
Subscribe
eNewsletter
Ready to get certified?
Free CDCES Coach App
eNewsletter
Free CDCES Coach App
Free Med Pocket Cards

Announcements ___________________________ |
Join us in celebrating National Nutrition Month and the registered dietitian nutritionists who help us maintain the pleasure of eating while empowering us to make informed decisions about daily food choices!
We are thrilled to highlight the significant impact RDNs have on individuals, communities, and society by promoting healthy eating habits, preventing disease, and improving our overall quality of life.
In this newsletter you will find three exciting articles by our expert guest dietitians, coupled with Questions of the Week.
First, Christine Craig provides valuable insights on how to manage diabetes during periods of religious or medical fasting. This is perfect timing since Ramadan is being observed through the end of March. Catch Christine live during our Virtual Conference in April.
Next, Jessica Jones provides insights and strategies to break through weight stigma and provide weight-inclusive nutrition counseling. You can join her live webinar on this topic on June 5th.
Lastly, Evgeniya Evans discusses a mindful eating approach that provides a compassionate, sustainable path to achieving balance and well-being. You can catch her live webinar on this topic, airing June 11th.
You can also download our updated Diabetes Apps Cheat Sheet and Pocket Card and test your knowledge with 3 nutrition Questions of the Week!
With an abundance of gratitude,
Coach Beverly, Bryanna, Tiffany, Christine, & Katarina
Gain fresh insights, practical tools, and a deeper understanding of the latest in person-centered diabetes care. Our expert team brings the ADA Standards of Care to life—covering medications, behavior change, technology, and more! If you’re preparing for the CDCES or BC-ADM exam, this conference—paired with free bonus courses—serves as the ideal study companion!
With interactive co-teaching, we keep sessions engaging, relevant, and fun. Let’s learn and grow together!

Our expert team transforms complex diabetes science into clear, practical insights—keeping it real, engaging, and fun! The faculty includes:
For last week’s practice question, we quizzed participants on ADA Standards & what is next med addition? 67% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question:
JR has type 2 diabetes and takes Metformin 1000mg BID and sitagliptin (Januvia), A1C 8.1%. GFR 47, UACR 158mg/g. Recent diagnosis of congestive heart failure. These are the medications their insurance covers.
Of the following medications, which addition would most benefit JR?
Answer Choices:
For a helpful reference, please see our PocketCards for more information.
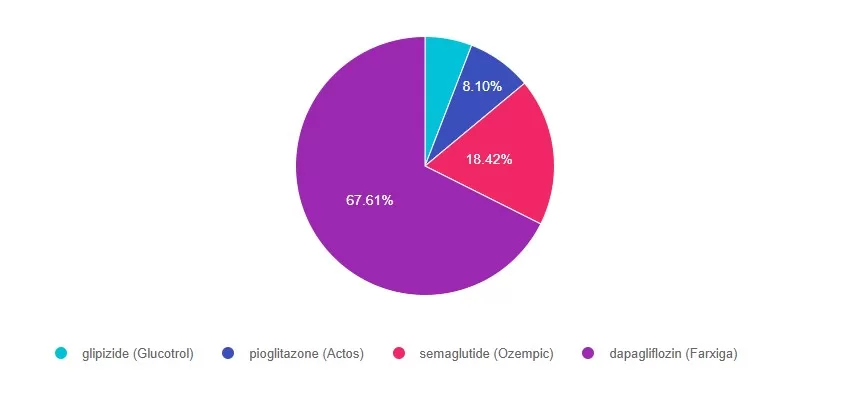
Answer 1 is incorrect. 5% chose this answer, “Glipizide (Glucotrol)”. Even though glipizide would help lower blood glucose, considering JL’s CHF and worsening kidney function, it is not the best choice.
Answer 2 is incorrect. 8% of you chose this answer, “pioglitazone (Actos)”. Even though pioglitazone would help lower blood glucose, considering JL’s CHF and worsening kidney function, it is not the best choice.
Answer 3 is incorrect. About 18% of respondents chose this, “Semaglutide (Ozempic)”. Even though semaglutide would help lower blood glucose and would address worsening kidney function, considering JL’s CHF and worsening kidney function, it is not the best choice.
