Subscribe
eNewsletter
Ready to get certified?
Free CDCES Coach App
eNewsletter
Free CDCES Coach App
Free Med Pocket Cards
By: Beverly Thomassian
Gung Hay Fat Choy.
Every Chinese New Year brings a wave of gratitude for Alex and Ying, who welcomed an akward 14-year-old into their family-style restaurant and made her feel loved and cared for. Their generosity and belief in me left a lasting imprint on my heart.
I invite you to enjoy this excerpt from my recent book Healing through Connection for Healthcare Professionals. Join Coach Beverly for an intimate virtual interview on the writing of this book on Feb. 20 at 11:30am PST.

When I was fourteen and a half, I found refuge in an unexpected place—a small Chinese restaurant tucked between a Kinney Shoe Store and an Italian eatery in a strip mall in the San Fernando Valley. While my home life was unraveling, I was quietly being stitched back together behind the counter at Ying’s Kitchen.
I didn’t know it then, but this restaurant would do more than offer me a paycheck. It would shape my work ethic, show me what being part of a team meant, and serve as a foundation for the healthcare professional I would one day become. In that busy kitchen filled with the scent of onions and sizzling oil, I learned the beauty of hard work—and the profound healing that comes when someone believes in you.
Finding Refuge in Ying’s Kitchen
As the latest in the long line of high school girls, my job was to answer phones, bag the food, ring up the orders, and answer customer questions for $1.25 an hour. Barely a teenager with no restaurant experience, I approached my assigned tasks with a combination of diligence and confusion.
Early on, I stumbled. Anne, a high school senior in charge of training me, told me, in no uncertain terms, that I was “not keeping pace with the training program, and they might let me go.” This awkward coaching session is seared into my brain. It pushed me into high gear, and I became determined to be the best Ying’s Kitchen employee ever! That moment lit a fire in me. I doubled down, became the fastest phone answerer in the West Valley, and soon trained the new hires myself. It was more than pride, it was survival. A sense of belonging, and a safe place to grow.
Beyond being my employers, Alex and Ying looked out for me. Alex asked me about my day at school and practiced Chinese with me. Before closing, he would ask me if I was hungry. My favorites were the pork fried rice and the egg rolls, and on special nights, he would make me moo goo gai pan. During the summer, Alex coached me on the importance of drinking hot water to cool down. He asked me about my boyfriends and made sure I was keeping up with my homework. Best of all, he always smiled, showing his one gold tooth when I walked through the door.
His wife, Ying, only spoke a few words of English, but she had a way of letting me know she saw me. During springtime, she would call me over and take one strand of my hair, wrapping it carefully around a Jasmine flower from her yard. As I walked through my work shift, I could smell the scent of jasmine and know that I had a found family who treasured me.
Post-Traumatic Growth in Practice
In their book What Happened to You, Oprah Winfrey and Dr. Bruce Perry describe how post-traumatic growth can emerge when safe adults and healing relationships interrupt a cycle of pain. I am living proof of that truth.
Working at Ying’s Kitchen didn’t erase the pain of my past, but it gave me the structure, accountability, and connection I needed to believe in a future beyond it. It became the cornerstone of how I eventually built Diabetes Education Services—a company whose mission is rooted in decreasing shame and blame in diabetes care. The resilience, empathy, and grit that carried me through adolescence now fuel my passion for advocating person-centered, trauma-informed healthcare.
What This Means for Healthcare Professionals
As healthcare professionals, we may look for sophisticated solutions to complex human problems. But sometimes, the most transformative interventions are also the simplest: a steady routine, a safe space, and someone who believes in you.
This is especially true for people living with diabetes and other chronic conditions. Many carry unspoken histories of trauma. When we show up with kindness, curiosity, and consistency, we’re not just delivering care—we’re becoming part of someone’s healing journey.
Whether you’re precepting a student, mentoring a colleague, or counseling a patient, consider the ripple effect of your presence. Like Alex and Ying, you might be offering more than a service—you could be anchoring someone in a storm.
From Survival to Service
Looking back, I see how Alex and Ying laid the groundwork for how I lead today. Those years at Ying’s Kitchen profoundly shaped how I built and now manage my company. The lessons of diligence and love became my guiding light, helping me navigate even the roughest waters and steer my ship toward calmer horizons. The discipline I learned behind that counter still guides how I show up—whether teaching a course, writing a book, or sitting with someone in their hardest moment.
