Subscribe
eNewsletter
Ready to get certified?
Free CDCES Coach App
eNewsletter
Free CDCES Coach App
Free Med Pocket Cards

The fourth trimester describes the time from delivery through the first 12 weeks postpartum. During this phase, attention often shifts to the newborn. However, for those who experienced gestational diabetes mellitus (GDM), engaging with their health care team can set the stage for long-term health and well-being.
Although only about 10% of individuals are affected by GDM, their risk of developing type 2 diabetes increases tenfold after delivery¹. Despite this heightened risk, studies ²,³ demonstrate that postpartum follow-up remains suboptimal. Comprehensive postpartum care planning started before delivery supports physical and psychological health for the long run
Individuals with GDM usually transition off diabetes medications in the postpartum period ¹; however, it is important to ensure appropriate medication care plans are in place based on the individual’s need. As prior existing pre-diabetes or diabetes may be found in up to one-third ² of individuals during this stage, both the American Diabetes Association and ACOG recommend oral glucose tolerance testing (OGTT) using pre-pregnancy criteria at 4-12 weeks 3 after delivery. OGTT is recommended instead of A1c testing, within the first 12 weeks postpartum, because of changes in blood volume, blood loss during delivery, and the rapid glycemic variations after birth.
However, we know barriers follow-up care and screenings exist. One health system’s retrospective study ¹ showed that while most women receive care from an OB-GYN after delivery, only 29% completed the recommended blood glucose screening. Among those
with abnormal results, just 11% were prescribed glucose-lowering medications, and 21% received a referral for diabetes risk reduction. This study is not unique ¹,² in its findings, and it highlights the need for proactive outreach and post-delivery care.
Ongoing and additional screenings are recommended due to increased cardiometabolic health risks. If postpartum OGTT results are found normal, repeat pre-diabetes and diabetes screening is recommended at least every 1-3 years. ¹ Home blood pressure monitoring is recommended for individuals with history of hypertension. Checking a lipid panel within the first year postpartum for assessment of ASCVD risk, however lipid levels may take up to 3 months to return to pre-pregnancy levels and should not be performed before 6 weeks postpartum due to pregnancy-related changes in lipid metabolism. Routine screening for post-partum depression is also recommended, given the higher prevalence of depression symptoms during and post-GDM, impacting self-care and metabolic outcomes.
In addition to early screening, intervention strategies require a multidisciplinary approach focusing on recovery, prevention, and empowerment. Coordination between OB-GYN, primary care, diabetes care teams, and pediatric groups ensures continuity of care. Education on lifestyle and behavioral health management should be delivered with empathy and flexibility, recognizing the competing demands of new motherhood. A Diabetes Prevention Program subgroup analysis of women who received lifestyle
interventions 10 years after GDM found a 50% decreased incidence of development of diabetes, and a more recent meta-analysis 5 found lifestyle interventions reduced the incidence of diabetes by 24%. Interventions with a registered dietitian can support lactation, restore nutrient balance, and promote cardiometabolic risk reduction.
Encouraging a gradual return to physical activity, beginning with gentle movement and progressing to regular moderate exercise, is associated with improved insulin sensitivity, diabetes risk reduction, and enhanced mood. Incorporating lactation consultants into postpartum care supports ACOG recommendations for exclusive breastfeeding the first 6 months of life and continued up to 2 years of age with solid foods transition. Though challenges such as delayed milk production and reduced supply may occur 6 due to the history of insulin resistance, breastfeeding offers many health benefits and significantly lowers the risk of developing type 2 diabetes for both mother and child. 4 Finally, establishing a clear transition plan to primary care that promotes annual visits, family planning, and ongoing lifestyle support may enhance long-term health maintenance.
Flexible care delivery models that meet women where they are in this stage of life may further help overcome barriers and reduce disparities in postpartum follow-up.
The fourth trimester represents a pivotal opportunity to ensure postpartum care and support to engage lifelong health. This time often shifts focus to the newborn, but for women with a history of GDM, this period is not only about recovery but also prevention of type 2 diabetes, cardiovascular disease, and future pregnancy complications. The diabetes care team can support postpartum screenings, nutrition, lifestyle interventions, and transition of care that close postpartum care gaps. Proactively outreaching and engaging during this critical phase can connect individuals to resources and long-term chronic disease prevention.
Christine Craig, MS, RDN, CDCES
Founder: Nutrition for Daily Living
References:

