Subscribe
eNewsletter
Ready to get certified?
Free CDCES Coach App
eNewsletter
Free CDCES Coach App
Today, Lilly announced caps on out-of-pocket insulin costs at $35 per month and price reductions of 70% for its most commonly prescribed insulins.
In addition, according to their website announcement, Lilly is reducing the list price of insulins:

“The aggressive price cuts we’re announcing today should make a real difference for Americans with diabetes. Because these price cuts will take time for the insurance and pharmacy system to implement, we are taking the additional step to immediately cap out-of-pocket costs for patients who use Lilly insulin and are not covered by the recent Medicare Part D cap” said David A. Ricks, Lilly’s Chair and CEO.
“The American Diabetes Association (ADA) is the leading voice advocating for insulin affordability and is working to ensure that all people with diabetes have access to the care they need. We applaud Eli Lilly for taking the important step to limit cost-sharing for its insulin, and we encourage other insulin manufacturers to do the same. While we have been able to help achieve significant progress on the issue of insulin affordability, including Medicare’s new out-of-pocket cost cap on insulin, state copay caps, and patient assistance developments from insulin manufacturers, we know that our work is not done. We will work to ensure that Eli Lilly’s patient assistance program is benefiting patients as intended and continue the fight so that everyone who needs insulin has access.”? — Charles “Chuck” Henderson, CEO of the American Diabetes Association
Insulin has grown increasingly expensive in recent years despite the introduction of new competition. Many people with diabetes ration their medicines or discontinue them because of the cost. More than 30 million Americans live with diabetes, and more than seven million of them rely on insulin.
Click here to learn more and get involved!
Read our blog here for more info
TR is a health care professional who provides diabetes care and education support. They are interested in providing more person-centered care to the individuals they serve.
Which of the following statements verifies they are on the right track?
Click Here to Test your Knowledge

Whether you are new to diabetes or a seasoned expert, you’ll benefit from this virtual conference with the latest research plus critical content that you can immediately apply to your clinical practice.
If you are seeking a state-of-the-art review of current diabetes care, this course is for you. Our team has been fine-tuning this course for over fifteen years, and we know what you need. This program can also be a great addition to your CDCES or BC-ADM exam study plan.
Group discounts are available!*
Download Course Flyer | Download Schedule
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.

For last week’s practice question, we quizzed participants on the new ADA Standards for lipid management. It was a complicated question and 43% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question:
JR is 67 with type 1 diabetes and was discharged a few months ago after receiving a coronary artery bypass. JR is on insulin pump therapy and a CGM, with a recent A1C of 6.7%. Their blood pressure is 129/78.
Other recent labs include:
JR’s medications include: insulin, atorvastatin 80mg, atenolol 50mg, and aspirin therapy. JR has met with the dietitian and is trying to eat healthfully. They have lost 5 pounds over the past few months.
Based on the 2023 ADA Standards of Care and JR’s history, which of the following is considered best practice?
Answer Choices:
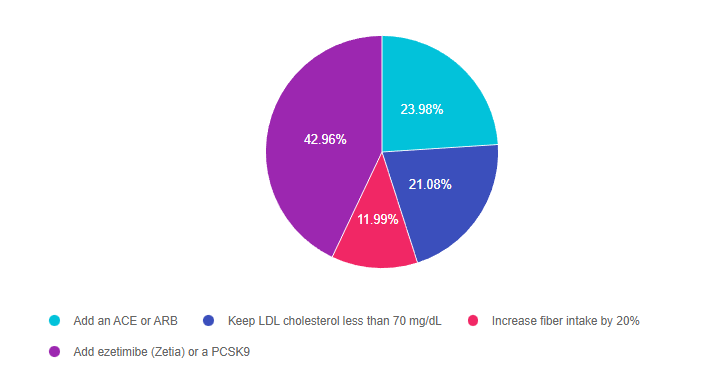
Answer 1 is incorrect. 23.93% chose this answer, “Add an ACE or ARB.” This was a juicy answer. However, since the B/P is on target at less than 130/80 and JR does not have an elevated UACR, adding an ACE or ARB is not indicated at this time.
