Renewing your CDCES – Important Updates to Keep in Mind
If you’re one of the many CDCES professionals uncertain about the latest certification renewal requirements, this article will help clarify the process.
We visited the official Certification Board for Diabetes Care and Education Website and did a little detective work and sleuthing, to help clarify the requirements so you can plan for your next renewal cycle.
The most important update is that starting in 2025, CDCESs renewing their certification must meet updated requirements aimed at enhancing diabetes care, education, and ongoing professional development.
These updates involve engaging in at least two CE activities focused on the American Diabetes Association Standard’s and completing a minimum of 75 hours of continuing education (CE) during the renewal period. The aim is to help CDCESs stay up-to-date with evolving standards, thereby improving care and fostering professional development.
New ADA Standard of Care CE Requirements:
CDCESs are required to engage in CE activities—either virtually or in person—twice during their renewal period, focused on the American Diabetes Association’s annual Standards of Care for Diabetes updates.
Both activities can be completed at any time within the renewal cycle. There is no set minimum duration or specific CE credit requirement for these activities. The goal is to ensure CDCESs stay current with evolving standards, which enhances care and supports professional growth.
Activities recognized by CBDCE or its approved providers that pertain to the ADA Standards of Care annual updates will fulfill this obligation.
Documentation and Verification: During renewal, CDCESs will attest to completing these activities. If selected for an audit, they must provide documentation such as CE certificates or conference agendas that verify their participation in relevant sessions. For example, attending a conference on ADA updates will count, provided attendees can verify the specific sessions they attended.
Length of CE Activity: There is no specific number of CEs that one has to earn or minimum length of the activity (30 minutes, 1 hour, 1 day, etc.) for the activity to be able to be used to meet the requirement. The intent for this change is for the CDCES to keep abreast of changes, maintain current knowledge, and enhance the quality of care provided to people with diabetes. It also provides a means for CDCESs to engage in on-going professional development.
Make sure CE Provider is Accredited*. To verify the courses qualify, verify the CE provider is on the List of CBDCE Recognized Providers or has been approved by a Provider on our List of Recognized Providers. Also check that the content of the activities pertains to the annual release of American Diabetes Association’s Standards of Care for Diabetes to ensure that the activity meets the requirement.
*Diabetes Education Services is accredited by the CDR and all CE hours earned can be applied towards renewal.
Optional CE Topics for Renewal that are encouraged but not required:
To reflect recent changes in the specialty, the Board encourages CDCESs to complete continuing education (CE) activities in at least one of the following areas during their renewal cycle (individual or program level):
Educational principles and teaching strategies
Diabetes-related technology
Leadership and strategy (e.g., CQI, change management, program development)
Population health
Diversity, equity, inclusion, and accessibility (e.g., social determinants of health, cultural competency)
These broad topics are designed to support evolving roles in diabetes care and education, ensuring CDCESs stay informed about emerging trends. The Board anticipates that many CDCESs will have already engaged in at least one activity within these areas during their cycle.
During the renewal process, you will be asked if you have completed any CE activities in these areas and to specify the relevant topic. Starting in 2024, this information will be collected at the end of each renewal cycle and presented to the Board to provide insights into the CE content CDCESs are engaging with in their professional roles.
ADA Standards of Care Upcoming Class!
This course, updated annually, is an essential review for anyone in the field of diabetes. Join Coach Beverly as she summarizes the annual updates to the American Diabetes Association’s (ADA) Standard of Medical Care in Diabetes & provides critical teaching points & content for healthcare professionals involved in diabetes care & education
Sign up for Diabetes Blog Bytes – we post weekly Blog Bytes that are informative and FREE! Every week we post one exam practice Question of the Week and Rationale of the Week. Sign up below!
The use of DES products does not guarantee the successful passage of the certification exam. CBDCE and ADCES do not endorse any preparatory or review materials for the CDCES or BC-ADM exams, except for those published by CBDCE & ADCES.
Cheat Sheet Updates – Reflect 2025 ADA Standards
With the publication of the ADA Standards of Care, Coach Beverly embarks on the yearly arduous yet rewarding task of updating our Cheat Sheet Library! As part of the new CDR Accreditation requirements, handouts and slides used as part of the educational courses and resources have to be free of commercial bias and be “logo-free.” The CDR Accrediting Committee ensures that participants attending live or online training programs are presented with content free of conflict of interest, based on evidence, and without brands, ads, and logos.