Are you a healthcare professional providing diabetes care in an under-resourced community? Are you working toward earning your certification in diabetes education (CDCES or BC-ADM?)
If yes, please consider applying for our Bridge Scholarship, which covers the registration cost for the DiabetesEd Training Conference in San Diego, Oct 22-23, 2026 (value of $559). This program will provide you with the content needed to prepare for mastery-level diabetes certification and beyond!
Recipients will be awarded the Training Conference reg fee, including the live program, printed syllabus, 30+ CE’s, plus access to the online bonus courses for one year! Applications Due on July 20th, 2026

🌟Updated Schedule: ADA Boot Camp, Tech, MNT & More
Live in Beautiful San Diego – Oct 22-23, 2026
Re-Ignite your Passion & Prepare for Diabetes Certification Exams
🎓 Earn 30+ CEs: AMA PRA Category 1 Credits™, ACPE, ANCC, and CDR!
📅
2-Day Conference
Oct 22–23, 2026
⏱️
15.5 Live CEs
+ 17 bonus CEs
🏅
CDCES & BC-ADM
Exam Prep + Renewal
📍
San Diego, CA
1.7 mi from airport
The field of diabetes care is expanding and evolving rapidly. This unique training conference will keep you on the cutting edge plus prepare you for certification exams. It also fulfills the Standards of Care renewal requirement. Join us for two days of intensive education that is fun and inspiring. Add on the optional Day 3 (Engaging the Disengaged), to complete your conference exeperience.
Coach Beverly and Diana Isaacs, PharmD, BC-ADM, CDCES co-lead an exciting day that brings the ADA and AACE Standards to life. Gain fresh insights, practical tools, and a deeper understanding of the latest in person-centered diabetes care. After attending, you will be empowered to share the latest in diabetes care with your colleagues and the people in your care.
Take your knowledge to the next level with this intensive deep-dive into insulin therapy, dosing and pattern management with Dr. Diana Isaacs. Next, stay for the diabetes tech show-and-tell as Diana demonstrates the specs of the latest pumps and sensors. After lunch, nutrition whiz Christine Craig, MS, RDN, CDCES expertly details the latest in MNT and provides real strategies on translating this content to your clinical practice. You will have a chance to put it all together as Coach Beverly leads you through a series of case studies that integrates content from Day 1 and Day 2.
On Saturday, join this exceptional day-long program led by William H. Polonsky, PhD, CDCES & Susan Guzman, PhD (Behavioral Diabetes Institute) that reveals psychosocial forces behind diabetes self-management — tools to break through resistance and inspire change.
Read more below
📜 Essentials
Registration
+ Printed Syllabus
$559.00
🌟 Deluxe
Essentials
+ ADA Standards Book
$589.00
🏆 Complete – Best Value!
Deluxe
+ ADCES Review Guide e-Book
$669.00

Transform how you engage patients with diabetes — master behavior change, reduce distress, and overcome medication hesitancy.
Why do so many patients know what they should do — but still struggle to do it?
The answer lies in the psychology of diabetes.
In this transformative full-day course, world-renowned experts William H. Polonsky, PhD, CDCES, and Susan Guzman, PhD, from the Behavioral Diabetes Institute reveal the hidden psychosocial forces that drive — or derail — diabetes self-management.
You’ll walk away with a completely new toolkit for breaking through patient resistance, dissolving medication hesitancy, and creating clinical encounters that actually inspire change!

JR was recently diagnosed with type 2 diabetes, but based on their history of pancreatitis, you suspect JR actually has Diabetes Type 3c.
Which of the following symptoms match a diagnosis of Diabetes Type 3c?