Finally, Answer 4 is correct. 67% chose this answer, “Dapagliflozin (Farxiga)”. YES, GREAT JOB. Dapagliflozin is a SGLT-2i that will help lower blood glucose, address worsening kidney function and CHF. Plus, it is covered by insurance. Considering JL’s health profile, it is the best choice.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Gain fresh insights, practical tools, and a deeper understanding of the latest in person-centered diabetes care. Our expert team brings the ADA Standards of Care to life—covering medications, behavior change, technology, and more! If you’re preparing for the CDCES or BC-ADM exam, this conference—paired with free bonus courses—serves as the ideal study companion!
With interactive co-teaching, we keep sessions engaging, relevant, and fun. Let’s learn and grow together!

Our expert team transforms complex diabetes science into clear, practical insights—keeping it real, engaging, and fun! The faculty includes:
by Evgeniya Evans, MS, RDN, CDCES
Managing diabetes often involves making significant lifestyle and dietary adjustments, which can sometimes feel overwhelming or lead to feelings of deprivation. Research highlights that diabetes distress, experienced by 18–45% of individuals with diabetes, can negatively impact glycemic outcomes and medication adherence (Aikens, 2012; Nicolucci et al., 2013). Successful diabetes management, however, requires more than adherence to rules—it calls for a lifestyle change. For meaningful, lasting effects, individuals can find joy and purpose in their efforts, making new lifestyles not only healthy but also enjoyable (Fredrickson, 2004; Garland et al., 2010). Mindful eating offers a compassionate and sustainable pathway to achieving this balance

Mindful eating shifts the focus from what to eat to how to eat. It invites individuals to bring awareness, curiosity, and intention to their eating habits and bodily sensations. Rooted in mindfulness principles, this practice involves paying purposeful, nonjudgmental attention to the present moment during meals (Kabat-Zinn, 2009). By slowing down and tuning into internal cues like hunger and fullness, individuals can foster sustainable behavior changes that go beyond traditional diet approaches (Framson et al., 2009; Nelson, 2017).
Unlike restrictive diets that focus on counting calories or carbs, mindful eating emphasizes sensory awareness and emotional well-being. This approach helps individuals become more attuned to their body’s needs, promoting a more positive relationship with food.

A growing body of research supports mindful eating’s effectiveness in improving various aspects of health. It enhances the connection between the body and food, helping to interrupt automatic or emotional eating patterns (Forman et al., 2016). In addition, mindful eating has been shown to reduce binge eating behaviors (Kristeller & Hallett, 1999; Mercado et al., 2021).
For individuals with diabetes, mindful eating can lead to significant benefits. Studies have demonstrated improvements in A1C levels, weight management, and reductions in depressive symptoms. It has also been linked to enhanced self-efficacy and improved dietary patterns (Miller et al., 2012; 2014). By promoting awareness and fostering emotional resilience, mindful eating can support better glycemic management and help reduce diabetes-related distress.

Mindful eating strategies fall into three broad categories:
Here is how it works:
Reflect on the Experience:
If you are looking for a fun way to explore mindful eating further, teach someone you know how to eat mindfully. Choose a simple food, such as a piece of fruit, a berry, nut, or a piece of chocolate, and guide them through the steps of sensory engagement. After the practice, reflect together on the experience, asking, what did you notice? How did it feel to eat this way?
This exercise often reveals that when we slow down and savor our food, we enjoy it more and may feel satisfied with smaller portions.

Mindful eating is more than a strategy; it is a mindset that transforms how we approach food, health, and self-care. For diabetes educators, integrating mindful eating can refresh and enhance their toolbox by creating a more compassionate, effective, and enjoyable path to better diabetes care.
Whether you are planning to use this practice professionally or personally, start small, explore the practice, and empower yourself and others to build a positive relationship with food, one mindful bite at a time.
