Care Intensive. Purchase this course individually for $29 or the entire bundle and save 70%.
Enroll in our entire Level 2 – Standards of Care Intensive to join us for the below for Live Webinar Updates. All courses air at 11:30 a.m. (PST)
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
JR is 63, has diabetes and has a B/P of 162/94 which is repeated on a separate visit. JR also has albuminuria. What would be the recommended pharmacological approach based on the ADA Standards of Care?
Click here to test your knowledge!
This series is designed for health care professionals who are interested in getting started in diabetes education and for those actively working toward becoming a Certified Diabetes Care and Education Specialist. Each course in this series provides the critical building blocks and foundation for those entering the diabetes field. Plus, they prepare you to advance to our Level 2 Standards of Care Intensive Courses.
Join us for our 2021 Live Webinar Updates. All courses air at 11:30 a.m. (PST)
Instructor: Beverly Thomassian RN, MPH, CDCES, has been Board Certified in Advanced Diabetes Management for over 20 years. She is an Associate Clinical Professor at UCSF and Touro University and a nationally recognized diabetes expert.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]
Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.

Today, is Winter Solstice, when we experience the shortest day and longest night of the year. From here we will slowly gain more light each day, marking this as an astronomical shift from darkness to light.
For many cultures, winter solstice marks a day of rebirth, saying goodbye to the past year and a universal deep breath for the future.
Susan Cooper penned a beautiful poem about winter solstice that we are thrilled to share with you below. Given this incredibly difficult year, it seems especially poignant and I hope you enjoy the read.
As a special bonus this year, Jupiter and Saturn will align in the night sky today, December 21st, in an event astronomers call the “great conjunction.”
The last time Jupiter and Saturn came this close was 1623, but that conjunction was too near the sun to be seen by Earthlings. 1226 is actually the most recent time such close conjunction of Jupiter and Saturn was visible to humans.
You can watch it online with webcasts from The Virtual Telescope Project, Slooh at NASA Telescope here.
And so the Shortest Day came and the year died
And everywhere down the centuries of the snow-white world
Came people singing, dancing
To drive the dark away
They lighted candles in the winter trees
They hung their homes with evergreen
They burned beseeching fires all night long
To keep the year alive
And when the new year’s sunshine blazed awake
They shouted, reveling
Through all the frosty ages you can hear them
Echoing behind us—listen!
All the long echoes, sing the same delight
This Shortest Day
As promise wakens in the sleeping land:
They carol, feast, give thanks
And dearly love their friends
And hope for peace.
And now so do we, here, now,
This year and every year.
Welcome, Yule!
This poem is available as a children’s hardcover with beautiful watercolor illustrations by Carson Ellis.