Explore the magnificent world of diabetes and the gut — from periodontal disease to the microbiome and everything in between.
Join Coach Beverly Thomassian, RN, MPH, CDCES, BC-ADM, for a fascinating journey through gastrointestinal health from top to bottom. This course covers fatty liver disease, gastroparesis, intestinal complications of diabetes, the gut microbiome, and more — giving you the knowledge to better support whole-body health.
Featured Articles ___________________________ |
Upcoming Programs ___________________________ Upcoming FREE Webinars ___________________________ |
Greetings, wonderful healthcare colleagues!
Did you know that over 16% of American adults—nearly 1 in 6—are living with diabetes, according to the latest data from the CDC? When we look at the bigger picture, it becomes clear that social drivers of health play a decisive role in this growing epidemic.
Data suggests that access to knowledge, resources, and supportive environments can profoundly impact prevention, diagnosis, and daily diabetes management. By equipping individuals with knowledge about diabetes management and preventative measures, we empower them to take ownership of their health and inspire change within their communities.
To get the ball rolling, we are excited to share a list of our favorite FREE diabetes resources in English and Spanish. Please share this information with your colleagues and community members.
Have you considered the implications of Stage 4 Gestational Diabetes (GDM)? As Christine Craig highlights, after the birth of a baby, it is challenging to keep follow-up appointments and receive ongoing healthcare. Yet after delivery with GDM, the risk of future diabetes is high, and staying connected with the care team improves outcomes. Read more about this critical 4th Stage.
Our tech expert, Dr. Sarah, considers the impact of technology on diabetes distress. What effect does being “plugged” into technology have on the emotional health of the person living with diabetes?
Lastly, to help everyone feel their best this holiday season, we are sharing our popular handout, “Ten Strategies to Survive the Holidays” as well as an info sheet on reframing diabetes distress.
We hope you can join our FREE webinars celebrating National Diabetes Month. We sincerely appreciate your ongoing dedication to improving diabetes care.
With gratitude for the care you give every day!
Coach Beverly, Bryanna, Astraea & Katarina
For last week’s practice question, we quizzed participants on RT forgetting their insulin, and what would be the best response. 63.10% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question

RT has type two diabetes and has been maintaining a time and range of 70% or greater. However, when they show up at the office, the last week’s time in range dropped to 30%. You ask what was different this week from the previous few months. RT tells you they went on a five day fishing trip and forgot their insulin.
What’s the best response?
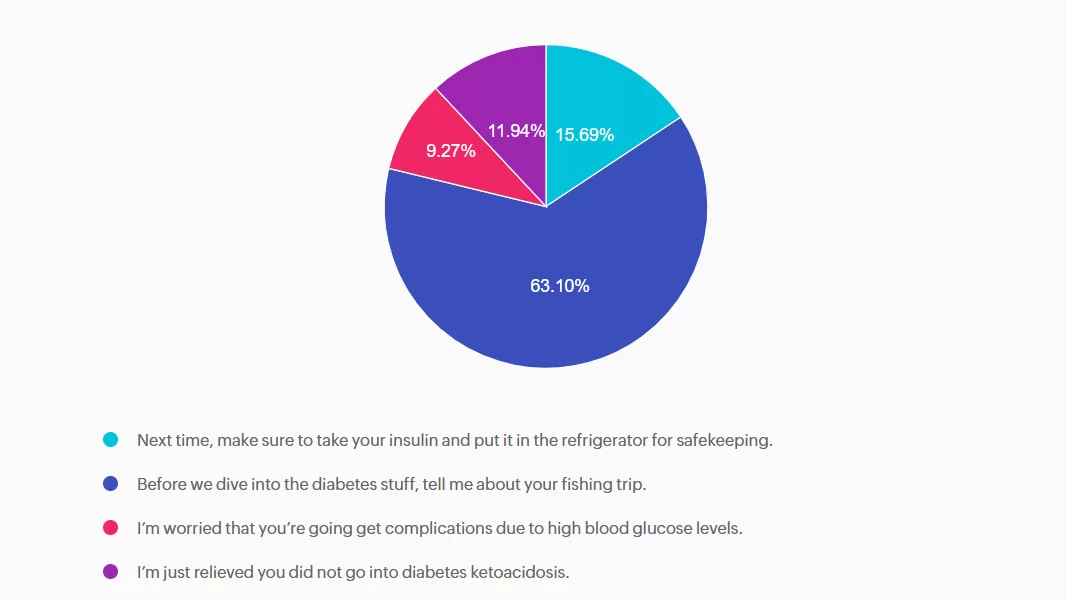
Answer A is incorrect: 15.69% chose this answer, “Next time, make sure to take your insulin and put it in the refrigerator for safekeeping.” This approach goes under the compliance model, where the healthcare professional only provides one way instruction without considering the individuals insights and problem solving skills. We want to work toward a person-centered collaborative approach to foster connection.
Answer B is correct: 63.10% chose this answer, “Before we dive into the diabetes stuff, tell me about your fishing trip.” Great job! This is the best answer. By asking RT about their fishing trip first, you let them know you are interested in their life experiences and this helps to establish a connection. After hearing about the trip, we might pivot and say something like, “Do you want to discuss strategies to bring your insulin on your next fishing trip?”
Answer C is incorrect: 9.27% chose this answer, “I’m worried that you’re going get complications due to high blood glucose levels.” Although this statement shows concern, it is unlikely that RT will get diabetes complications from not taking their insulin for a few days. This statement could lead to feelings of shame and failure, and may close the door to making a meaningful connection.
Answer D is incorrect: 11.94% chose this answer, “I’m just relieved you did not go into diabetes ketoacidosis.” This statement could evoke feelings of guilt and shame, that could close the door to future communication. And if RT has type 2 diabetes, the chance of DKA is minimal. Instead of focusing on the HCP feelings, let’s check in with RT and explore problem solving strategies for future trips that would work for them.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!