While my early life was shaped by adversity, the safe haven of Ying’s Kitchen taught me that healing often begins with being seen. That’s something we can all offer, no matter our title or training.
Sometimes, the most profound lessons in healing don’t come from textbooks—they come from trusted adults, jasmine flowers, and the quiet grace of being loved into wholeness.
Why Join?
Because you deserve a space to rest, reflect, and reconnect — not just with others, but with yourself. Together, we can remind one another of the humanity behind the healthcare, and rediscover the power of connection in healing.
Your presence matters. Your story matters. And we’re honored to walk this journey with you.

JZ is proud of their Time of Range of 89%. You notice their time below range is 7%. JZ uses a rapid-acting insulin pen 4–6 times daily to keep glucose in target range and occasionally increases the glargine dose when evening glucose is elevated.
What is your primary concern?
Gain fresh insights, practical tools, and a deeper understanding of the latest in person-centered diabetes care. Our expert team brings the ADA Standards of Care to life—covering medications, behavior change, technology, and more!
If you’re preparing for the CDCES or BC-ADM exam, this conference, paired with a handful of free bonus courses, serves as the ideal study companion! Plus, this content counts toward the ADA Standards requirements for CDCES Renewal.
With interactive co-teaching, we keep sessions engaging, relevant, and fun.
Let’s learn and grow together!
Course credits through AMA PRA Category 1 Credits™, ACPE, ANCC, and CDR!
Program Objectives:
Upon completion of this activity, participants should be able to:
For last week’s practice question, we quizzed participants on which feature most strongly supports a diagnosis of hyperosmolar hyperglycemic state (HHS) rather than diabetes ketoacidosis (DKA). 59.77% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question

A 32-year-old with newly discovered diabetes is brought to the emergency department with polyuria and lethargy. They have been sleeping more than usual.
Initial labs show:
Based on the following labs, which feature most strongly supports a diagnosis of hyperosmolar hyperglycemic state (HHS) rather than diabetes ketoacidosis (DKA)?
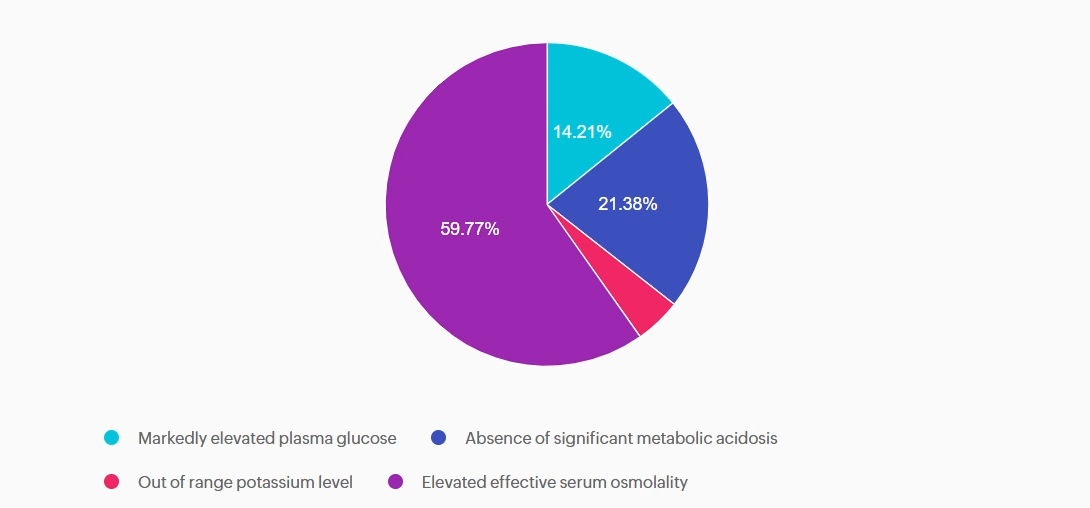
Answer A is incorrect: 14.21% chose this answer, “Markedly elevated plasma glucose.” This answer is tempting, because glucose levels do become markedly elevated with HHS. However, very high glucose levels can also occur with DKA. So this answer doesn’t differentiate between these two hyperglycemic crises.