We are proud to meet the rigorous standards set by the CDR Accreditation Committee and have a 25-year history of intentionally avoiding conflict of interest by not accepting contributions or funds from diabetes-related companies or industries and creating original materials.
Cheat Sheet Updates based on 2025 Standards
ADA Standards of Care 2, Diagnosis and Classification of Diabetes include additional details on screening for type 1 and type 2 diabetes and diabetes in pregnancy, which is captured in our Diagnosis and Classification Cheat Sheet. The diagnostic testing methods and criteria, remained the same as in past years, with an increased emphasis on using A1C as the preferred diagnostic tool, given its accessibility, greater convenience (fasting not required), greater preanalytical stability, and fewer day-to-day perturbations during stress, changes in nutrition, or illness.
Screen for presymptomatic type 1 diabetes, by testing autoantibodies to insulin, GAD, islet antigen 2, or ZnT8 for those with type 1 phenotypic risk (younger age, ketoacidosis, etc.)
For Type 2 diabetes, the suggested screening age for everyone starting at age 35 remained the same as did the BMI cut-off of 23 for Asian Americans and 25 for all others.
Additional risk factors for earlier screening were added and a few were modified from last year. The elevated blood pressure cut-off was decreased from 140/90 to 130/80. In addition to regular screening for those taking antiretroviral medications, ADA added monitoring for hyperglycemia in those taking high-risk medicines (steroids, antipsychotic meds) or a history of pancreatitis and re-checking glucose levels annually or if any signs of hyperglycemia.
In the diabetes and pregnancy section, the ADA more strongly recommended screening all women at the first prenatal visit to help detect undiscovered hyperglycemia and initiate early treatment. Before 15 weeks of gestation, test individuals with risk factors and consider testing all individuals for undiagnosed diabetes at the first prenatal visit using standard diagnostic criteria if not screened preconception.
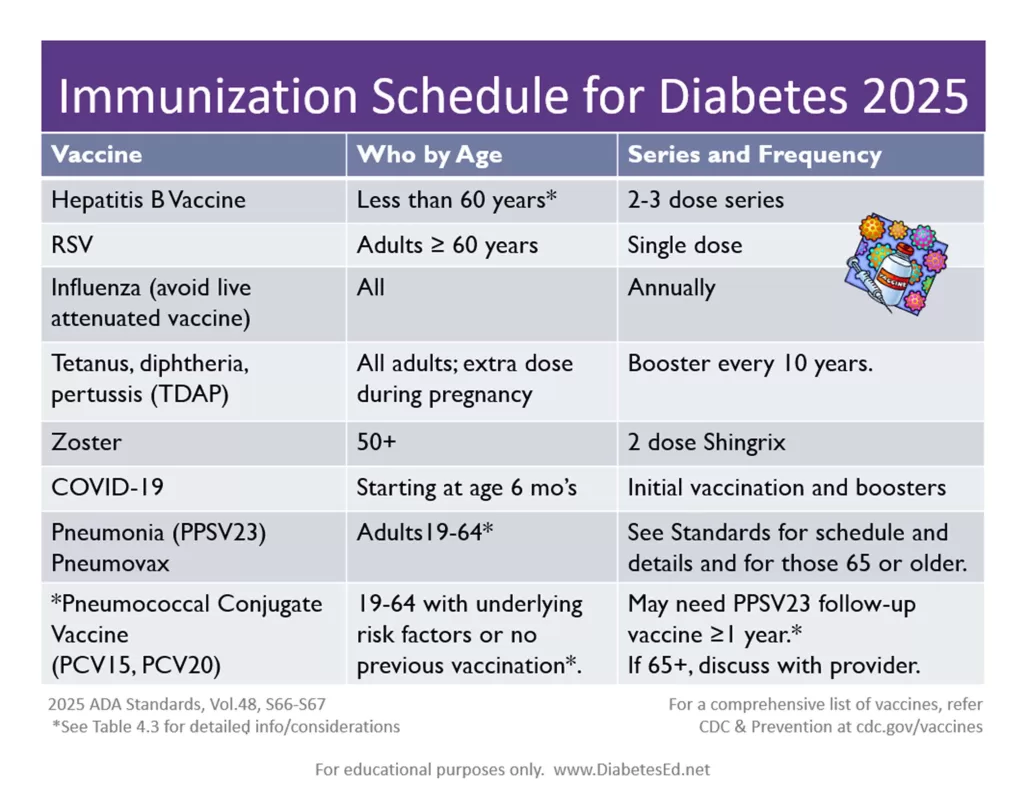
This chart details the types of vaccines, when, and how often they are recommended for people with diabetes. There were two new additions this year. A single RSV dose is recommended for those 60 years and older and the COVID-19 vaccine and boosters are suggested starting at six months of age.
