
Subscribe
eNewsletter
Ready to get certified?
Free CDCES Coach App
eNewsletter
Free CDCES Coach App

For last week’s practice question, we quizzed participants on diabetes & the impact it has on communities. 82% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question: November is National Diabetes Month. This month shines a spotlight on the 37 million people living with diabetes and the 96 million with prediabetes. Certain communities are hit harder with diabetes than others due to a combination of genetics and social determinants of health.
Which of the following statements are most accurate?
Answer Choices:
If you are thinking about taking the certification exam, this practice test question will set you up for success. Test writers anticipate possible answers based on the details in the question. They will wave those “juicy answers” right under your nose. Your job is to weed through the particulars, pluck out the most important elements and choose the BEST answer.
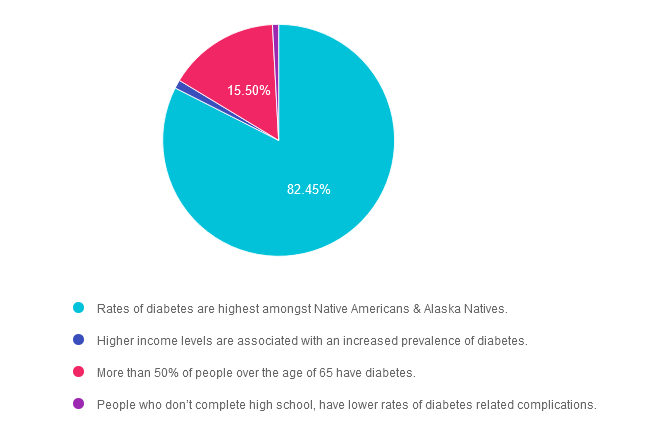
Answer 1 is correct. 82.45% chose this answer. “Rates of diabetes are highest amongst Native Americans & Alaska Natives.” YES, sadly, this is the best answer. For both men and women, prevalence of diagnosed diabetes was highest among American Indian and Alaska Native adults (13.6%), followed by non-Hispanic Black adults (12.1%), adults of Hispanic origin (11.7%), non-Hispanic Asian adults (9.1%) and non-Hispanic White adults (6.9%) (See CDC Appendix Table 3). As diabetes advocates, we can campaign for improved access to health care and address social determinants of health for communities at highest risk of prediabetes and diabetes.
Answer 2 is incorrect. 1.19% of you chose this answer. “Higher income levels are associated with an increased prevalence of diabetes.” People who have the lowest earnings and who don’t graduate high school have the highest rates of diabetes. Socioeconomic status and rates of diabetes are inversely related.
Answer 3 is incorrect. About 15.5% of respondents chose this. “More than 50% of people over the age of 65 have diabetes.” This is a tempting answer, but a little exaggerated. According to CDC Stats, 30% of people age 65 or live with diabetes.
Finally, Answer 4 is incorrect. 0.85% chose this answer. “People who don’t complete high school, have lower rates of diabetes related complications.” People who don’t graduate high school have the highest rates of diabetes and less resources to engage in preventive care.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
November kicks off National Diabetes Month, a time to recognize that over 11% of Americans are living with diabetes and over 35% have prediabetes. Since diabetes results from a combination of genetics plus environment, there is a recognition that social determinants of health play a pivotal role in the development of diabetes and its complications. Through advocacy and education, we can inform individuals on best care for diabetes and support them in taking action to improve the health of their communities to prevent future diabetes. We have put together a list of FREE diabetes resources in English and Spanish to share with people living with prediabetes and diabetes. Thank you for your advocacy and belief that we can make a difference. Coach Beverly
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
In 1923, the Nobel prize in physiology or medicine was awarded to Frederick Grant Banting and John James Richard MacLeod “for the discovery of insulin”. 100 years later, we celebrate this life saving discovery each year on November 14th, a day designated as World Diabetes Day.
Why do we celebrate World Diabetes Day on November 14th? Please choose the best answer.
Click Here to Test your Knowledge
This course will transform your test anxiety into calm self-confidence and test-taking readiness.
Instructor: Beverly Thomassian RN, MPH, CDCES, has been Board Certified in Advanced Diabetes Management for over 20 years. She is an Associate Clinical Professor at UCSF, a working educator, and a nationally recognized diabetes expert. She has a Master’s Degree in Public Health from UCLA, with a focus on behavioral health and education.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
On October 25th, 1923 the Nobel prize in physiology or medicine was awarded to Frederick Grant Banting and John James Richard MacLeod “for the discovery of insulin”. The discovery was made in 1921 i.e., only two years before, which makes the time period between the detection and this prize one of the shortest in the history of the Nobel Prize.