According to the latest CDC Data, over 16% of Americans are living with diabetes and 38% have prediabetes. This means about half of our communities are living with hyperglycemia.
Advocacy and education play essential roles in diabetes care and prevention. By equipping individuals with knowledge about diabetes management, healthy lifestyle choices, and preventative measures, we empower them to take ownership of their health and inspire change within their communities.
Community-centered education can be incredibly powerful—when people feel informed and supported, they’re more likely to make meaningful changes and encourage others to do the same. This creates a ripple effect, fostering healthier communities and potentially reducing the prevalence of diabetes over time.
Wear blue: Wear blue on World Diabetes Day (November 14th) and throughout the month. You can also display a blue circle symbol in your window.
Participate in events: Join a Global Diabetes Walk or create your own. Support local chapter events hosted by organizations like the American Diabetes Association or Breakthrough T1D.
Host an event: Organize a fundraising event like a farm fresh sale or car wash, or host an educational session like a “Lunch and Learn” with a local expert.
Spread the word: Share educational content, personal stories, and facts about diabetes on social media, You can also share information via email or newsletters.
Post the Diabetes Risk test: Post the American Diabetes Association Risk Test (see below) in your organization’s or community’s newsletter.
We have put together a list of FREE Webinars and diabetes resources in English and Spanish to share with people living with prediabetes and diabetes. Thank you for your advocacy and belief that we can make a difference.
ADA’s Diabetes Food Hub – English and Spanish! Web site filled with information on healthy eating and an abundance of delicious recipes.
ADA Resources in Spanish – this newly opened information hub is perfect for those who prefer to learn and read in Spanish.
ADA’s FREE Life with Diabetes Program: ADA’s program includes six digital, printable journeys to teach how to live well with diabetes; a monthly e-newsletter with tips, stories, and more resources; six free issues of the Diabetes Forecast® magazine; access to an online community and local events. (The program is available in both English and Spanish).
ADA’s Risk Quiz: 60-second online risk assessment for type 2 diabetes. ADA created a self-assessment and a version to fill out the assessment for others. There’s also a printable version in English & Spanish that can be distributed to help ascertain risk. This is a great first step in helping individuals consider coming in for an appointment
CDC Diabetes Prevention Program Curricula and Handouts This site offers excellent resources for those interested in offering Diabetes Prevention Education in English and Spanish.
National Diabetes Education Program is an online library of resources compiled by the NDEP to help provide accurate information and support for people living with prediabetes and diabetes.
Spanish Language Resources: language can be a barrier to adequate and quality care. ADCES has created a number of free downloads for people with diabetes and prediabetes, which have been translated into Spanish.
Type 1 Diabetes Resource Page – Includes is a list of helpful online resources for Type 1 Diabetes. It include sites for national organizations like the American Diabetes Association (ADA), sites for diabetes interest groups, and other participant organizations that provide helpful diabetes tips and opportunities to join online groups.
Panther Diabetes Technology Deciphered. Get to the gist of what you need to know. Essential resources and guidance for health care professionals working with diabetes technology.
DiabetesWisePro for Clinicians A non-biased web site for health care professionals that has a quick tool to access insurance coverage information, how to order devices, what to include and where to go for support.
DiabetesWise A non-biased website that helps people with diabetes learn about different diabetes devices and determine the best match for their needs
Insulin Cost Savings Toolkit Resource Page – An ADCES complete listing of low cost insulin options and resources.
Technology Cost Savings Resource Page – An ADCES listing of websites and information to obtain pumps and sensors for a lower cost.
Cheat Sheets: We have assembled an abundance of helpful diabetes education cheat sheets for healthcare professionals and those living with diabetes. Feel free to print and share!
Join our special guest speaker, Nick Kundrat, and join the conversation!
Beyond Blood Glucose: Empowering Health Through a Holistic Lens
November 19th at 11:30 AM PST
MT is a 29-year-old with Type 1 diabetes who is currently 14 weeks pregnant. She uses a continuous glucose monitor (CGM) with concurrent fingersticks and uploads her glucose data weekly. Her CGM settings was already set to the recommended time in range and the latest CGM report shows the following: time in range (TIR): 67%, time below range: 6%, time above range: 27%.
Based on current ADA Standard of Care, which of the following statements is most accurate regarding her CGM values?
Level 5 | Beyond Blood Glucose: Empowering Health Through a Holistic Lens with:
Speaker Nick Kundrat, BS, CEP, CDCES, LMT