This standard emphasized reminding people with diabetes to avoid the live attenuated influenza vaccine and it included additional clarification on the pneumonia vaccines.
Feel free to download and share these info sheets and share with colleagues and people living with diabetes!
ADA Standards of Care 2024 Webinar Update
Join us live on February 1, 2024, at 11:30 am PST
This course, updated annually, is an essential review for anyone in the field of diabetes. Join Coach Beverly as she summarizes the annual updates to the American Diabetes Association’s (ADA) Standards of Medical Care in Diabetes & provides critical teaching points & content for healthcare professionals involved in diabetes care & education.
Topics:
A review of changes & updates to the annual ADA Standards of Medical Care in Diabetes.
Identification of key elements of the position statement.
Discussion of how diabetes educators can apply this information in their clinical setting.
Can’t make it live? No worries. We will send post the recorded version to the Online University within 24 hours of the broadcast
Instructor: Beverly Thomassian RN, MPH, CDCES, has been Board Certified in Advanced Diabetes Management for over 20 years. She is an Associate Clinical Professor at UCSF, a working educator, and a nationally recognized diabetes expert. She has a Master’s Degree in Public Health from UCLA, with a focus on behavioral health and education.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and our CPEU courses have received Prior Approval* from the Commission of Dietetic Registration (CDR), Provider DI002. Since our CPEU courses received Prior approval* from the CDR, these CPEU courses satisfy the CE requirements for the CDCES /BC-ADM regardless of your profession!
The use of DES products does not guarantee the successful passage of the certification exam. CBDCE and ADCES do not endorse any preparatory or review materials for the CDCES or BC-ADM exams, except for those published by CBDCE & ADCES.
National Diabetes Month – Resources
November kicks off National Diabetes Month
According to the latest CDC Data, over 16% of Americans are living with diabetes and 38% have prediabetes. This means about half of our communities are living with hyperglycemia.
Advocacy and education play essential roles in diabetes care and prevention. By equipping individuals with knowledge about diabetes management, healthy lifestyle choices, and preventative measures, we empower them to take ownership of their health and inspire change within their communities.
Community-centered education can be incredibly powerful—when people feel informed and supported, they’re more likely to make meaningful changes and encourage others to do the same. This creates a ripple effect, fostering healthier communities and potentially reducing the prevalence of diabetes over time.
We have put together a list of FREE Webinars and diabetes resources in English and Spanish to share with people living with prediabetes and diabetes. Thank you for your advocacy and belief that we can make a difference.
FREE Webinars to Celebrate National Diabetes Month
Websites that offer FREE handouts & info on diabetes
ADA’s Diabetes Food Hub – English and Spanish! Web site filled with information on healthy eating and an abundance of delicious recipes.
ADA Resources in Spanish – this newly opened information hub is perfect for those who prefer to learn and read in Spanish.
ADA’s FREE Life with Diabetes Program: ADA’s program includes six digital, printable journeys to teach how to live well with diabetes; a monthly e-newsletter with tips, stories, and more resources; six free issues of the Diabetes Forecast® magazine; access to an online community and local events. (The program is available in both English and Spanish).
ADA’s Risk Quiz: 60-second online risk assessment for type 2 diabetes. ADA created a self-assessment and a version to fill out the assessment for others. There’s also a printable version in English & Spanish that can be distributed to help ascertain risk. This is a great first step in helping individuals consider coming in for an appointment
National Diabetes Education Program is an online library of resources compiled by the NDEP to help provide accurate information and support for people living with prediabetes and diabetes.