by Evgenia Evans, MS, RDN, CDCES
Aikens, J. E. (2012). Prospective associations between emotional distress and poor outcomes in type 2 diabetes. Diabetes Care, 35(12), 2472–2478. https://doi.org/10.2337/dc12-0181
Forman, E. M., Shaw, J. A., Goldstein, S. P., Butryn, M. L., Martin, L. M., Meiran, N., Crosby, R. D., & Manasse, S. M. (2016). Mindful decision making and inhibitory control training as complementary means to decrease snack consumption. Appetite, 103, 176-183. https://doi.org/10.1016/j.appet.2016.04.014
Framson, C., Kristal, A. R., Schenk, J. M., Littman, A. J., Zeliadt, S., & Benitez, D. (2009). Development and validation of the Mindful Eating Questionnaire. Journal of the American Dietetic Association, 109(8), 1439–1444. https://doi.org/10.1016/j.jada.2009.05.006
Fredrickson, B. L. (2004). The broaden-and-build theory of positive emotions. Philosophical Transactions of the Royal Society of London. Series B, Biological Sciences, 359(1449), 1367–1377. https://doi.org/10.1098/rstb.2004.1512
Garland, E. L., Fredrickson, B. L., Kring, A. M., Johnson, D. P., Meyer, P. S., & Penn, D. L. (2010). Upward spirals of positive emotions counter downward spirals of negativity: Insights from the broaden-and-build theory and affective neuroscience on the treatment of emotion dysfunctions and deficits in psychopathology. Clinical Psychology Review, 30(7), 849–864. https://doi.org/10.1016/j.cpr.2010.03.002
Harvard T.H. Chan School of Public Health. (2024, November 7). Mindful Eating. The Nutrition Source. https://nutritionsource.hsph.harvard.edu/mindful-eating/
Kabat-Zinn, J. (2009). Full catastrophe living: Using the wisdom of your body and mind to face stress, pain, and illness. Random House Publishing Group.
Kristeller, J. L., & Hallett, C. B. (1999). An exploratory study of a meditation-based intervention for binge eating disorder. Journal of Health Psychology, 4(3), 357–363. https://doi.org/10.1177/135910539900400305
Kristeller, J. L., Wolever, R. Q., & Sheets, V. (2014). Mindfulness-based eating awareness training (MB-EAT) for binge eating: A randomized clinical trial. Mindfulness, 5(3), 282–297. https://doi.org/10.1007/s12671-012-0179-1
Mercado, C., Marasigan, K., Cardona, J., & Ko, E. (2021). Mindfulness-based interventions for emotional eating and binge eating in adults: A meta-analysis. Appetite, 164, 105265. https://doi.org/10.1016/j.appet.2021.105265
Miller, C. K. (2017). Mindful eating with diabetes. Diabetes Spectrum, 30(2), 89–94. https://doi.org/10.2337/ds16-0040
Miller, C. K., Kristeller, J. L., Headings, A., Nagaraja, H., & Miser, W. F. (2012). Comparative effectiveness of a mindful eating intervention to a diabetes self-management intervention among adults with type 2 diabetes: A pilot study. Journal of the Academy of Nutrition and Dietetics, 112(11), 1835–1842. https://doi.org/10.1016/j.jand.2012.07.036
Miller, C. K., Kristeller, J. L., Headings, A., & Nagaraja, H. (2014). Comparative effectiveness of a mindful eating intervention to a diabetes self-management intervention among adults with type 2 diabetes: A randomized controlled trial. Health Education & Behavior, 41(2), 145–154. https://doi.org/10.1177/1090198113493092
Nicolucci, A., Kovacs Burns, K., Holt, R. I. G., Comaschi, M., Hermanns, N., Ishii, H., Kokoszka, A., Pouwer, F., Skovlund, S. E., Stuckey, H., Tarkun, I., Vallis, M., Wens, J., & Peyrot, M. (2013). Diabetes Attitudes, Wishes and Needs second study (DAWN2™): Cross-national benchmarking of diabetes-related psychosocial outcomes for people with diabetes. Diabetic Medicine, 30(7), 767–777. https://doi.org/10.1111/dme.12245
Nelson, J. B. (2017). Mindful eating: The art of presence while you eat. Diabetes Spectrum, 30(3), 171–174. https://doi.org/10.2337/ds17-0015
Enroll in our upcoming webinar led by Evgeniya Evans, MS, RDN, CDCES
This engaging and practical webinar, developed by Evgeniya Evans, MS, RDN, CDCES, a positive psychology practitioner, is tailored explicitly for healthcare professionals including dietitians, diabetes care specialists, and providers.
Using evidence-based strategies, participants will gain a deeper understanding of the benefits of incorporating mindfulness into the eating experience, including enhanced glycemic management, improved emotional well-being, and healthier eating behaviors. The webinar includes an overview of mindfulness and mindful eating strategies, such as engaging all five senses, recognizing hunger cues, addressing cravings, and using practical tools to create supportive eating environments.

