Subscribe
eNewsletter
Ready to get certified?
Free CDCES Coach App
eNewsletter
Free CDCES Coach App
Free Med Pocket Cards
We are geared up to help grow and mentor future Certified Diabetes Care and Education Specialists (CDCES) to meet the increasing and varied needs of our diabetes community.
We are offering 14 Bridge Scholarships, which cover the registration cost for our “Virtual DiabetesEd Conference” on April 15-17, 2026. This program will provide you with diabetes fundamentals and beyond! Earn 30+ CEs with access to the courses for one year!
Over the next 10 years we are “Building a Bridge” to welcome a thousand new diabetes educators into the field. If you know a healthcare professional seeking a new challenge and eager to pursue a meaningful and rewarding specialty, please invite them to consider becoming a Certified Diabetes Care and Education Specialist (CDCES).
Diabetes Education Services is committed to improving equity and access to diabetes training and education for a diverse group of healthcare professionals. We don’t want financial barriers to stop anyone from attending this conference. In appreciation of those who are role models and advocates for practicing the best diabetes care in their communities.
The Bridge Scholarship program is not just about learning—it’s about creating connections, fostering growth and building a community of passionate diabetes care professionals. We are excited to offer this incredible opportunity to those who are committed to advancing their skills and knowledge in diabetes education. Together, we can make a real difference in the lives of those living with diabetes.
These scholarships are awarded to healthcare professionals who provide care and education to under-served communities that lack access to Diabetes Specialists and healthcare resources. Applicants must be in the process of gaining practice hours and planning to take their CDCES Exam within the next 3 years.
Gain fresh insights, practical tools, and a deeper understanding of the latest in person-centered diabetes care. Our expert team brings the ADA Standards of Care to life—covering medications, behavior change, technology, and more!
If you’re preparing for the CDCES or BC-ADM exam, this conference, paired with a handful of free bonus courses, serves as the ideal study companion! Plus, this content counts toward the ADA Standards requirements for CDCES Renewal.
For last week’s practice question, we quizzed participants on CS’s A1C climbing after experiencing distress. 50.55% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question

CS is a 42-year-old with type 1 diabetes for just over 18 years. In the past year, their A1C changed from 7.4% to 9.1%, and weight increased by 20 pounds. Review of CGM data suggests missed insulin boluses more than 7 times per week, and discussion with CS reveals missed clinic visits due to feeling “burned out”. They score in the moderate range on the Diabetes Distress Scale.
Based on the ADA 2026 Standards of Care, which of the following is the most appropriate next step?
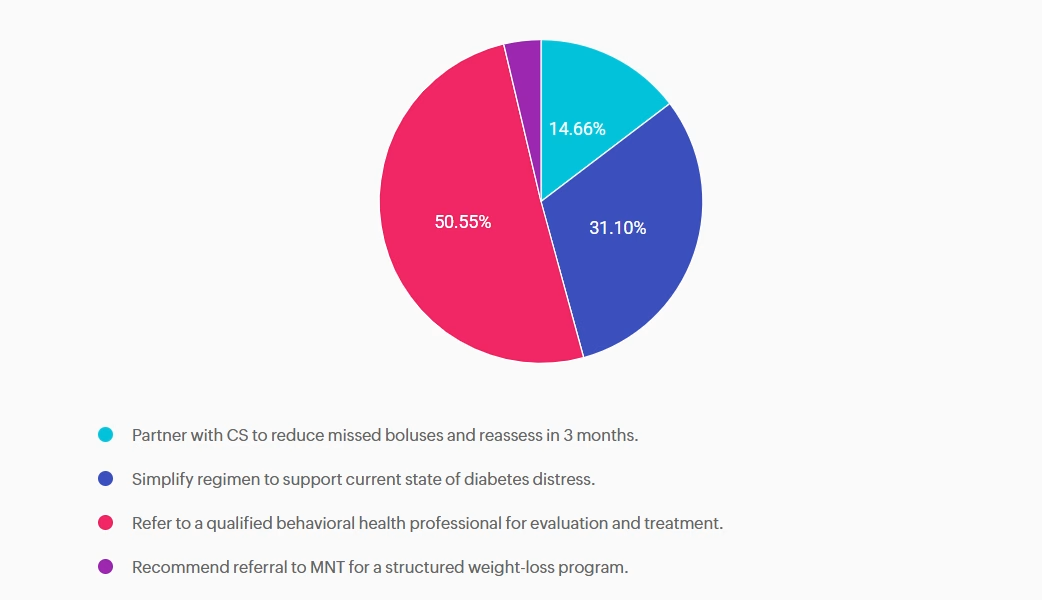
Answer A is incorrect: 14.66% chose this answer, “Partner with CS to reduce missed boluses and reassess in 3 months.” While reducing missed boluses and optimizing insulin therapy are essential to support A1c reduction, this intervention alone does not address the likely underlying psychological barriers to self-management.