Dr. Banting was born on November 14, 1891. That is why we celebrate World Diabetes Day on November 14th.

During a hot summer in 1921, Dr. Banting secured space to test out his theory in the University of Toronto. Along with his colleague, Charles Best, and a bare bones lab, they conducted dozens of experiments on dogs, which ultimately led to the discovery of insulin.
Dr. Banting and Charles Best began their experiments ligating the pancreases of dogs, thinking this would prevent destruction by the digestive pancreatic juices, and then isolating the extract from the islet cells. They then processed the extract from the islet cells and injected this extract they called “insulin” into diabetic dogs. According to an audio Interview with Dr. Best, by July 1921, they had 75 positive examples of insulin lowering blood glucose levels in dogs.

In February 1922, doctor Frederick Banting and biochemist John Macleod published their paper on the successful use of a alcohol based pancreatic extract for normalizing blood glucose levels in a human patient.
Here are some photos of the first insulin bottles produced by the University of Toronto and Eli Lilly.
Soon, word of their discovery got out and the race was on to produce enough insulin to treat the flood of type 1 patients arriving in Toronto to receive this miracle injection.
First Children to Receive Insulin

The first patient to receive insulin was a ‘welfare’ case at Toronto General Hospital – no clinical trial structure to say the least. People from Canada/US flooded into Toronto to receive treatment. Banting struggled with the lack of accessibility of insulin – volume needed and issues of purification.
The earliest patients were “selected”, some youths from Canada/US, some soldiers with diabetes (probably because of Banting’s service in the First World War) and then later some select private patients. During this time they were working hard to increase the volume and continue to improve the purification process. Insulin was available for testing in US, namely through Dr. Elliot Joslin in the late summer 1922.
Dr. Banting – Fun and Interesting Facts
Takes a Team
While Best played a critical and important role, credit must also go to Professor Macleod, from the University of Toronto, who provided the lab space, showed Dr. Banting how to operate on dogs, provided his student Best and suggested they switch from a saline to alcohol to purify the ‘extract’. Dr. Macleod also secured the support of JB Collip, the 4th man on the team and the fist person to purify insulin for human use. Best is also known for pushing Banting to return to the research during a particular dark period of failure.
Want to Learn More About the Dr. Banting?
Historical Insulin Powerpoint Slides – here is a collection of some of my favorite powerpoint slides, depicting the discovery of insulin.
Visit Banting House FaceBook Page
November kicks off National Diabetes Month, a time to recognize that over 11% of Americans are living with diabetes and over 35% have prediabetes. Since diabetes results from a combination of genetics plus environment, there is a recognition that social determinants of health play a pivotal role in the development of diabetes and its complications. Through advocacy and education, we can inform individuals on best care for diabetes and support them in taking action to improve the health of their communities to prevent future diabetes. We have put together a list of FREE diabetes resources in English and Spanish to share with people living with prediabetes and diabetes. Thank you for your advocacy and belief that we can make a difference. Coach Beverly
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.

Be a part of our diabetes community while learning about the latest in diabetes care. Plus, Coach Beverly provides an interactive question and answer session at the end of each live webinar.
Join us to get ready to succeed a the CDCES Exam. This course will transform your test anxiety into calm self-confidence and test taking readiness.
We will review sample test questions, and the reasoning behind choosing the right answers.
After registering, you will receive a confirmation email containing information about joining the webinar.
Topics covered include:
Can’t make it live? No worries. We will send post the recorded version to the Online University within 24 hours of the broadcast
Intended Audience: All healthcare professionals & paraprofessionals looking to become CDCES-certified
Instructor: Beverly Thomassian RN, MPH, CDCES, has been Board Certified in Advanced Diabetes Management for over 15 years. She is an Associate Clinical Professor at UCSF, a working educator, and a nationally recognized diabetes expert.
Coach Bev invites you to join this 60-minute webinar that covers gastrointestinal health from top to bottom. Topics include; fatty liver disease diagnosis and treatment, intestinal complications associated with diabetes, keeping the microbiome healthy, and more. Join us to explore the magnificent wonders of diabetes and the gut.
New content and exciting research findings! Join the wonderment as we explore the impact of our GI System on our health.
Topics covered include:
Intended Audience: These courses are knowledge-based activities designed for individuals or groups of diabetes educators, including RNs, RDs, Pharmacists, Nurse Practitioners, Clinical Nurse Specialists, Physician Assistants, and other health care providers interested in enhancing their diabetes and microbiome knowledge
Instructor: Beverly Thomassian RN, MPH, CDCES, BC-ADM is a working diabetes specialist and a nationally recognized diabetes expert.