Participants will also learn how to adapt these approaches to diverse populations and the unique needs of individuals. Join us to deepen your expertise, participate in insightful discussions, and empower individuals to cultivate sustainable, positive relationships with food while achieving long-term health goals.
Course topics:

Evgeniya Evans, MAPP, RDN, LDN, CDCES, specializes in chronic disease prevention, diabetes management, and women’s health. Her unique approach integrates mindfulness-based nutrition and positive psychology, creating transformative impacts on her patients’ health and well-being.
Evgeniya’s academic journey reflects her dedication to lifelong learning and her holistic understanding of nutrition and health. She began with four years of Sociology studies at Omsk State University in Russia, followed by earning a Bachelor of Science in Nutrition and Dietetics from the University of Illinois Chicago. She furthered her expertise with a master’s degree in Applied Positive Psychology from the University of Pennsylvania. This diverse educational foundation allows her to address the socio-psychological factors that influence dietary behaviors and deliver a well-rounded approach to patient care.
At Cook County Health’s Diabetes Clinic within the Endocrinology Department, Evgeniya provides medically tailored nutrition therapy and culturally sensitive counseling. She works with individuals from various socio-economic backgrounds, guiding them through their unique health challenges with compassion and precision. Her dedication to creating personalized, sustainable dietary strategies highlights her commitment to promoting long-term health and vitality for her patients.
In addition to her clinical practice, Evgeniya is a passionate educator. She teaches several classes at her clinic, including Pillars of Diabetes Management with Lifestyle, Nutrition for Health and Vitality, and The Art of Mindful Eating. Her emphasis on education underscores her belief in the transformative power of fostering a healthy, enjoyable lifestyle supported by mindful eating and a positive mindset.
Evgeniya envisions a world where individuals are free from the struggles of dieting and food-related shame. She dreams of a future where no one feels deprecated by their appearance or food choices, and everyone enjoys the vitality and health to pursue their dreams. She is devoted to fostering vibrant, authentic lives where cooking, eating, and sharing meals with loved ones are sources of joy, love, and positive connection.
All hours earned count toward your CDCES Accreditation Information
JL observes Ramadan and fasts from sunrise to sunset. JL has type 2 diabetes and usually takes 4 units of bolus insulin three times a day with meals and 10 units of glargine (Rezvoglar) at bedtime.
What would be the best recommendation for JL?
Gain fresh insights, practical tools, and a deeper understanding of the latest in person-centered diabetes care. Our expert team brings the ADA Standards of Care to life—covering medications, behavior change, technology, and more! If you’re preparing for the CDCES or BC-ADM exam, this conference—paired with free bonus courses—serves as the ideal study companion!
With interactive co-teaching, we keep sessions engaging, relevant, and fun. Let’s learn and grow together!
Our expert team transforms complex diabetes science into clear, practical insights—keeping it real, engaging, and fun! The faculty includes:
Host a Local Event!
Use EarthDay.org’s event map to find or promote cleanups, workshops, or plantings in your area.
For last week’s practice question, we quizzed participants on what happens when people stop taking GLP /GIPs. 81% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question:
About 30% of people with diabetes started on GLP-1’s stop taking this medication before completing a year of therapy.
According to ADA Standards, what results from sudden discontinuation of GLP-1s /GIP like semaglutide and tirzepatide?
Answer Choices:
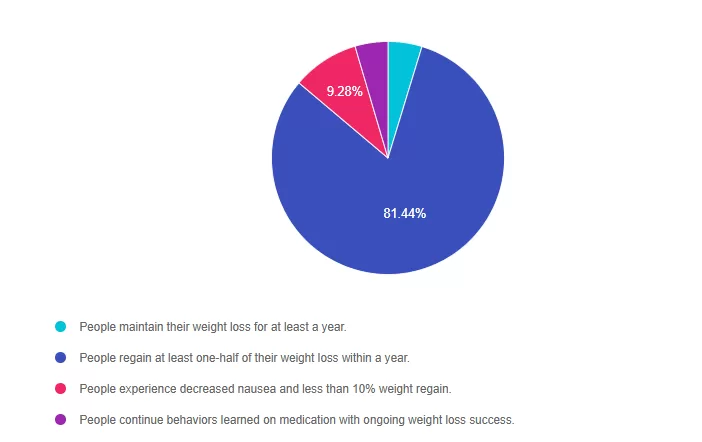
Answer 1 is incorrect. 4.71% chose this answer. “People maintain their weight loss for at least a year.” According to the ADA Standards, people regain 50 to 70% of the weight lost after this gut hormone replacement therapy is stopped.