Answer 2 is incorrect. 21.08% of you chose this answer, “Keep LDL cholesterol less than 70 mg/dL.” Since JR has ASCVD, as evidenced by their need for a coronary artery bypass, the LDL target is less than 55 mg/dL. This new intensified LDL target is based on the 2023 updated guidelines. Read our blog on New Lipid Guidelines here.
Answer 3 is incorrect. 11.99% of respondents chose this answer, “Increase fiber intake by 20%.” While increasing fiber intake is always a good idea, in may not be enough to help JR get their LDL to a target level of less than 55 mg/dl.
Finally, Answer 4 is correct. 42.96% chose this answer, “Add ezetimibe (Zetia) or a PCSK9.” Yes, this is the best answer, GREAT JOB. Since JR has ASCVD, as evidenced by their need for a coronary artery bypass, the LDL target is less than 55 mg/dL. Since they are already on max dose of atorvastatin at 80mg, the ADA Guidelines recommend adding an additional agent, either ezetimibe (Zetia) or a PCSK9 to further lower the LDL to reach a target of less than 55 mg/dL. Download Lipid Medication Cheat Sheet Here
Thank you so much for reading this “Rationale of the Week”. For more information on this topic, we encourage you to Read our blog on New Lipid Guidelines and Download Lipid Medication Cheat Sheet Here. We also invite you to join our Online Courses and Virtual DiabetesEd Training Program.
Whether you are new to diabetes or a seasoned expert, you’ll benefit from this virtual conference with the latest research plus critical content that you can immediately apply to your clinical practice.
If you are seeking a state-of-the-art review of current diabetes care, this course is for you. Our team has been fine-tuning this course for over fifteen years, and we know what you need. This program can also be a great addition to your CDCES or BC-ADM exam study plan.
Group discounts are available!*
Download Course Flyer | Download Schedule
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
With the approval of Tzield (teplizumab-mzwv), an anti-CD3 monoclonal antibody, we can now offer children 8 years and older an opportunity to delay the progression to type 1 diabetes for up to two years or longer and improve beta cell function.
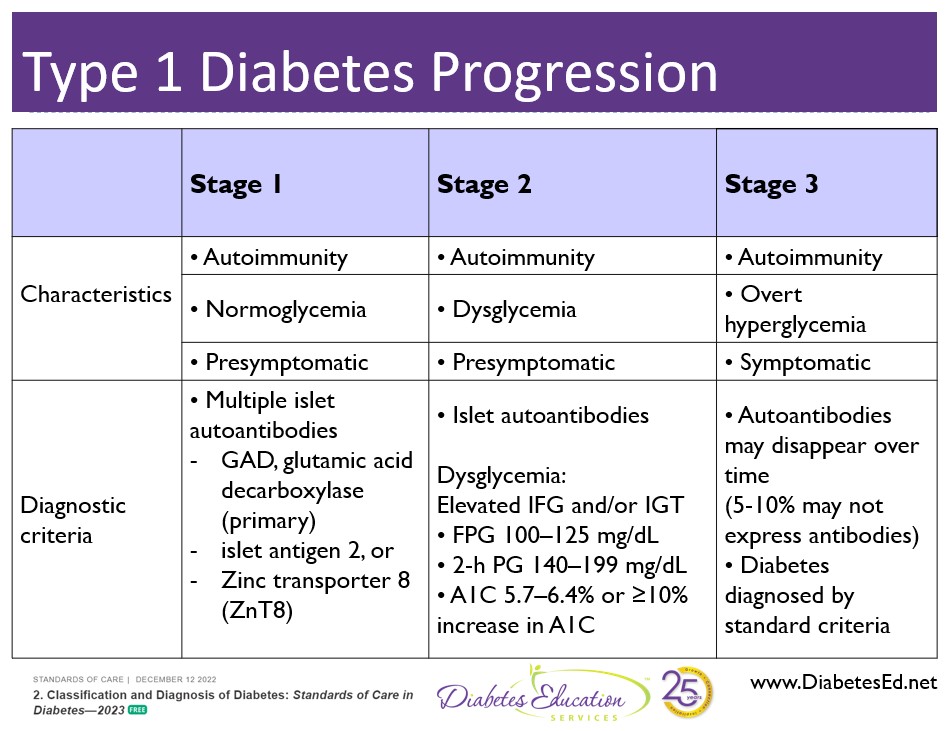
Teplizumab is the first disease-modifying therapy that impedes the progression of type 1 diabetes by binding to the surface of T cells to dampen the unwanted immune system response. It can delay the onset of symptomatic stage 3 type 1 diabetes in adults and children 8 years and older with stage 2 type 1 diabetes (see staging chart).