Spanish Language Resources: language can be a barrier to adequate and quality care. ADCES has created a number of free downloads for people with diabetes and prediabetes, which have been translated into Spanish.
Type 1 Diabetes Resource Page – Includes is a list of helpful online resources for Type 1 Diabetes. It include sites for national organizations like the American Diabetes Association (ADA), sites for diabetes interest groups, and other participant organizations that provide helpful diabetes tips and opportunities to join online groups.
Tech Resources
DiabetesWisePro for Clinicians A non-biased web site for health care professionals that has a quick tool to access insurance coverage information, how to order devices, what to include and where to go for support.
DiabetesWiseA non-biased website that helps people with diabetes learn about different diabetes devices and determine the best match for their needs
November 2024 Newsletter | Celebrate Diabetes Month & Embrace Diversity
Happy November,
Nearly 16% of American adults — that’s close to 1 in 6 — now has diabetes, according to the latest data from the CDC. Along with social determinants of health, education seems to matter: While about 20% of Americans with a high school degree have diabetes, the rate falls to 10.7% for people with a college degree.
To help increase awareness, we have compiled a list of our favorite FREE diabetes information resources in English and Spanish to empower people with prediabetes and diabetes to take action.
Did you know dietary choices can improve eye health? While glucose management is essential in reducing the risk of retinopathy, nutritional strategies that reduce glycemic variability, blood pressure, inflammation, and oxidative stress significantly impact retinal health and vision. Read more below.
We are excited to announce the launch of the Diabetes Care Provider Directory, spearheaded by Diversity in Diabetes. This inclusive organization aims to connect individuals with healthcare professionals who want to provide care for people from diverse experiences, fostering a collaborative environment for effective diabetes care.
Lastly, to help everyone feel their best this holiday season, we are sharing our popular handout highlighting Ten Strategies to Survive the Holiday commotion and another info sheet on reframing diabetes distress.
We hope you can join our FREE webinars in celebration of National Diabetes Month. We are sincerely grateful for your ongoing dedication to improving diabetes care.
You’re Invited to Join the Diversity in Diabetes Care Directory
It is with great enthusiasm that I share a transformative initiative: the launch of the Diabetes Care Provider Directory at Diversity in Diabetes.
In a increasingly diverse world, the need for cultural humility in healthcare has never been more critical, particularly for individuals living with diabetes. As we navigate the complexities of diabetes management, we acknowledge that each person’s journey is unique, deeply influenced by their cultural background, personal experiences, and individual needs.
The launch of the Diabetes Care Provider Directory at Diversity in Diabetes aims to connect individuals with healthcare professionals who are excited to connect with people with diverse experiences, fostering a collaborative environment for effective diabetes care.
At Diversity in Diabetes (DiD), the mission is anchored in three foundational pillars: Education, Resources, and Support. These essential elements are thoughtfully curated to meet the unique needs of vulnerable populations, including BIPOC communities, men, LGBTQIA+ individuals, and those aged 65 and older on their diabetes care journey. By focusing on these pillars, Diversity in Diabetes strive to empower individuals with the knowledge and tools they need to manage their health effectively.
About Diversity in Diabetes
Founded in August 2020 by Quisha Umemba and Kacey Creel, Diversity in Diabetes (DiD) is a 501(c)(3) nonprofit organization dedicated to addressing the critical lack of diversity in diabetes care. As the creators of the People of Color Living with Diabetes Summit, Quisha and Kacey have focused on raising awareness, providing education, and developing solutions to combat healthcare inequities and improve health outcomes for individuals and communities of color.
At Diversity in Diabetes (DiD), the organization is dedicated to advocating for greater representation of healthcare professionals in diabetes management. They work diligently to enhance awareness of treatment options specifically for People of Color Living with Diabetes (POCLWD) and promote the effective integration of technology in their care. Additionally, DiD strives to improve access to Diabetes Self-Management Education and Support programs for POCLWD, tirelessly pursuing a more equitable landscape in diabetes care. Their commitment to inclusivity and support aims to empower individuals and communities, fostering an environment where everyone can thrive in their diabetes journey.