Use the code Cyber30 for 30% off at checkout!
For last week’s practice question, we quizzed participants on Diabetes Tech and Diabetes Distress. 99.36% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Kyle is a 55-year-old man with type 2 diabetes for ten years. He was recently diagnosed with retinopathy in both eyes. His grandmother lost her eyesight due to diabetes. Due to this family history, he is very concerned about his new diagnosis. He uses a Libre continuous glucose monitor (CGM) to monitor his blood sugar levels. During your visit, he is preoccupied with checking his Libre CGM and tells you that he uses his glucometer to verify CGM readings at least four to six times per day. When you ask him about this, he reports that he can’t focus on his work or home life if he isn’t over 90% time in range.
As a diabetes care and education specialist, what is the best approach to this situation?
Answer A is incorrect: 0% chose this answer, “Reassure Kyle that retinopathy is very common with type 2 diabetes. Encourage him to verify the CGM with his glucometer more frequently if that helps make him feel less anxious.” This is incorrect. Although diabetes retinopathy is a common complication of diabetes, it is not inevitable, and the risk can be reduced by maintaining optimal glycemic control. Additionally, verifying blood glucose levels with a glucometer when there appears to be no issue with his CGM will not alleviate his anxiety.
Answer B is incorrect: 0% chose this answer, “Educate Kyle that the CGM he is using cannot be calibrated and instruct him to stop using his glucometer, since the CGM is accurate.” This is incorrect. Though his particular CGM cannot be calibrated, fingerstick blood glucose readings are the gold standard when CGM readings are unexpectedly out of range.
Answer C is correct: 99.36% chose this answer, “Acknowledge Kyle’s fears about vision loss, screen for diabetes distress, and collaborate on strategies to reduce the emotional burden of CGM use, including referral to a behavioral health provider if indicated.” This is correct. Kyle is demonstrating symptoms of diabetes distress due to fear of ocular complications, perfectionism, and technology overwhelm. The ADA Standards of Care 2025 recommend routine screening for diabetes distress and other psychosocial concerns at least annually or when complications arise.
Answer D is incorrect: 0.64% chose this answer, “Adjust Kyle’s time in range target goal to >90% to meet his expectations and reduce his worry about complications.” This is incorrect: The time in range goal for most adults living with diabetes is >70%. Adjusting his time-in-range goal to >90% will not work to reduce his obsessive behavior.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!