Answer B is incorrect: 21.38% chose this answer, “Absence of significant metabolic acidosis.” This juicy answer is tempting, since with HHS there is the absence of metabolic acidosis. However, based on the question details, there is no information on pH or ketone status, so we can’t make that assumption.
Answer C is incorrect: 4.64% chose this answer, “Out of range potassium level.” The potassium level of 3.7 is within normal range and doesn’t help us differentiate between HHS and DKA.
Answer D is correct: 59.77% chose this answer, “Elevated effective serum osmolality.” YES, this is the BEST Answer. Great Job! One of the main features of HHS, is increased serum osmolality (greater than 300), due to a combination of elevated glucose and dehydration.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!

Several years ago, I was nominated for Diabetes Educator of the Year. Being put forward by colleagues I deeply respected and admired was profoundly meaningful—and, honestly, a little overwhelming.
The nomination felt like recognition of decades of clinical work, teaching, mentoring, and advocacy for person-centered diabetes care. After submitting the detailed application, I allowed myself to feel hopeful. I imagined sharing my philosophy of judgment-free diabetes care with audiences across the country, offering a message of healing for both healthcare professionals and the people they serve. I even choreographed my walk-up dance in my head, ready to hit the ground running.
Then the email arrived from the board: I hadn’t been selected.
I won’t pretend it didn’t sting. I was devastated. Awards matter because they symbolize recognition; they affirm that your voice has value. When I wasn’t chosen, I found myself sitting with a familiar response that many healthcare professionals have experienced: a complicated mix of disappointment, sharp self-doubt, and the well-worn instinct to minimize the hurt and simply move on.
But once the initial ache softened, something important came into focus. I realized that while awards can amplify a message and provide a platform for it, they are not the source of the message itself. And my message was still burning—undiminished—inside me.
For years, I had been witnessing something under the surface of diabetes care and, more broadly, of healthcare. Earnest and compassionate clinicians were giving their all to provide the best care, but felt they weren’t breaking through or reaching people in ways that led to significant change. Many were questioning their worth, their effectiveness, and even their decision to enter healthcare at all.
I heard it in hallway conferences. In mentoring meetings. In calm moments after lectures when someone would come up to me and say, “I thought it was just me.”
I knew then that the story I was burning to share couldn’t be reduced to a title or an award category. The message I was holding wasn’t just about diabetes education and achieving an A1C of less than 7%. It was about the emotional gift of caring—and the healing strength of connection.
Not winning that award forced a reckoning moment: How could I share my message on a bigger stage?
The answer surprised me with its clarity. Write a book.
I wrote Healing through Connection for Healthcare Professionals because this story matters, award or no award.
The lived experiences and emotional well-being of healthcare professionals matter. You can make a bigger impact in the care you provide by taking inventory of your inner dialogue and beliefs.
Working with people living with diabetes can be filled with connection, joy, and revitalization. By leaving judgment at the door and accepting each other as we are – messy, complicated, and beautiful- you can deepen your connection. The unvoiced grief, the unresolved trauma, the silent resilience, can all have a voice at the table. As a healthcare professional, you deserve healing too.
Not winning hasn’t stopped me from sharing my message; it motivated me to find a different way to share it.
It pushed me to write honestly about:
This book is not a rebuttal to an award committee.
It’s a love letter to healthcare professionals who keep showing up even when recognition is scarce.
Today, when a nurse, pharmacist, dietitian, or physician tells me, “This book made me feel less alone,” I know I chose the right path.
I didn’t win an award, but I found my voice and shared my authentic life story in my book. This book is my commitment transparency with the hopes that it gives you permission to share your truth.
I wrote Healing through Connection so that other healthcare professionals can share their story and create a healing space for themselves and the people in their care.
Because in the end, the greatest legacy is knowing that your message touched the lives of your community and created space for more compassion, for us and those in our care.
Maria, a 52‑year‑old woman with type 2 diabetes for 8 years, attends a follow‑up visit. Her A1C has risen from 7.8% to 9.2% over the past year. She reports feeling “overwhelmed” and says she didn’t want to start the medication her clinician recommended at the last visit. She explains, “I’m scared of side effects, and I feel like needing medication means I failed.”