Enroll in our entire Level 4 | Advanced & Specialty Topic Courses All courses air at 11:30 a.m. (PST)
All hours earned count toward your CDCES Accreditation Information
Can’t make it live? No worries. We will send post the recorded version to the Online University within 24 hours of the broadcast
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
For last week’s practice question, we quizzed participants on the 5 different tongue tastes. 67% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
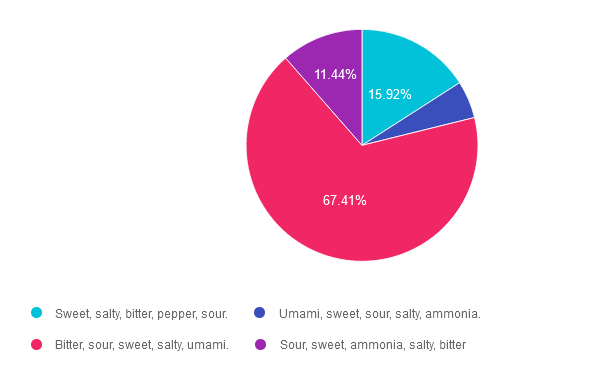
Question: JR thinks that their ability to taste food has diminished recently. They ask you, what are the five confirmed basic tastes of the tongue?
Which of the following lists describes the best answer?
Answer Choices:
If you are thinking about taking the certification exam, this practice test question will set you up for success. Test writers anticipate possible answers based on the details in the question. They will wave those “juicy answers” right under your nose. Your job is to weed through the particulars, pluck out the most important elements and choose the BEST answer.
Answer 1 is incorrect. 15.92% chose this answer. “Sweet, salty, bitter, pepper, sour.” This answer is really close, however there are no specific receptors on the tongue to detect the flavor pepper.
Answer 2 is incorrect. 5.22% of you chose this answer. “Umami, sweet, sour, salty, ammonia.” This answer is really close, however, ammonia is not a confirmed flavor and this list is missing the flavor, bitter.
Answer 3 is correct. About 67.41% of respondents chose this. “Bitter, sour, sweet, salty, umami.” YES, these are the 5 confirmed tastes and one more taste might be added to list, ammonium chloride. According to an article in Neuroscience News, “The tongue’s response to ammonium chloride, a component in some candies, may indicate a sixth basic taste. The study illuminated that OTOP1, a protein receptor that signals sour taste, also responds notably to ammonium chloride.”
Finally, Answer 4 is incorrect. 11.44% chose this answer. “Sour, sweet, ammonia, salty, bitter” This answer is really close, however, ammonia is not a confirmed flavor and this list is missing the flavor, umami.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Coach Bev invites you to join this 60 minute webinar that covers gastrointestinal health from top to bottom. Topics include; fatty liver disease diagnosis and treatment, intestinal complications associated with diabetes, keeping the microbiome healthy, and more. Join us to explore the magnificent wonders of diabetes and the gut.
Can’t make it live? No worries. We will send post the recorded version to the Online University within 24 hours of the broadcast
Instructor: Beverly Thomassian RN, MPH, CDCES, has been Board Certified in Advanced Diabetes Management for over 20 years. She is an Associate Clinical Professor at UCSF, a working educator, and a nationally recognized diabetes expert. She has a Master’s Degree in Public Health from UCLA, with a focus on behavioral health and education.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.

November kicks off National Diabetes Month, a time to recognize that over 11% of Americans are living with diabetes and over 35% have prediabetes. Since diabetes results from a combination of genetics plus environment, there is a recognition that social determinants of health play a pivotal role in the development of diabetes and its complications. We have compiled a list of our favorite FREE diabetes information resources in English and Spanish to empower people with prediabetes and diabetes.
This newsletter also explores why a new sweetener may confuse those who dose insulin based on carb counting. This vital information can help prevent unintended hypoglycemia.
We include a quick primer on new terms that describe liver disease to better reflect the metabolic inflammation and remove the stigma associated with terms like “fatty” and “non-alcoholic.”
Lastly, we welcome Ginger to our team and invite you to test your knowledge with our Question and Rationale of the Week!
Thank you for your advocacy and belief that we can make a difference.