Get 30% Off Your Entire Order!
From November 30th to December 2nd, use the code “Cyber30″ for 30% off at checkout!
Save the date and shop our sale

The American Diabetes Association estimates that over 8 million people in the United States depend on insulin therapy for survival.¹ Multiple daily injections (MDI) of insulin can be challenging to manage. Diabetes care and education specialists understand that complex medication regimens often lead to difficulty achieving medication adherence and worsening glycemic control.²
CeQur Simplicity is a unique alternative to MDI therapy. It redefines insulin delivery with a wearable device that administers insulin with just a few clicks. By simplifying insulin delivery, CeQur can support successful insulin management and improve glycemic control without the hassle of multiple daily injections.
The CeQur Simplicity patch is a wearable insulin delivery device for adults aged 21 and older, approved for individuals with type 1 or type 2 diabetes who require insulin. This thin patch can hold up to 200 units of either U-100 lispro (Humalog) or U-100 aspart (Novolog) insulin. The patch can be used for up to 4 days on any approved insulin injection site. It is usually worn on the abdomen, thigh, or upper arms, as these areas are more accessible for reaching the CeQur device.³
Pressing the buttons on the sides of the device delivers two units of insulin. Each press produces an audible click to announce delivery. Over the 4-day wear period, this wearable insulin device replaces up to twelve meal bolus injections. The ease of use and ability to dose without carrying and storing insulin or injecting it can be freeing for many people living with diabetes. Research has found that when using the CeQur patch, users were more satisfied with the device, experienced less diabetes-related burden, and missed fewer insulin boluses.
CeQur is not an automated insulin delivery system. This device operates independently and does not connect to continuous glucose monitors. The CeQur Simplicity is not approved for basal insulin and does not replace the need for basal insulin.
Diabetes healthcare professionals can help identify clients who may benefit from the CeQur Simplicity insulin patch. An ideal CeQur candidate may be those who:
The healthcare professional’s (HCP) role starts with explaining the CeQur Simplicity device and how it differs from traditional insulin pumps and insulin pens. Besides identifying those who may benefit from CeQur, the HCP also provides training and troubleshooting for CeQur. CeQur training includes demonstrating how to apply and remove the device, using the click-based bolus feature, and performing site care and rotation procedures. This hands-on education helps clients build confidence in their new insulin delivery device. HCP’s can also assist in exploring cost, insurance coverage, and manufacturer support programs.
Here are other considerations for the diabetes healthcare professional:
✅ Assess the ability to count by 2s as the device only delivers doses in increments of 2 units.
✅ Fill the CeQur device with insulin just before use and never prefilled in advance.
✅ Do not apply a CeQur insulin patch near the area where basal insulin is injected.
✅ Avoid applying the insulin patch to areas that will be irritated by clothing, accessories, or a seat belt.
✅ Use the ‘Change By’ sticker provided with each device as a reminder of when the device needs to be changed.
✅ Avoid submerging the patch more than 3 feet 3 inches (1 meter). Also, do not squeeze the dosing buttons while the patch is underwater.³
Diabetes healthcare professionals work to identify and address barriers to insulin therapy. Collaborating with clients can boost their confidence, foster effective diabetes self-management, and improve their psychological outcomes. For those who are frustrated with their current MDI therapy but are also leery of AID systems, the CeQur Simplicity insulin patch may offer fewer injections, freedom from carting around meal-time insulin, and an improved quality of life.
References