Answer B is incorrect: 31.1% chose this answer, “Simplify regimen to support current state of diabetes distress.” While simplifying insulin dosing may be supportive in some cases, without addressing the underlying diabetes distress it is unlikely to achieve sustained improvement.
Answer C is correct: 50.55% chose this answer, “Refer to a qualified behavioral health professional for evaluation and treatment.” The 2026 ADA Standards of Care recommends a referral to a qualified behavioral health professional for evaluation and treatment when diabetes distress, burnout, reduced engagement in diabetes management or other psychosocial factors are impacting self-care and glycemic targets. ¹
Answer D is incorrect: 3.7% chose this answer, “Recommend referral to MNT for a structured weight-loss program.” Focusing solely on weight loss does not address the primary psychosocial barriers and weight gain may be a symptom of underlying behavioral health needs. Evaluation and treatment from a behavioral health provider would be the most appropriate next step.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!

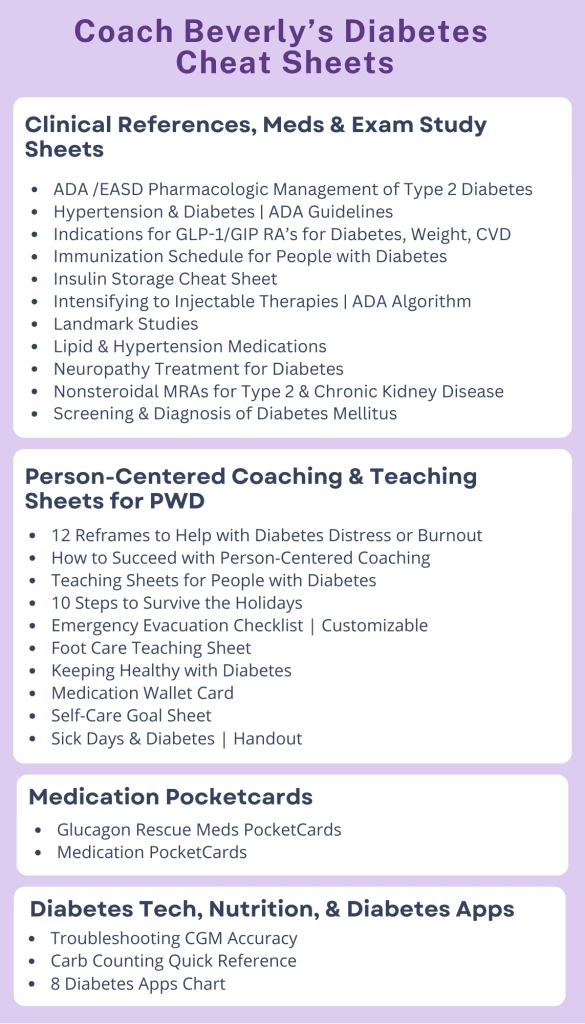
If you’re a busy diabetes healthcare professional, you want tools that help you deliver excellent, evidence-based care—without spending hours digging for information. That’s exactly why we created our Diabetes Cheat Sheet Resource Page, and we’re excited to share that it’s been updated with new additions for 2026.
You can download these free clinical and teaching cheat sheets directly from our website or through the CDCES Coach App. To make your life easier, we’ve reorganized everything by category and alphabetically, so you can quickly find exactly what you need—right when you need it.
The first section focuses on concise, evidence-based clinical summaries drawn from the American Diabetes Association Standards of Care and current research. These resources are ideal for:
The next section includes ready-to-use handouts designed for people living with diabetes. Many are available in both English and Spanish, and several allow you to add your own logo or tailor the content to better serve your population.
A highlight of this section is the new “Keeping Healthy with Diabetes” sheets. These were personally created by Coach Beverly as teaching tools for community classes and for the people she serves in a rural health clinic. They clearly summarize:
Perfect for printing, sharing, and using in real-world conversations.
You’ll also find dedicated sections on:
Whether you’re caring for people with diabetes, teaching others, or preparing for an exam, these updated resources are designed to save you time, reduce overwhelm, and support best-in-class care.

Peripheral Artery Disease (PAD) is significantly underdiagnosed. While PAD affects around 8.5 million Americans and prevalence rises with age (up to 20% over 60), only 10-20% are clinically diagnosed, highlighting a major gap in awareness and screening.
According to the ADA Standards, what needs to be included in the initial screening for PAD?
Featured Articles ___________________________ |
Greetings, wonderful healthcare colleagues!
You are going to love all the updates to our cheat sheets, online university courses, and PocketCards.
Coach Beverly has been excitedly scanning the 2026 ADA Standards to discover updates and advances in diabetes care. She and her team are hustling to integrate these new findings across our platforms, including the CDCES Coach App, handouts, courses, and web content, so that you can access the latest information with confidence.
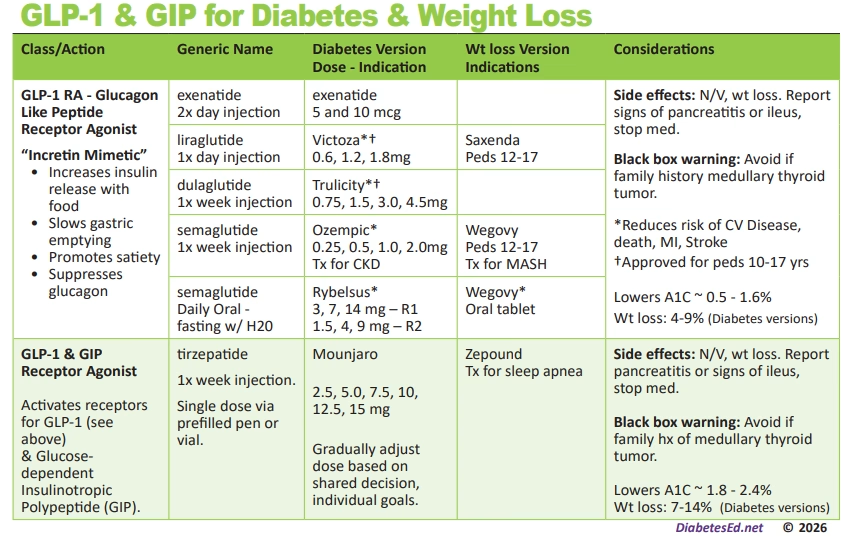
In our first newsletter of 2026, we are excited to share that we have made significant changes to our Medication PocketCards in the GLP-1/GIP RA section. Now included are the diabetes and weight-loss versions of this popular medication class, with indications for each. You can compare and contrast at a glance. Download your free version and read more below.
Our library of Cheat Sheets is updated and includes a few new additions! These sheets are available on our website and the CDCES Coach App for easy access, with the option to download and share with your colleagues and people living with diabetes alike.
Christine Craig, MS, RD, CDCES, explores her experience with a client who arrived at her office distraught and struggling with the loss of his lifelong partner. Pass the tissues.
Our Tech contributor, Dr. Beattie, provides a summary of red flag statements that may indicate a person is experiencing barriers to effectively using technology in their day-to-day management.
We encourage you to test your knowledge with our Question and Rationale of the Week. January kicks off our Level 1 Fundamental Series, followed by our annual ADA Standards of Care update on January 29th and Level 2 Mastery Course Series in February. We hope to see you there!
Here is to a 2026 filled with self-compassion and moments of awe.
Coach Beverly, Bryanna, Astraea & Katarina
For last week’s practice question, we quizzed participants on Katie needing support with improving her glycemic management, and what would be the best response. 76.5% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Katie is a 14-year-old living with type 1 diabetes since age 10. She uses multiple daily insulin injections (MDI) therapy to manage her diabetes and started using a continuous glucose monitor (CGM) 3 months ago at the recommendation of her endocrinology team. Her A1c has increased to 9.2% since starting CCM technology.
Her mother reports that Katie has episodes of prolonged hyperglycemia when she is away from home. When at home, her mother will remind Katie to bolus based on the alerts she gets on the CGM share app. Katie reports she mutes alarms and alerts because she doesn’t want her classmates to hear them, afraid they will judge her. When you ask if she has uploaded her data to the school nurse or her endocrinology team she says, “The app is really confusing.” Her mother is frustrated with Katie for not paying attention to the CGM, saying, “She can text her friends without any problem; I don’t know why she struggles with the CGM”.
As the diabetes healthcare provider, how can you support Katie in improving her glycemic control?
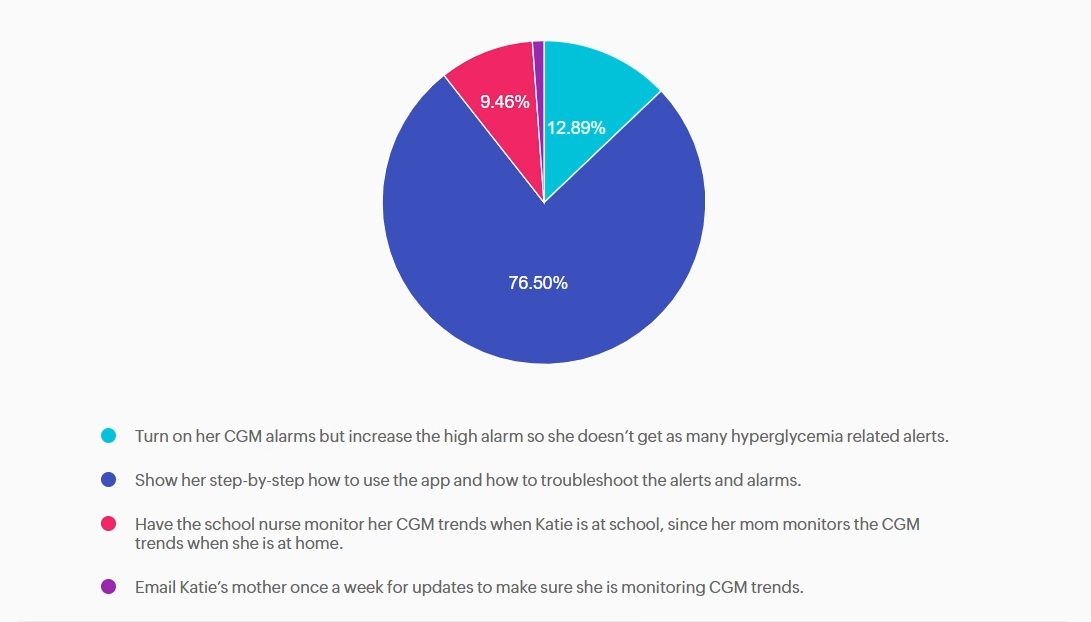
Answer A is incorrect: 12.89% chose this answer, “Turn on her CGM alarms but increase the high alarm so she doesn’t get as many
hyperglycemia related alerts.” Helping Katie turn on and increasing her high alarm will not help improve her glycemic management.
Answer B is correct: 76.5% chose this answer, “Show her step-by-step how to use the app and how to troubleshoot the alerts and alarms.” Guiding Katie through the CGM app and its functions helps her ask questions, resolve issues, and better monitor her glycemic management.
Answer C is incorrect: 9.46% chose this answer, “Have the school nurse monitor her CGM trends when Katie is at school, since her mom monitors the CGM trends when she is at home.” Asking the school nurse to monitor CGM data while Katie is at school is not helping to improve Katie’s self-management skills.
Answer D is incorrect: 1.15% chose this answer, “Email Katie’s mother once a week for updates to make sure she is monitoring CGM
trends.” Emailing Katie’s mother does not help improve Katie’s CGM self-monitoring skills or her confidence level with the CGM app.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Gain fresh insights, practical tools, and a deeper understanding of the latest in person-centered diabetes care. Our expert team brings the ADA Standards of Care to life—covering medications, behavior change, technology, and more!
If you’re preparing for the CDCES or BC-ADM exam, this conference, paired with a handful of free bonus courses, serves as the ideal study companion! Plus, this content counts toward the ADA Standards requirements for CDCES Renewal.
With interactive co-teaching, we keep sessions engaging, relevant, and fun.
Let’s learn and grow together!
Course credits through AMA PRA Category 1 Credits™, ACPE, ANCC, and CDR!
Program Objectives:
Upon completion of this activity, participants should be able to:
For last week’s practice question, we quizzed participants on the new ADA Standards and the development of type 2 diabetes. 42.48% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
According to the new 2026 ADA Standards, “type 2 diabetes is associated with insulin secretory defects related to” which of the following?
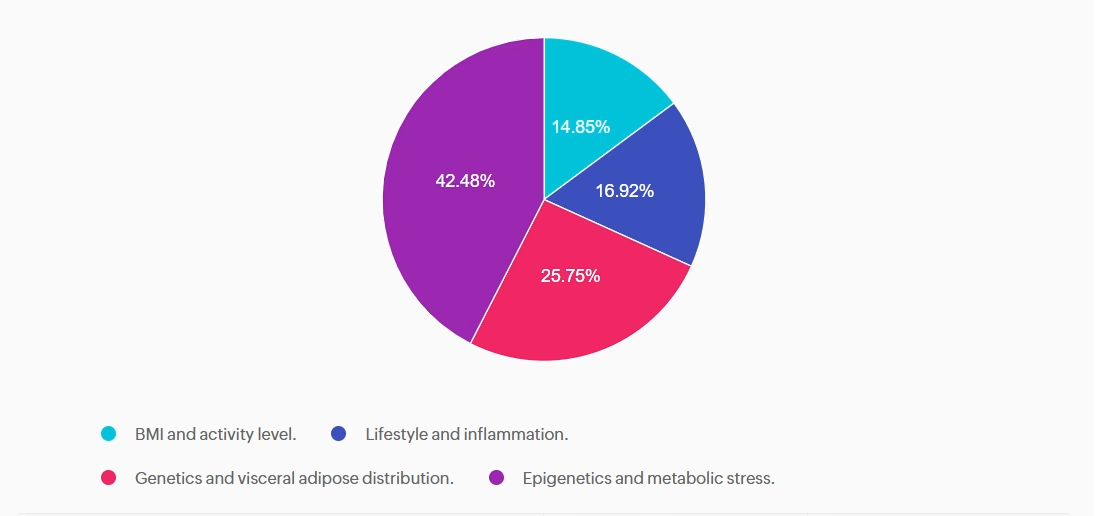
Answer A is incorrect: 14.85% chose this answer, “BMI and activity level.” This answer is incorrect but tempting. BMI level is used as a a screening tool for prediabetes and diabetes risk, but is not included as a factor contributing to secretory defects. According to the ADA, there are four factors related to insulin secretory defects in type 2 diabetes. They include; genetics, epigenetics, metabolic stress and inflammation.