It is administered by intravenous infusion once daily for 14 consecutive days and is expected to cost in the region of $200,000 for the course of treatment.
Teplizumab is indicated for the individual in stage 2 type 1 diabetes, or for those with two or more islet autoantibodies and abnormal glycemia but still asymptomatic. People with stage 2 type 1 diabetes, have a nearly 100% lifetime risk of progression to clinical (stage 3) type 1 diabetes and a 75% risk of developing the condition within 5 years.
Results from a landmark clinical type 1 prevention trial conducted by TrialNet showed that with a two-week course of teplizumab:
Insulin production in response to glucose was impaired in the participants before they enrolled in the trial. In participants given an inactive placebo, insulin production declined through the first six months of the study. But in those treated with teplizumab, insulin production improved after treatment.
These results suggest that a single course of Teplizumab may provide long-lasting improvement in beta cell function. This, in turn, could delay or even prevent the development of type 1 diabetes in high-risk individuals.
The ability to halt the progression of stage 2 type 1 diabetes from progressing to symptomatic stage 3 diabetes brings the prospect of more wide spread screening for type 1 into sharper focus. Currently, 40-50% of new type 1 diabetes is diagnosed when the individual is admitted to the hospital in a life-threatening hyperglycemic crisis or DKA. Studies suggest, identifying children at risk of future type 1 could avert DKA presentation, saving hundreds of thousands of dollars in hospital costs and allowing for early CD3 monoclonal antibody intervention.
Based on data from Trialnet, even though type 1 diabetes runs in families, 85 – 90% of people don’t have a first-degree relative with type 1 diabetes. That means, broader screening initiatives will be needed to identify those at risk for type 1 and eligible for the benefits of Teplizumab therapy.
The Juvenile Diabetes Research Foundation is working toward a two-pronged screening approach.
This includes testing infants at birth with a genetic risk score combined with antibody screening. With this approach, providers can monitor kids with high genetic risk scores – based on human leukocyte antigen haplotypes, and provide education to family members regarding signs of hyperglycemia. In addition, antibody screening can help identify the stage of autoimmunity and help guide treatment action.
Researchers now have solid proof that immunotherapy can slow the progression of type 1 diabetes. This offers hope to conduct additional studies to extend the benefits of teplizumab, while continuing to test other immune therapies. Keep posted!
Whether you are new to diabetes or a seasoned expert, you’ll benefit from this virtual conference with the latest research plus critical content that you can immediately apply to your clinical practice.
If you are seeking a state-of-the-art review of current diabetes care, this course is for you. Our team has been fine-tuning this course for over fifteen years, and we know what you need. This program can also be a great addition to your CDCES or BC-ADM exam study plan.
Group discounts are available!*
Download Course Flyer | Download Schedule
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
LR experienced gestational diabetes with their third pregnancy and now, at age 41, was just diagnosed with prediabetes. LR’s BMI is 29.3 and she is trying to lose weight.
Based on the 2023 ADA Standards of Care, in addition to providing LR with lifestyle coaching, what other intervention is recommended?
Click Here to Test your Knowledge
Whether you are new to diabetes or a seasoned expert, you’ll benefit from this virtual conference with the latest research plus critical content that you can immediately apply to your clinical practice.
If you are seeking a state-of-the-art review of current diabetes care, this course is for you. Our team has been fine-tuning this course for over fifteen years, and we know what you need. This program can also be a great addition to your CDCES or BC-ADM exam study plan.
Group discounts are available!*
Download Course Flyer | Download Schedule
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
To celebrate, we are spreading the love with a 15% discount off
ALL Online Courses & Virtual Conference from Feb 10-17, 2023. Use code LOVE15 at checkout.
Whether you are new to diabetes or a seasoned expert, you’ll benefit from this virtual conference with the latest research plus critical content that you can immediately apply to your clinical practice.
If you are seeking a state-of-the-art review of current diabetes care, this course is for you. Our team has been fine-tuning this course for over fifteen years, and we know what you need. This program can also be a great addition to your CDCES or BC-ADM exam study plan.