Answer 2 is correct. 81.44% of you chose this answer. “People regain at least one-half of their weight loss within a year.” YES, this is the best answer! Great JOB. According to ADA Standards, “sudden discontinuation of semaglutide and tirzepatide results in regain of one-half to two-thirds of the weight loss within 1 year. Consider trying lowest effective dose, using intermittent therapy, or stopping medication followed by close weight monitoring. This information is helpful for our clinical practice as we navigate the best approach to utilizing GLP-1 /GIP Therapy.
Answer 3 is incorrect. About 9.28% of respondents chose this. “People experience decreased nausea and less than 10% weight regain.” According to the ADA Standards, people regain 50 to 70% of the weight lost after this gut hormone replacement therapy is stopped.
Finally, Answer 4 is incorrect. 4.57% chose this answer. “People continue behaviors learned on medication with ongoing weight loss success.” According to the ADA Standards, people regain 50 to 70% of the weight lost after this gut hormone replacement therapy is stopped.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Gain fresh insights, practical tools, and a deeper understanding of the latest in person-centered diabetes care. Our expert team brings the ADA Standards of Care to life—covering medications, behavior change, technology, and more! If you’re preparing for the CDCES or BC-ADM exam, this conference—paired with free bonus courses—serves as the ideal study companion!
With interactive co-teaching, we keep sessions engaging, relevant, and fun. Let’s learn and grow together!
Our expert team transforms complex diabetes science into clear, practical insights—keeping it real, engaging, and fun! The faculty includes:
JR has type 2 diabetes and takes Metformin 1000mg BID and sitagliptin (Januvia), A1C 8.1%. GFR 47, UACR 158mg/g. Recent diagnosis of congestive heart failure. These are the medications their insurance covers.
Of the following medications, which addition would most benefit JR?
Gain fresh insights, practical tools, and a deeper understanding of the latest in person-centered diabetes care. Our expert team brings the ADA Standards of Care to life—covering medications, behavior change, technology, and more! If you’re preparing for the CDCES or BC-ADM exam, this conference—paired with free bonus courses—serves as the ideal study companion!
With interactive co-teaching, we keep sessions engaging, relevant, and fun. Let’s learn and grow together!
Our expert team transforms complex diabetes science into clear, practical insights—keeping it real, engaging, and fun! The faculty includes:
For last week’s practice question, we quizzed participants on. 79% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question.