With thanks to all of you,
Coach Beverly and Bryanna
Featured Articles
FREE Webinars & Resources
Upcoming Events – See the complete calendar listing
November kicks off National Diabetes Month, a time to recognize that over 11% of Americans are living with diabetes and over 35% have prediabetes. Since diabetes results from a combination of genetics plus environment, there is a recognition that social determinants of health play a pivotal role in the development of diabetes and its complications. Through advocacy and education, we can inform individuals on best care for diabetes and support them in taking action to improve the health of their communities to prevent future diabetes. We have put together a list of FREE diabetes resources in English and Spanish to share with people living with prediabetes and diabetes. Thank you for your advocacy and belief that we can make a difference. Coach Beverly
November is National Diabetes Month. This month shines a spotlight on the 37 million people living with diabetes and the 96 million with prediabetes. Certain communities are hit harder with diabetes than others due to a combination of genetics and social determinants of health.
Which of the following statements are most accurate?
Click Here to Test your Knowledge
November kicks off National Diabetes Month, a time to recognize that over 11% of Americans are living with diabetes and over 35% have prediabetes. Since diabetes results from a combination of genetics plus environment, there is a recognition that social determinants of health play a pivotal role in the development of diabetes and its complications. Through advocacy and education, we can inform individuals on best care for diabetes and support them in taking action to improve the health of their communities to prevent future diabetes. We have put together a list of FREE diabetes resources in English and Spanish to share with people living with prediabetes and diabetes. Thank you for your advocacy and belief that we can make a difference. Coach Beverly
All hours earned count toward your CDCES Accreditation Information
For last week’s practice question, we quizzed participants on checking for fibrosis & liver elastography. 52% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
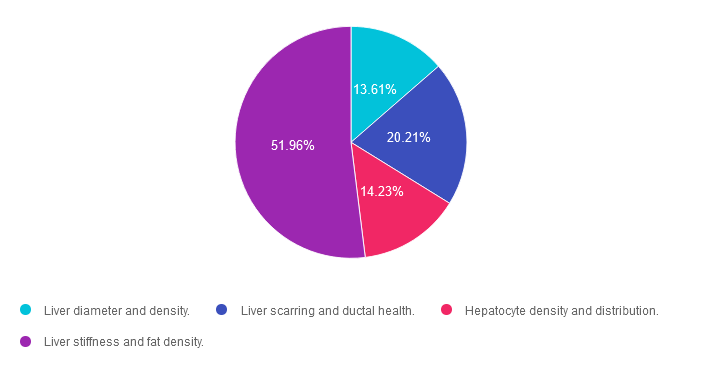
Question: The provider is sending JR for a Liver Elastography or FibroScan test since JR has elevated ALT and AST levels along with an elevated Fib-4 score.
Which of the following are measured during this liver ultrasound procedure?
Answer Choices:
If you are thinking about taking the certification exam, this practice test question will set you up for success. Test writers anticipate possible answers based on the details in the question. They will wave those “juicy answers” right under your nose. Your job is to weed through the particulars, pluck out the most important elements and choose the BEST answer.
Answer 1 is incorrect. 13.61% chose this answer. “Liver diameter and density.” This answer is tempting, but unfortunately, it is not accurate. Liver Elastography or FibroScan test measures for liver stiffness and fat density, two very important findings to quantify liver health.
Answer 2 is incorrect. 20.21% of you chose this answer. “Liver scarring and ductal health.” This answer is also tempting, but not accurate. Liver Elastography or FibroScan test measures for liver stiffness and fat density, two very important findings to quantify liver health.
Answer 3 is incorrect. About 14.23% of respondents chose this. “Hepatocyte density and distribution.” Unfortunately, this tempting answer is not accurate. Liver Elastography or FibroScan test measures for liver stiffness and fat density, two very important findings to quantify liver health.
Finally, Answer 4 is correct. 51.96% chose this answer. “Liver stiffness and fat density.” YES, this is the BEST Answer. This 5-10 minute, non-invasive test, measures liver stiffness or degree of fibrosis (reported as the kPa score) and the amount of fat in the liver (reported as the CAP score). Join our FREE Webinar on Exploring the GI System – From the Gut to the Butt on November 16th to learn more!
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Coach Bev invites you to join this 60 minute webinar that covers gastrointestinal health from top to bottom. Topics include; fatty liver disease diagnosis and treatment, intestinal complications associated with diabetes, keeping the microbiome healthy, and more. Join us to explore the magnificent wonders of diabetes and the gut.
Can’t make it live? No worries. We will send post the recorded version to the Online University within 24 hours of the broadcast
Instructor: Beverly Thomassian RN, MPH, CDCES, has been Board Certified in Advanced Diabetes Management for over 20 years. She is an Associate Clinical Professor at UCSF, a working educator, and a nationally recognized diabetes expert. She has a Master’s Degree in Public Health from UCLA, with a focus on behavioral health and education.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.