Group discounts are available!*
Download Course Flyer | Download Schedule
“Not just a course – it’s an experience”
Join us to get ready to succeed at the 2023 BC-ADM Exam. This course will transform your test anxiety into calm self-confidence and test-taking readiness. Topics covered include:
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
For last week’s practice question, we quizzed participants on low blood sugars and beer. 38% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question:
JL is 19 and has type 1 diabetes, drinks a “few beers” on the weekends with their college friends. JL uses an insulin pump, but mostly relies of fingerstick checks to monitor blood sugars. According to their log, JL experienced a few low blood glucose levels the past weekend of 62, 49, and 51.
Based on the ADA Standards, what is the most important recommendation for JL?
Answer Choices:
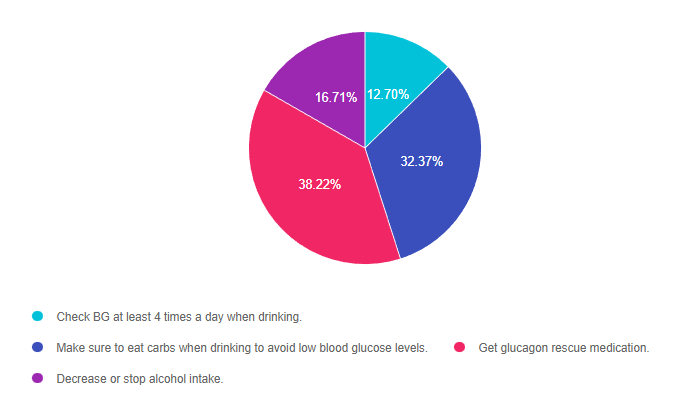
Answer 1 is incorrect. 12.70% chose this answer, “Check BG at least 4 times a day when drinking.” This is a juicy answer. Although monitoring will help JL detect low blood sugars, it doesn’t necessarily translate into taking action to prevent or treat these frequent bouts of level 2 hypoglycemia.
Answer 2 is incorrect. 32.37% of you chose this answer, “Make sure to eat carbs when drinking to avoid low blood glucose levels.” This is another juicy answer and a solid recommendation. For people with type 1 who experience hypoglycemia when drinking alcohol, eating 15gms of carb along with each alcohol serving can help maintain glucose levels. However, this answer is not based on the ADA Standards of Care.
Answer 3 is correct. 38.22% of respondents chose this answer, “Get glucagon rescue medication.” This is the BEST answer. According to the ADA’s Standard 6 on Glycemic Targets, “6.12 Glucagon should be prescribed for all individuals at increased risk of level 2 or 3 hypoglycemia, so that it is available should it be needed”. JL is experiencing Level 2 hypoglycemia with glucose levels dropping to 49 and 51. (see image from Glucagon PocketCard to right for Hypo Levels). While prevention of hypoglycemia is the long term goal, in the short term we need to make sure JL has access to a glucagon rescue med and that their significant others are trained on how to administer this life saving glucose booster.
Finally, Answer 4 is incorrect. 16.71% chose this answer, “Decrease or stop alcohol intake.” While we might want to have a conversation about alcohol and safety, the ADA Standards allow for 1 alcohol serving a day for women and 2 alcohol servings a day for men. In this situation, we might want to discuss adjusting insulin dosing and carbohydrate intake to prevent future bouts of hypoglycemia. However, for safety sake, JL will need a glucagon rescue med prescribed in case of a severe low blood glucose.
Thank you so much for reading this “Rationale of the Week”. For more information on this topic, we encourage you to join our Online Courses and Virtual DiabetesEd Training Program.

Can’t join all the sessions live? No problem. Your registration guarantees you access to the recorded lectures for a full year.
This bundle is specifically designed for healthcare professionals who are studying for the Board Certified in Advanced Diabetes Management (BC-ADM) or the Certified Diabetes Care and Education Specialist (CDCES) certification exam.