Which of the following responses is the least appropriate (i.e., the WRONG thing to say) to Maria?

In this course, William H. Polonsky, PhD, CDCES, and Susan Guzman, PhD, examine the powerful role of psychosocial factors in diabetes self-management. Through innovative strategies, participants will learn how to recognize and address common barriers to effective self-care and cardiometabolic medication initiation and maintenance, while fostering respectful, stigma-free clinical encounters.
Through a collaborative and person-centered approach, the course emphasizes communication strategies that enhance motivation, build confidence, and reinforce the value of self-management. Participants will develop skills in diabetes-focused action planning, addressing medication hesitancy, and providing ongoing support and resources to sustain behavior change over time. The goal is to help clinicians make diabetes care more doable, meaningful, and effective for people living with diabetes.
Featured Articles & Announcements ___________________________ |
Webinars & Programs
___________________________
Greetings, healthcare colleagues!
As healthcare professionals, we’re often invited into the most tender moments of people’s lives. In these moments, you may notice your heart swell with compassion, sorrow, or deep gratitude. While this emotional labor is rarely acknowledged, I want you to know: I see it. I hear it.
We recognize the love and care you give each day. Whether it’s an after-hours check-in, helping with food access, volunteering at a community event, or offering a much-needed hug.
This February, let’s take a moment to honor you and the quiet heroism of showing up again and again with an open heart.
In this newsletter issue, I share how not being selected for a diabetes educator award led me to a deeper realization and lit a fire to share my message by writing a book.
We also highlight the power of professional connections and the importance of membership in shaping a healthcare future that reflects our values and vision. A special thanks to Sarah Hormachea, RD, MS, CDCES, BC-ADM for her meaningful insights and guest article contribution.
In celebration of fiber, don’t miss nutrition expert Christine Craig’s article featuring the unsung benefits of fiber plus a high five list.
A tech-focused feature from Dr. Beattie explores how technology and diabetes distress can be linked, along with tools to address it.
You are the heartbeat of health care! Here’s to leading with love this month and every month.
With hearts full of gratitude,
Coach Beverly, Bryanna, Astraea & Katarina
Basic & e-Deluxe CDCES Boot Camp Bundle includes:
CDCES Boot Camp | 50+ CEs
Our CDCES Boot Camp Online Prep Bundle is a comprehensive, high-impact program built specifically for healthcare professionals preparing for the Certified Diabetes Care and Education Specialist (CDCES) exam.
✔ Earn CE/CPE credit through AMA PRA Category 1 Credits™, ACPE, ANCC, and CDR. For more information on accreditation, visit the registration page on our Online Store and click the “Accreditation” tab.
✔ Learn at your pace with expert-led, exam-focused content
✔ Everything you need—organized, practical, and in one place
✔ Perfect for self-directed learners who want complete, person-centered content for clinical practice and exam prep.
✔ Build knowledge, sharpen test-taking skills, and prepare with confidence—on your schedule.
Focused. Flexible. Proven.
Gain fresh insights, practical tools, and a deeper understanding of the latest in person-centered diabetes care. Our expert team brings the ADA Standards of Care to life—covering medications, behavior change, technology, and more!
If you’re renewing your CDCES or BC-ADM certification this live conference, paired with a handful of free bonus courses, serves as the ideal renewal companion!
Join this FREE, pharmacist-focused webinar Co-led by Diana Isaacs, PharmD, BCPS, BC-ADM, BCACP, CDCES, FADCES, FCCP, Endocrinology Clinical Pharmacy Specialist and Coach Beverly Thomassian, RN, MPH, CDCES, BC-ADM.
Leave with a practical roadmap for achieving Certification Diabetes Care and Education Specialist (CDCES) or Board Certification in Advanced Diabetes Management (BC-ADM).

For last week’s practice question, we quizzed participants on recommendations for facilitating positive health behavior change, according to 2026 ADA Standards. 81.75% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
KC has type 2 diabetes, diagnosed 5 years ago. They report low physical activity, frequent sugar-sweetened beverage intake, and high stress related to work. Last A1c was 8.2%. KC reports previous advice to “exercise more and drink less soda,” but reports making minimal changes. They express interest in improving health but feels overwhelmed by where to start.