The Importance of Culturally Competent Care
Many individuals with diabetes encounter barriers when accessing care that resonates with their personal and cultural realities. Understanding these diverse perspectives is essential for fostering a supportive environment in which patients can thrive.
Diversity in Diabetes aims to bridge this gap by creating a comprehensive directory that connects individuals to healthcare professionals who genuinely understand and respect their unique needs.
Diversity in Diabetes is actively seeking compassionate and dedicated professionals to enrich their directory—healthcare providers, dietitians, endocrinologists, therapists, and others who share a commitment to inclusive care. Here’s why I encourage you to consider joining this important initiative:
Lead the Change in Diabetes Care
By participating in this directory, you will contribute to a network that prioritizes culturally competent care. Your involvement can help create a healthcare environment where every individual feels valued and understood on their journey to managing diabetes.
Increase Your Visibility
Joining the directory allows you to reach a diverse client base actively seeking your expertise. This is an opportunity to connect with those who can benefit greatly from your knowledge and compassion.
Access Valuable Resources
Members of the directory will gain access to a wealth of resources and tools provided by Diversity in Diabetes. These materials will empower you to enhance your practice and deliver the highest quality of care to your patients.
Your Role in This Initiative
As healthcare professionals, we play a crucial role in shaping the experiences of those we serve. Your dedication to understanding and addressing the diverse needs of individuals living with diabetes can have a transformative impact on their health outcomes. By joining the Diabetes Care Provider Directory, you will help ensure that everyone has access to the compassionate, culturally competent care they deserve.
If you are ready to make a meaningful difference and be part of this vital initiative, I encourage you to visit Diversityindiabetes.org/care-directory to learn more and register.
Together, we can foster a more inclusive diabetes care community that uplifts and empowers all individuals. Thank you for your unwavering commitment to improving the lives of those living with diabetes. Diversity in Diabetes (DiD) Team.
Enroll in our Free Webinar: Strategies to Revitalize Your Diabetes
It’s been five year since you passed your exam. Now you are approaching your renewal date, so how do you maintain this hard-earned certification? To help you stay on top of this important process, we’ve gathered some essential updates from the CBDCE website.
This year, the CBDCE published new rules to renew certification which you might have missed. To make sure there are no surprises during your renewal process, here are key considerations from the CBDCE Website that we hope you find helpful!
2025 CDCES Renewal Updates
To promote quality and inclusive diabetes care and education, the CBDCE Board changed the continuing education (CE) content requirements. Certificants will still need to complete 75 CE units over a five year period. However, to make sure CDCES’s stay abreast of the latest standards and promote inclusive care, the Board is now requiring participation in CE courses that provide updates on the ADA Standards of Care at least twice during the individual’s renewal cycle.
Required CE Activities now include ADA Standards Update
This means that starting in 2024, certificants will need to start acquiring these more specific CEs in preparation for 2025 renewal.
According to the CBDCE, to successfully renew their CDCES, applicants must participate in CE activities that are focused on the American Diabetes Association’s Standards of Care for Diabetes* two separate times during your renewal cycle.
In addition, the following CE Activities are encouraged:
If you are renewing your CDCES in 2025 or later by completing 75 CE units over the five-year period, the CBDCE requires that you demonstrate completion of the following type of CE Activities (you can immediately start accumulating these needed CEs). The CBDCE encourages the following CE activities at least once during your renewal cycle:
education principals/teaching strategies
diabetes-related technology;
leadership/strategy (e.g., CQI, change agent, program development);
population health; or
diversity, equity, inclusion, and accessibility (e.g., social determinants of health, cultural competency).
Diabetes Education Services Online University is Here to Help!
Our content incorporates the ADA Standards and Content Requirement The bundles listed below are well-suited for meeting CDCES renewal requirements. Additionally, we refresh our entire content library every year to stay current with the latest ADA Guidelines.
In addition, our DiabetesEd Training Programs cover the ADA Standards of Care with clarity and intention by a trio of experts, including Diana Issacs, PharmD, BC-ADM, CDCES, and FADCES a contributing author to the ADA Standards.
Plus, all of our content incorporates education principles and teaching strategies, with a special emphasis on population health, equity, diversity, and inclusion.
The use of DES products does not guarantee the successful passage of the diabetes certification exams. CBDCE & ADCES does not endorse any preparatory or review materials for the certification exams, except for those published by CBDCE & ADCES.
**To satisfy the requirement for renewal of certification by continuing education for the Certification Board for Diabetes Care & Education (CBDCE), continuing education activities must be applicable to diabetes and approved by a provider on the CBDCE List of Recognized Providers (www.ncbde.org). CBDCE does not approve of continuing education. Diabetes Education Services is accredited/approved by the Commission of Dietetic Registration which is on the list of CBDCE Recognized Providers.
Here's how you can get started right away. Enroll in our ADA Standards of Care Course today!
This course, updated annually, is an essential review for anyone in the field of diabetes. Join Coach Beverly as she summarizes the annual updates to the American Diabetes Association’s (ADA) Standard of Medical Care in Diabetes & provides critical teaching points & content for healthcare professionals involved in diabetes care & education.
Victoza (liraglutide) – First GLP-1 Available as a Generic
Victoza is now available in generic form at a slightly reduced monthly price of $469.60 for a 2-pack and $704.40 for a three-pack. According to the ADA average wholesale price chart, Victoza typically costs around $1,340 for a month’s supply, which is about a 50% reduction in price.
Victoza (liraglutide injection 1.8 mg) is a once-daily GLP-1 injection approved to treat type 2 diabetes. It lowers A1C by about 1%, along with weight loss and reduced risk of cardiovascular events. See our Medication PocketCards for more info.
Generic Victoza, produced by Teva Pharmaceuticals, is the first GLP-1 RA that has gone generic. Victoza’s patent in the US and Europe expired in late 2023, paving the way for companies like Teva to pursue generic versions. Two other generic Victoza options are being developed with a possible December 2024 release date. Once multiple Victoza generics are on the market, the hope is that competition will further reduce prices for people who would benefit from this medication. Patents for newer GLP-1 medications like Ozempic and Wegovy won’t expire until several years later.
Launching this more cost-effective generic Victoza comes as many people with diabetes struggle to access the more popular GLP-1 medications like semaglutide (Ozempic) and dulaglutide (Trulicity). Liraglutide (Victoza) was also approved for weight loss for those without diabetes who met the BMI criteria in 2014 under the brand name Saxenda.
The first generic GLP-1 is a significant milestone in improving access to diabetes drugs. With the launch of additional Victoza generics in 2025 and beyond, prices should continue to fall even further, helping more people access these crucial medications.
Another SGLT-2 Approved for Pediatrics
This month, the FDA approved another SGLT-2i, dapagliflozin (Farxiga), for children under the age of 18. Dapagliflozin and empagliflozin are now both approved for pediatrics starting at the age of 10 diagnosed with type 2 diabetes as an adjunct to diet and exercise to improve glycemic control.
The incidence and prevalence of type 2 diabetes in children and adolescents are increasing globally. In the US, there are nearly 30,000 individuals under the age of 20 living with type 2 diabetes, with 5,300 new cases diagnosed each year, according to the US Centers for Disease Control and Prevention and recent research. Children with type 2 diabetes often experience earlier onset of complications than adults and benefit from interdisciplinary care and social support.
Data from the T2NOW Phase III trial, published in The New England Journal of MedicineEvidence, Farxiga, provided clinically meaningful improvements in glycemia for children and adolescents with type 2 diabetes. The safety results in this pediatric population were consistent with those in adults with T2D. Of course, it is essential to provide education on preventing genital infections and any signs of diabetes ketoacidosis. See our Medication PocketCards
The use of DES products does not guarantee the successful passage of the certification exam. CBDCE and ADCES do not endorse any preparatory or review materials for the CDCES or BC-ADM exams, except for those published by CBDCE & ADCES.
Get Ready – How to Prepare for Natural Disasters
As we enter fire and storm season, it’s always a good idea to think ahead and be prepared for disaster. For people living with diabetes, a “diabetes kit” is an important part of emergency preparedness. We are excited to share a few getting ready checklists and resources that we think are really helpful.