Intended Audience: This library of critical information is designed for individuals or groups of diabetes specialists, including RNs, RDs, Pharmacists, Nurse Practitioners, Clinical Nurse Specialists, Physician Assistants, and other health care providers interested in staying up to date on current practices of care for people with diabetes and preparing for the BC-ADM or the CDCES certification Exam.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
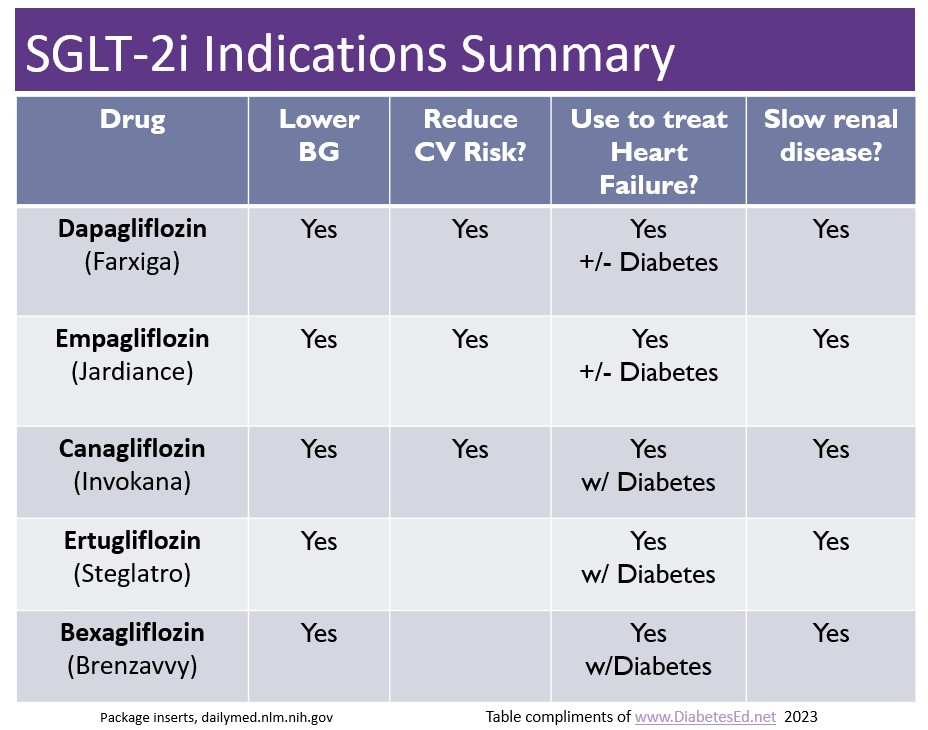
There are now five SGLT-2 Inhibitors that are FDA approved for the treatment of diabetes. The latest one is bexagliflozin (Brenzavvy). We created the chart below to summarize the features and indications of the various SGLT-2i’s. We have also updated our eMedication PocketCard, with this 5th SGLT-2i.
According to TheracosBio, FDA approval of bexagliflozin was based on 23 studies in over 5,000 patients with type 2 diabetes. At a dose of 20mg a day, bexagliflozin decreases A1C by 0.6% to 1.0%, decreases body weight by about 3 kg and drops systolic blood pressure almost 3 mm Hg on average. This treatment can be utilized as a monotherapy or combined with metformin or as an add-on to standard-of-care treatment, including metformin, sulfonylureas, insulin, DPP-IV inhibitors or combinations of all these agents.
GFR cut off of 30: For those with chronic kidney disease, bexagliflozin was safe and well tolerated, however it is not recommended if the eGFR less than 30 mL/min/1.73 m2 and is contraindicated for those on dialysis.
No additional CV benefit data. Bexagliflozin was not found to be superior to placebo in reducing MACE (a composite of cardiovascular death, nonfatal myocardial infarction, nonfatal stroke, and hospitalization for unstable angina). In a trial that included patients with type 2 diabetes and either established CVD or multiple risk factors for CVD, 10.1% (57/567) of the placebo group experienced 1 MACE event vs 7.9% (89/1132) of the bexagliflozin group. However, while the phase 3 data do not indicate any apparent CVD risk, a robust CVD outcomes trial has not been done.
Lower extremity caution: An increased, although not statistically significant, incidence of lower limb amputations was observed among patients treated with bexagliflozin (8.3 vs. 5.1 events per 1,000 patient-years; HR = 1.64, 95% CI, 0.70, 3.82).
Other warnings include genital mycotic infections, DKA, volume depletion, urinary tract infections and urosepsis, similar to other SGLT-2 inhibitors. Read more here.
Download eMedication PocketCard