Which of the following responses best aligns with the 2026 ADA Standards of Care recommendations for facilitating positive health behavior change?
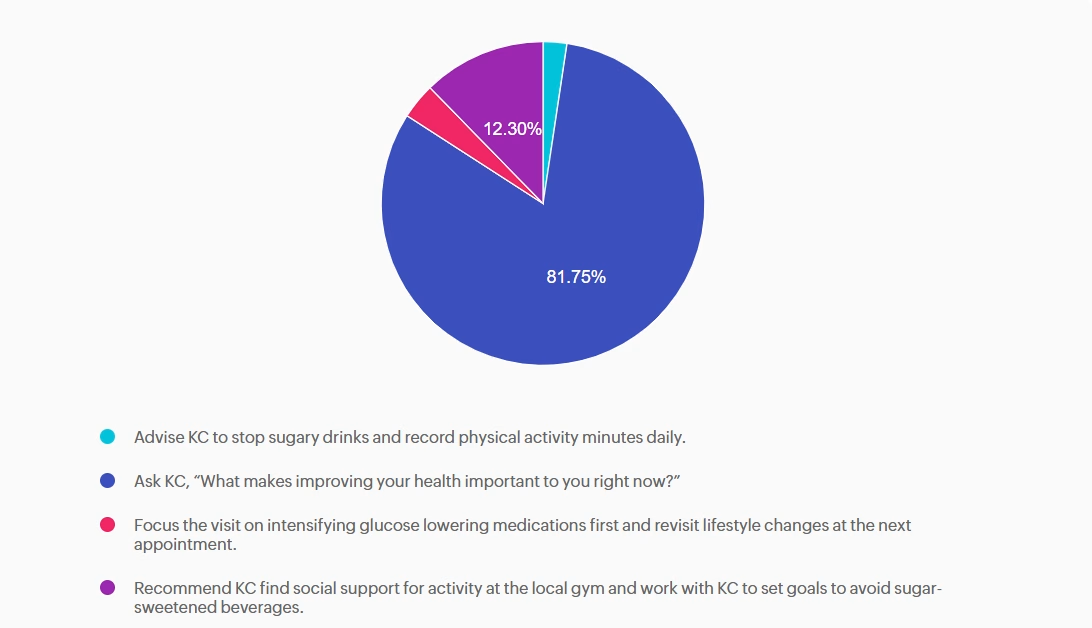
Answer A is incorrect: 2.38% chose this answer, “Advise KC to stop sugary drinks and record physical activity minutes daily.” Although the Standards of Care do recommend avoiding sugar-beverage consumption and increased activity, this answer is prescriptive and not collaborative. Simply telling the patient what to do without assessing motivation or barriers does not align with ADA recommendations for patient-centered behavior change.
Answer B is correct: 81.75% chose this answer, “Ask KC, “What makes improving your health important to you right now?”” This question is an example of a response using the strategy of motivational interviewing (MI). MI is a patient-centered counseling method that explores readiness, addresses ambivalence, helps patients identify barriers to behavior change and encourages confidence while setting goals. The 2026 ADA Standards of Care recommend using MI, along with other strategies, to help individuals with diabetes adopt sustainable lifestyle behaviors, including diet, physical activity, and stress management.
Answer C is incorrect: 3.57% chose this answer, “Focus the visit on intensifying glucose lowering medications first and revisit lifestyle changes at the next appointment.” While medication intensification may be a first step and necessary approach to support KC is their diabetes management, it fails to first address KC’s goals and desires. In addition, the 2026 ADA Standards of Care emphasize integrating behavior change support alongside pharmacologic therapy.
Answer D is incorrect: 12.3% chose this answer, “Recommend KC find social support for activity at the local gym and work with KC to set goals to avoid sugar-sweetened beverages.” While this option does consider strategies of social support and goal-setting it lacks assessment of readiness and barriers and again is a more prescriptive approach vs. collaborative approach.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
A 32-year-old with newly discovered diabetes is brought to the emergency department with polyuria and lethargy. They have been sleeping more than usual.
Initial labs show:
Based on the following labs, which feature most strongly supports a diagnosis of hyperosmolar hyperglycemic state (HHS) rather than diabetes ketoacidosis (DKA)?