Question:
According to the 2025 ADA Standards of Care, which of the following nutrition behaviors are strongly encouraged for individuals with diabetes?
Answer Choices:
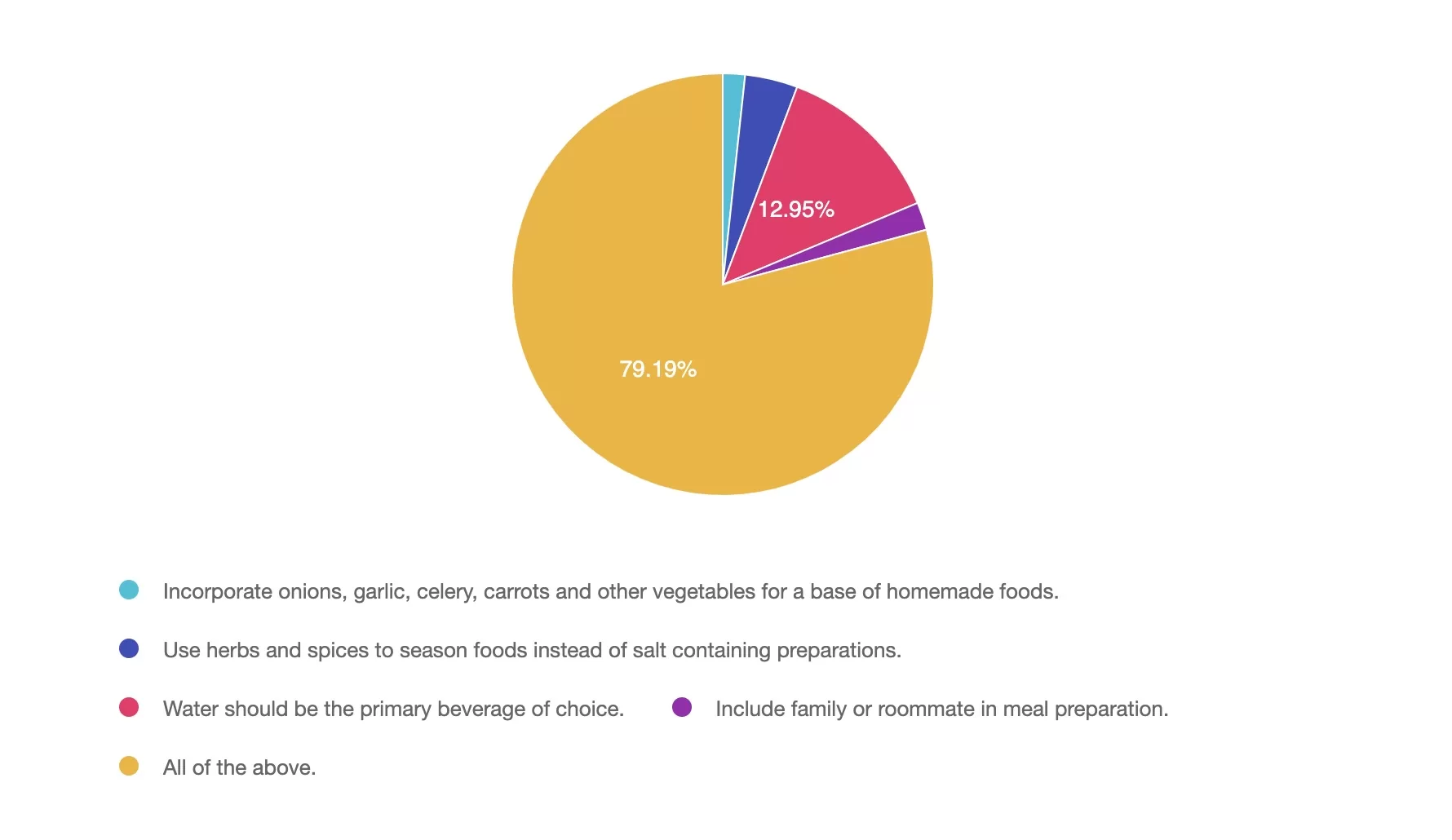
Answer 1 is incorrect. 1.7% chose this answer, ” Incorporate onions, garlic, celery, carrots and other vegetables for a base of homemade foods.” Although this answer is true, it is not the best answer. Incorporate onions, garlic, celery, carrots, and other vegetables for a base of homemade foods. These foods can serve as a base to many dishes and incorporates flavor, fiber, vitamins, and minerals while encouraging vegetable consumption.
Answer 2 is incorrect. 4% of you chose this answer, “Use herbs and spices to season foods instead of salt containing preparations.” Although this answer is true, it is not the best answer. 90% of people in the US exceed the daily recommended limits for sodium. Reducing salt intake is important for heart health, managing blood pressure and meeting dietary guidelines. Herbs and spices not only enhance flavor and may provide additional health benefits.
Answer 3 is incorrect. About 12% of respondents chose this, “Water should be the primary beverage of choice.” Although this answer is true, it is not the best answer. The 2025 ADA Standards of Care have emphasized water as the primary beverage of choice. Alternatives to plain water can include no calorie alternatives. Suggestions to add lemon, lime or cucumber to water, choose sparkling no calorie beverages and no-calorie carbonated beverages are also encouraged.
Answer 4 is incorrect. 2% chose this answer, “Include family or roommate in meal preparation.” Although this answer is true, it is not the best answer. Engaging others in meal preparation can create a supportive environment, encourage healthier eating habits, and make cooking more enjoyable. Social support can be especially helpful in managing diabetes long-term.
Answer 5 is correct. 79% chose this answer, “All of the above.” The 2025 ADA Standards of Care encourages all the above nutrition behaviors.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Gain fresh insights, practical tools, and a deeper understanding of the latest in person-centered diabetes care. Our expert team brings the ADA Standards of Care to life—covering medications, behavior change, technology, and more! If you’re preparing for the CDCES or BC-ADM exam, this conference—paired with free bonus courses—serves as the ideal study companion!
With interactive co-teaching, we keep sessions engaging, relevant, and fun. Let’s learn and grow together!
Our expert team transforms complex diabetes science into clear, practical insights—keeping it real, engaging, and fun! The faculty includes: