
Subscribe
eNewsletter
Ready to get certified?
Free CDCES Coach App
eNewsletter
Free CDCES Coach App

For last week’s practice question, we quizzed participants on how much does Diabetes Cost the U.S? 69% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question: According to the recently published ADA report on the 2022 Economic Costs of Diabetes in the U.S., which of the following statements is most accurate?
Answer Choices:
If you are thinking about taking the certification exam, this practice test question will set you up for success. Test writers anticipate possible answers based on the details in the question. They will wave those “juicy answers” right under your nose. Your job is to weed through the particulars, pluck out the most important elements and choose the BEST answer.
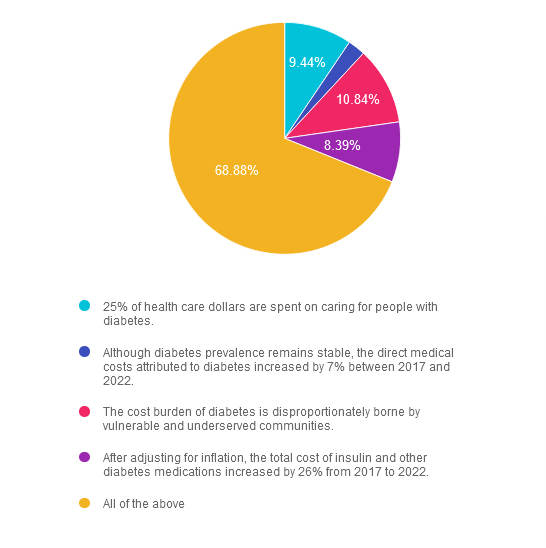
Answer 1 is incorrect. 9.44% chose this answer. “25% of health care dollars are spent on caring for people with diabetes.” Yes, a quarter of all health care dollars are spent on diabetes, with the majority of money spent on hospitalizations due to cardiovascular complications and medications. Read more details in the Diabetes Care Article, “Economic Costs of Diabetes in the U.S. 2022.
Answer 2 is incorrect. 2.45% of you chose this answer. “Although diabetes prevalence remains stable, the direct medical costs attributed to diabetes increased by 7% between 2017 and 2022.” The cost of treating diabetes keeps increasing, putting additional financial strain on people living with diabetes. Read more details in the Diabetes Care Article, “Economic Costs of Diabetes in the U.S. 2022.
Answer 3 is incorrect. About 10.84% of respondents chose this. “The cost burden of diabetes is disproportionately borne by vulnerable and underserved communities.” People who earn the least amount of money and live in under-resourced areas, continue to have the highest rates of diabetes and other chronic health conditions. Read more details in the Diabetes Care Article, “Economic Costs of Diabetes in the U.S. 2022.
Answer 4 is incorrect. About 8.39% of respondents chose this. “After adjusting for inflation, the total cost of insulin and other diabetes medications increased by 26% from 2017 to 2022.” Yes, the cost of medications keeps increasing, which may prevent many people from accessing optimal diabetes treatment. Read more details in the Diabetes Care Article, “Economic Costs of Diabetes in the U.S. 2022
Finally, Answer 5 is correct. 68.88% chose this answer. “All of the above” YES, GREAT JOB. Most of you chose the BEST Answer. Thank you for participating in our Question of the Week. All data is based on the Diabetes Care Article, “Economic Costs of Diabetes in the U.S. 2022”, published in November 2023
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
All data is based on the Diabetes Care Article, “Economic Costs of Diabetes in the U.S. 2022”, published in November 2023
Topics:
This course discusses common causes of hyperglycemia crises. Topics include hyperglycemia secondary to medications & insulin deprivation. The differences & similarities between Diabetes Ketoacidosis and hyperosmolar Hyperglycemic Syndrome are also covered. Treatment strategies for all situations are included.
Can’t make it live? No worries. We will send post the recorded version to the Online University within 24 hours of the broadcast
Instructor: Beverly Thomassian RN, MPH, CDCES, has been Board Certified in Advanced Diabetes Management for over 20 years. She is an Associate Clinical Professor at UCSF, a working educator, and a nationally recognized diabetes expert. She has a Master’s Degree in Public Health from UCLA, with a focus on behavioral health and education.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the diabetes certification exams. CBDCE & ADCES does not endorse any preparatory or review materials for the certification exams, except for those published by CBDCE & ADCES.
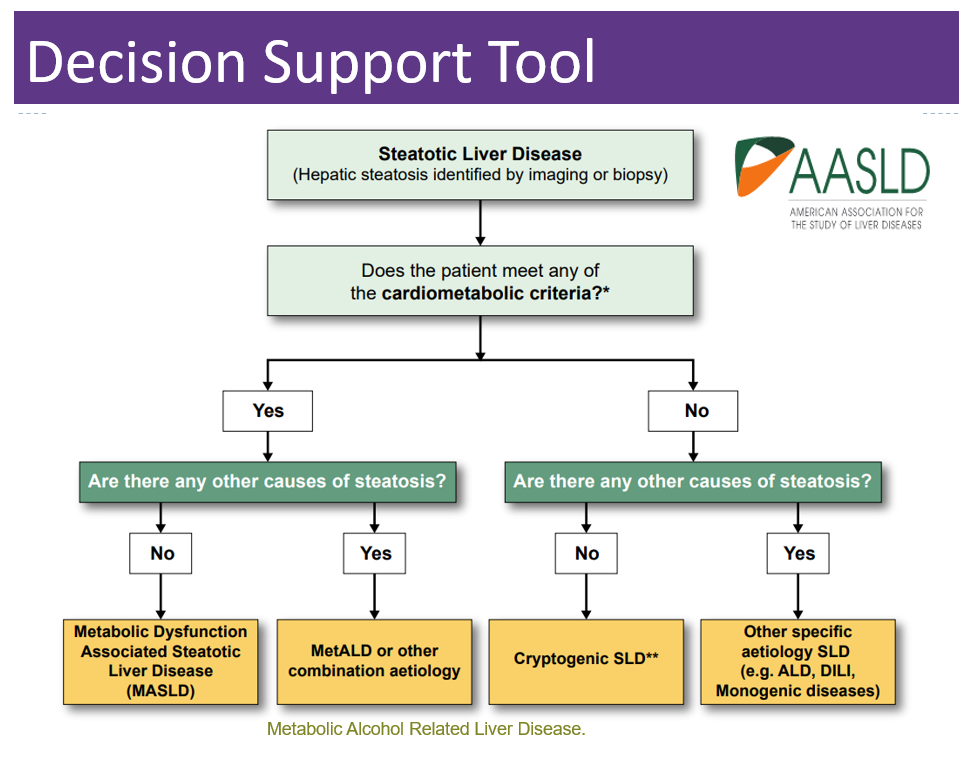
The American Association for the Study of Liver Diseases recently announced that they are updating their terms for Non-Alcoholic Steatohepatitis (NASH) and Non-Alcoholic Fatty Liver Disease (NAFLD).
Since NAFLD is considered the “hepatic manifestation of metabolic syndrome,” the organization wants the terminology to better reflect this metabolic inflammation and update the language to remove the stigma associated with the terms “fatty” and “non-alcoholic.”
According to the American Diabetes Association, NAFLD is prevalent in more than 70% of people living with diabetes. Early detection and intervention can decrease fat accumulation in the liver and lead to improved health. As diabetes care and education specialists, we can increase awareness and screenings while promoting lifestyle changes and medication therapy to save lives. One way to start the conversation is to share this updated Liver Nomenclature List with your colleagues.
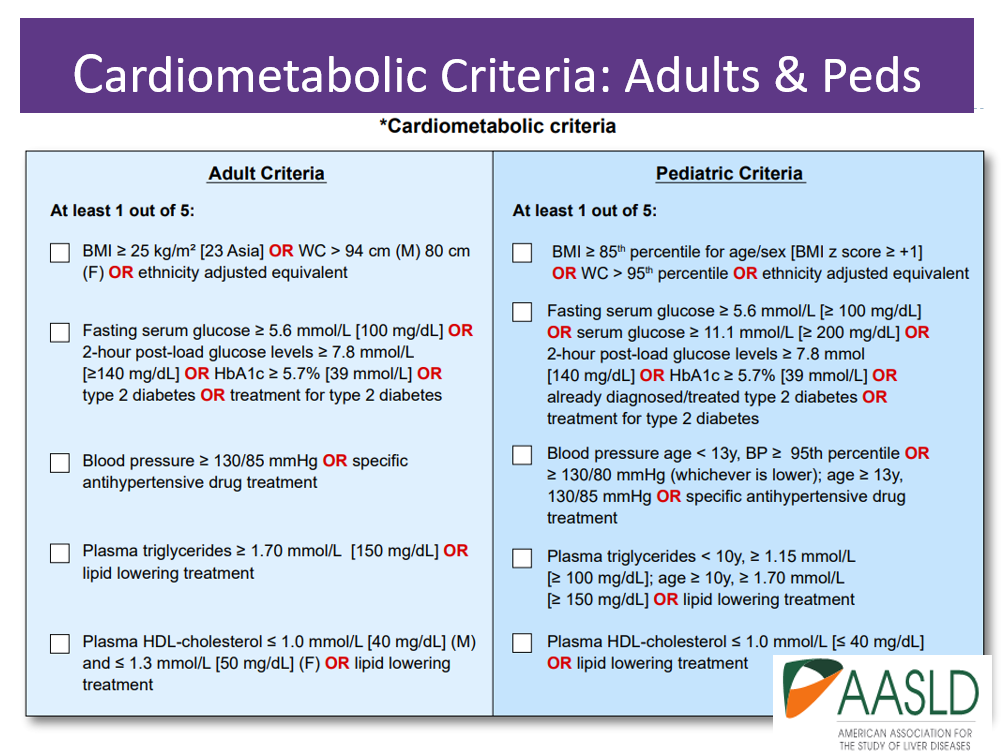
The new names, MASH and MAFLD, take into account the presence of liver disease along with cardiometabolic risk factors such as body weight, glucose levels, blood pressure, triglycerides, and HDL cholesterol levels (see CardioMetabolic table below).
Below is a summary chart from the AADSL that reflects these important changes.
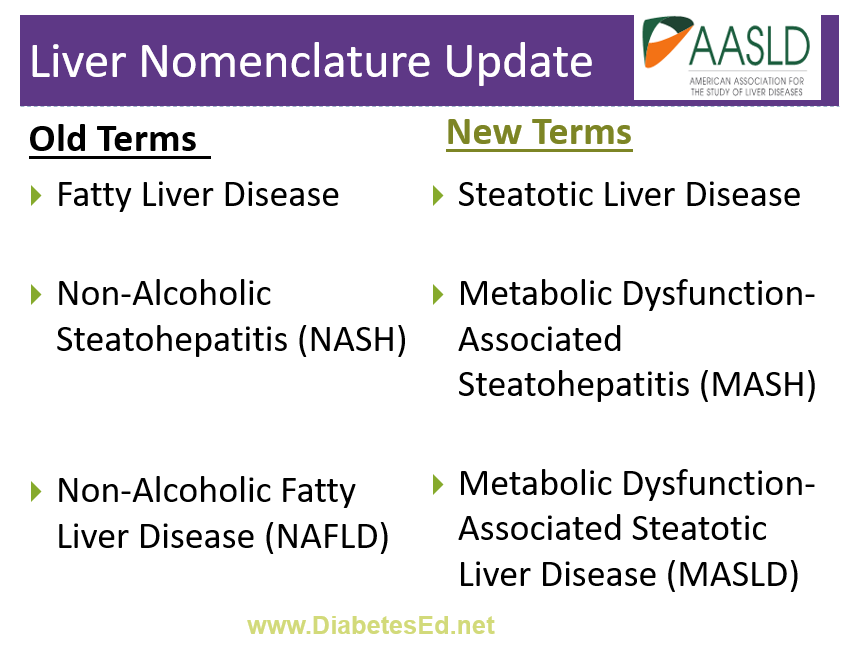
These new terms may not be universally accepted at first and the choice of name may vary by region and among healthcare professionals. Regardless of the name used, the management and understanding of the condition remain crucial to screening, identifying, and treating Steatotic Liver Disease.
Coach Bev invites you to join this 60-minute webinar that covers gastrointestinal health from top to bottom. Topics include; fatty liver disease diagnosis and treatment, intestinal complications associated with diabetes, keeping the microbiome healthy, and more. Join us to explore the magnificent wonders of diabetes and the gut.
Can’t make it live? No worries. We will send post the recorded version to the Online University within 24 hours of the broadcast
Instructor: Beverly Thomassian RN, MPH, CDCES, has been Board Certified in Advanced Diabetes Management for over 20 years. She is an Associate Clinical Professor at UCSF, a working educator, and a nationally recognized diabetes expert. She has a Master’s Degree in Public Health from UCLA, with a focus on behavioral health and education.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
According to recent research by the ADA/EASD, about 10% of people admitted to the hospital in diabetes crisis have euglycemic diabetes ketoacidosis.
Since blood sugars are at normal levels or only slightly elevated, which of the following lab tests most accurately evaluate for euglycemic ketosis?
Click Here to Test your Knowledge
Topics:
This course discusses common causes of hyperglycemia crises. Topics include hyperglycemia secondary to medications & insulin deprivation. The differences & similarities between Diabetes Ketoacidosis and hyperosmolar Hyperglycemic Syndrome are also covered. Treatment strategies for all situations are included.
Can’t make it live? No worries. We will send post the recorded version to the Online University within 24 hours of the broadcast
Instructor: Beverly Thomassian RN, MPH, CDCES, has been Board Certified in Advanced Diabetes Management for over 20 years. She is an Associate Clinical Professor at UCSF, a working educator, and a nationally recognized diabetes expert. She has a Master’s Degree in Public Health from UCLA, with a focus on behavioral health and education.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
We understand the important work you all do every day to support individuals living with and managing diabetes and prediabetes.

We are so thankful for the differences you all make in the world as you address disparities and improve the health of communities locally and across the nation.
We have been so inspired by our students and are so proud of each achievement. If you have a moment, stop by our CDCES Success Stories page to read about the incredible journeys students have taken to become diabetes educators and advocates.
At Diabetes Ed Services, we work diligently every day to provide diabetes information that is relevant, compassionate and cutting edge. We believe in the potential of all students, from people living with diabetes to health care professionals striving to enhance their knowledge. Thank you for being a part of our lives and community.
We will be closing shop starting today for the holidays. We will open our doors at 7am on Monday, well rested, a few pounds heavier and ready for our Cyber Monday Sale.
On behalf of the entire Diabetes Education Services Team, Happy Thanksgiving!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
For last week’s practice question, we quizzed participants on why we celebrate World Diabetes Day on Nov 14th. 39% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
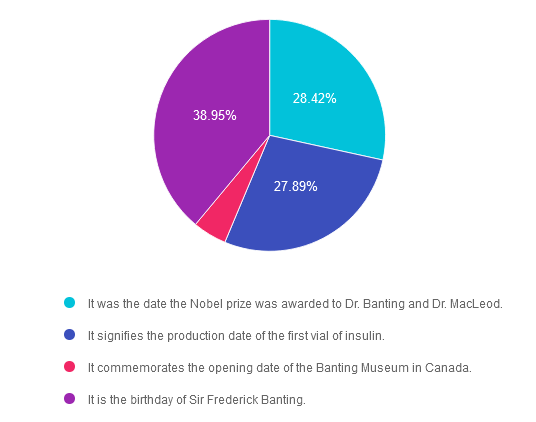
Question: In 1923, the Nobel prize in Physiology or Medicine was awarded to Frederick Grant Banting and John James Richard MacLeod “for the discovery of insulin”. 100 years later, we celebrate this life-saving discovery each year on November 14th, a day designated as World Diabetes Day.
Why do we celebrate World Diabetes Day on November 14th? Please choose the best answer.
Answer Choices:
If you are thinking about taking the certification exam, this practice test question will set you up for success. Test writers anticipate possible answers based on the details in the question. They will wave those “juicy answers” right under your nose. Your job is to weed through the particulars, pluck out the most important elements, and choose the BEST answer.
Answer 1 is incorrect. 28.42% chose this answer. “It was the date the Nobel Prize was awarded to Dr. Banting and Dr. MacLeod.” This is not the reason, however it is interesting to note that the Nobel prize for the discovery of insulin was awarded on December 10, 1923 in Stockholm, Sweden.
Answer 2 is incorrect. 27.89% of you chose this answer. “It signifies the production date of the first vial of insulin.” Great guess. However, it wasn’t until 1923 that the first vials of insulin were commercially produced and distributed.
Answer 3 is incorrect. About 4.74% of respondents chose this. “It commemorates the opening date of the Banting Museum in Canada.” The Banting House is a former residence and current museum in London, Ontario, Canada, known as the “Birthplace of Insulin.” It is the house where Sir Frederick Banting woke up at two o’clock in the morning on October 31, 1920 with the idea that led to the discovery of insulin. Since 1984, the house has been a museum dedicated to Banting’s discovery and his life.
Finally, Answer 4 is correct. 38.95% chose this answer. “It is the birthday of Sir Frederick Banting.” YES, this is the best answer. Dr. Banting was born on November 14, 1891. That is why we celebrate World Diabetes Day on November 14th.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
.png?h=459&iar=0&w=1459&hash=E665292742D2BABAECCFA59A56B88D3C)
November kicks off National Diabetes Month, a time to recognize that over 11% of Americans are living with diabetes and over 35% have prediabetes. Since diabetes results from a combination of genetics plus environment, there is a recognition that social determinants of health play a pivotal role in the development of diabetes and its complications. Through advocacy and education, we can inform individuals on best care for diabetes and support them in taking action to improve the health of their communities to prevent future diabetes. We have put together a list of FREE diabetes resources in English and Spanish to share with people living with prediabetes and diabetes. Thank you for your advocacy and belief that we can make a difference. Coach Beverly
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
According to the recently published ADA report on the 2022 Economic Costs of Diabetes in the U.S., which of the following statements is most accurate?
Click Here to Test your Knowledge
November kicks off National Diabetes Month, a time to recognize that over 11% of Americans are living with diabetes and over 35% have prediabetes. Since diabetes results from a combination of genetics plus environment, there is a recognition that social determinants of health play a pivotal role in the development of diabetes and its complications. Through advocacy and education, we can inform individuals on best care for diabetes and support them in taking action to improve the health of their communities to prevent future diabetes. We have put together a list of FREE diabetes resources in English and Spanish to share with people living with prediabetes and diabetes. Thank you for your advocacy and belief that we can make a difference. Coach Beverly
All hours earned count toward your CDCES Accreditation Information
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
To recognize Native American Heritage Month, we are honored to share a treasured poem by one of my favorite poets and writers, Joy Harjo. Plus, we also share an interactive map of Indigenous Lands (credit to NPR).
In 2019, Joy Harjo was recognized as the United States poet laureate and served three terms. Harjo is an internationally renowned performer and writer of the Muscogee (Creek) Nation.
She lives in Tulsa, Oklahoma and is the author of nine books of poetry, including the highly acclaimed An American Sunrise, several plays and children’s books, and two memoirs, Crazy Brave and Poet Warrior. Her many honors include the Ruth Lily Prize for Lifetime Achievement from the Poetry Foundation, the Academy of American Poets Wallace Stevens Award, two NEA fellowships, and a Guggenheim Fellowship.
You can learn more about Joy Harjo on her webpage, www.joyharjo.com.
Joy Harjo
Remember the sky that you were born under,
know each of the star’s stories.
Remember the moon, know who she is.
Remember the sun’s birth at dawn, that is the
strongest point of time. Remember sundown
and the giving away to night.
Remember your birth, how your mother struggled
to give you form and breath. You are evidence of
her life, and her mother’s, and hers.
Remember your father. He is your life, also.
Remember the earth whose skin you are:
red earth, black earth, yellow earth, white earth
brown earth, we are earth.
Remember the plants, trees, animal life who all have their
tribes, their families, their histories, too. Talk to them,
listen to them. They are alive poems.
Remember the wind. Remember her voice. She knows the
origin of this universe.
Remember you are all people and all people
are you.
Remember you are this universe and this
universe is you.
Remember all is in motion, is growing, is you.
Remember language comes from this.
Remember the dance language is, that life is.
Remember.
Indigenous Peoples’ Day is a time of reflection, recognition and celebration of the role Native people have played in U.S. history. One way to mark the day — and to learn about Indigenous history year-round — is to learn which Native lands you live on.


November is Transgender Awareness Month and in honor of our Trans and Gender Non-conforming community, we want to share some helpful resources for Diabetes Specialists to create more inclusive practices.
Whether we provide services in the hospital, clinic, or other outpatient settings, we can take steps to help the people we work with feel welcome.
“Members of the lesbian, gay, bisexual, transgender and queer (LGBTQ) community have unique health disparities and worse health outcomes than their heterosexual counterparts, which has clinical relevance in the delivery of diabetes care and education. Diabetes care and education specialists are in a pivotal position to help this medically-underserved and vulnerable population get the best possible care.”
Association of Diabetes Care & Education Specialists (ADCES)
Create healthcare settings that send a message of welcomeness to the Trans and greater LGBQIA+ community. There are many small and big ways to send a message of inclusion.
Cultural humility asks health care providers to develop critical self-awareness of personal implicit or explicit values and behaviors that may contribute to health care disparities. Cultural humility acknowledges the role of power and privilege within the patient-provider dynamic and within the health care system itself. Cultural values and behaviors emanating from the provider actually have the power to shape the encounter and may minimize the values of the person seeking care. By taking a closer look at our own biases during interactions, we can start becoming more intentional and align with the individual’s needs and values when providing care.
As Diabetes Educators, we recognize the importance of language in providing person-centered care to best support people living with diabetes.
There are a few small changes we can make to provide inclusive care for all people. To make our practices more welcoming, we can establish All Gender Restrooms and update our materials to use gender-inclusive language. Here is a list of terms and tips for shifting this language and creating more inclusive practices.
The easiest way to become more inclusive in our language which respects the autonomy of each individual to describe themselves and their bodies is to give them opportunities to share with us what those terms are and how they would like to be referred to.
A few ways you can do this are by expanding the ways we collect this information in our intake forms or discussing it with the individual in their initial appointment. You can incorporate sections to ask for someone’s pronouns or even a body map where someone can make notes about the preferred language that is used around their bodies. Giving space to outline triggering or preferred language for each person can empower not only gender-diverse people but can also support trauma survivors of all genders.
By paying careful attention to each person’s experience from the moment they walk in the door until we say goodbye, we can find ways to create a more inclusive environment. This awareness of the details is the great first step to showing your care and respect for those you work with.
List of Resources
ADCES Inclusive Care for LGBTQ+ People with Diabetes Handout – this handout provides definitions, terms to avoid, and a cultural competency checklist to help you move towards improving inclusivity within your practice.
All Gender Restroom Sign PDF
Inclusive Perinatal Care – Our blog on shifting language for more inclusive perinatal care.
Diabetes Prevention and Management for LGBTQ+ People Handout – this handout includes research of diabetes within the LGBTQ+ community, along with clinical considerations, programs, and resources for diabetes educators to use within their practice.
Policies on Lesbian, Gay, Bisexual, Transgender & Queer (LGBTQ+) issues – this resource by the American Medical Association lists all the current healthcare policies in place for the LGBTQ+ community.
Helio’s LGBTQ+ Health Updates Resource Center – this is a “collection of news articles and features that provide the latest information on the unique health needs of individuals in the LGBTQ+ community.
Online Therapy Guide for LGBTQ+ Youth – this resource uncovers common mental health problems and causes in LGBTQ+ youth and gives pointers on finding the right online therapist.
Are we missing important information and resources? Send us your favorites to [email protected].

For more information, read our Expert Interview with Theresa Garnero, APRN, BC-ADM, MSN, CDE President of Sweet People Club, and writer of the article “Providing Culturally Sensitive Care for the Lesbian, Gay, Bisexual, and Transgender (LGBT) Community” in Diabetes Spectrum.
November kicks off National Diabetes Month, a time to recognize that over 11% of Americans are living with diabetes and over 35% have prediabetes. Since diabetes results from a combination of genetics plus environment, there is a recognition that social determinants of health play a pivotal role in the development of diabetes and its complications. Through advocacy and education, we can inform individuals on best care for diabetes and support them in taking action to improve the health of their communities to prevent future diabetes. We have put together a list of FREE diabetes resources in English and Spanish to share with people living with prediabetes and diabetes. Thank you for your advocacy and belief that we can make a difference. Coach Beverly
All hours earned count toward your CDCES Accreditation Information