Answer B is incorrect: 16.92% chose this answer, “Lifestyle and inflammation.” This juicy answer is incorrect. Lifestyle is not a direct factor related to insulin secretory defects, but inflammation is a contributor. According to the ADA, there are four factors related to insulin secretory defects in type 2 diabetes. They include; genetics, epigenetics, metabolic stress and inflammation.
Answer C is incorrect: 25.75% chose this answer, “Genetics and visceral adipose distribution.” This answer is incorrect. Visceral adiposity is associated with an increased risk for diabetes, but does not contribute to insulin secretory defects. According to the ADA, there are four factors related to insulin secretory defects in type 2 diabetes. They include; genetics, epigenetics, metabolic stress and inflammation.
Answer D is correct: 42.48% chose this answer, “Epigenetics and metabolic stress.” This answer is correct, GREAT JOB! According to the ADA, there are four factors related to insulin secretory defects in type 2 diabetes. They include; genetics, epigenetics, metabolic stress and inflammation.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!

Our GLP-1 & GIP Meds PocketCard now includes two distinct versions—one for diabetes and one for weight management—so you can compare therapies at a glance.
Each version clearly outlines:
This side-by-side approach makes it easier to individualize treatment decisions based on a person’s health profile, age, and comorbidities.
Big news in the GLP-1 world! Semaglutide is now available as an oral formulation for weight loss, and we’ve added it to the PocketCard.
Just like Rybelsus, oral semaglutide for weight loss:
It’s the end of an era. Exenatide XR (Bydureon®, Bcise®) has been discontinued.
The only remaining option is generic exenatide, administered twice daily—still available and noted on the updated PocketCard.
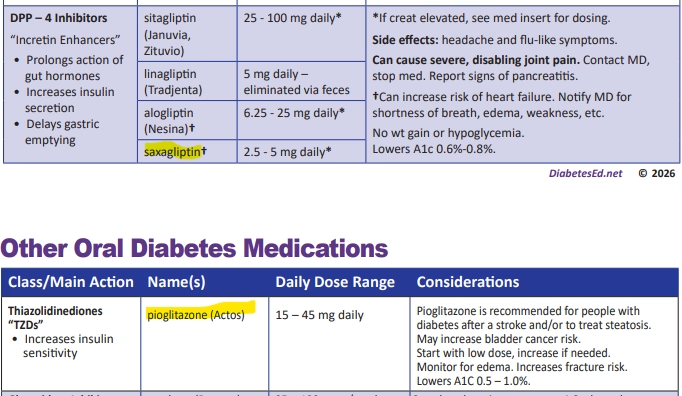
We say goodbye to rosiglitazone and welcome a renewed appreciation for pioglitazone (Actos®).
Pioglitazone:
Research led by Dr. Ralph DeFronzo demonstrates that pioglitazone can shift fat from visceral to subcutaneous depots, improving metabolic health and liver outcomes.
Clinical pearls included on the card:
Importantly, pioglitazone is also indicated for people with prediabetes or diabetes who have experienced a stroke, as it significantly reduces the risk of recurrent stroke.
DPP-4 inhibitors continue to decline in use due to lower efficacy and higher cost, and both alogliptin and saxagliptin carry an increased risk of hospitalization for heart-failure .
That said, generic saxagliptin is once again available, so we’ve added it back to the PocketCard in the DPP-4 category—clearly labeled to support informed prescribing.