For any emergency scenario, it’s important to have an emergency preparedness plan that includes a meeting point, an exit route, a “get-away” bag, and communication strategies. Identify and inform the people who will be included in the emergency plan ahead of time and make sure everyone clearly knows what to do and what action to take.
An easy way to get started is to download the Checklist and Plan created by the Diabetes Disaster Response Coalition. We have also created a Disaster Checklist Word document that you can download and customize for yourselves. These checklists can help you start the conversation and commit the details to paper.
Disaster can happen in a moments notice. It’s important to plan ahead and be ready, especially for people living with diabetes.
Here are a few helpful resources for ourselves and our community:
Resources for People with Diabetes
General information from the Diabetes Disaster Response Coalition (DDRC) on preparedness for people living with diabetes.
Have an Emergency Diabetes Plan and Kit Ready: DDRC’s Diabetes Plan and Kit checklist includes helpful steps to take in preparation for disaster. The checklist details needed supplies and information that should be written down and kept in a waterproof container for emergency situations where is can be found by a health care provider to make informed emergency treatment decisions.
Stay Updated: Visit Breakthrough Type 1 Disaster Relief Resources and Diabetes Disaster Response Coalition includes information on how to access medical support, shelters, and open pharmacies during times of disaster.
Individuals with diabetes who need help: Call 1-800-DIABETES (800-342-2383). The American Diabetes Association Center For Information is open, MON.-FRI. 9 a.m. TO 7 p.m. ET. Representatives are regularly updated with information on how to access medical support, shelters, pharmacies, and more.
American Red Cross Shelters: Contact the American Red Cross directly at 1-800-RED-CROSS.
Resource For Health Care Providers:
Insulin Supply Hotline: During a disaster, call the emergency diabetes supply hotline 314-INSULIN (314-467-8546) if you know of diabetes supply shortages in your community (i.e. shelter, community center). The hotline is for health care providers only.
Diabetes Disaster Response Coalition (DRRC). If a disaster hits, people with diabetes may need emergency supplies and help fast. Please visit the DRRC website if you are a diabetes health care provider and are requesting information about diabetes supplies during disasters.
In addition to the items listed below, make sure to pack hand sanitizer, wipes, and masks due to the current pandemic. Also, bring your own pillow and bedding in case you need to spend time in a shelter.
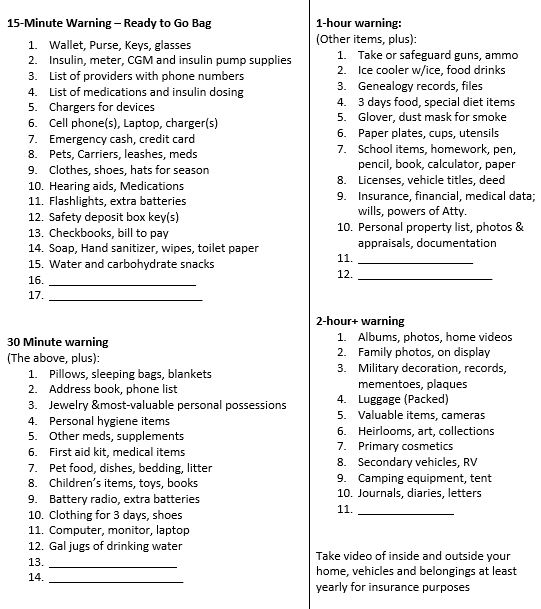
Download, Share, and Personalize this Emergency Checklist
Emergency Evacuation-Items to Gather for People with Diabetes We thought this list was a helpful way to prioritize what items to grab given different time frame limitations. We found it online and customized it for people with diabetes. It is available in Word or PDF. Thank you for sharing with your colleagues and community.
Emergency List that you can Customize in a Word Doc
Emergency List as a PDF to print out
Emergency List that you can Customize in a Word Doc
Emergency List as a PDF to print out
1-800-DIABETES (800-342-2383) is an excellent referral resource for people with diabetes to call toll-free for updates on accessing medical support during an emergency.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.

 If you’re one of the many CDCES professionals uncertain about the latest certification renewal requirements, this article will help clarify the process.
If you’re one of the many CDCES professionals uncertain about the latest certification renewal requirements, this article will help clarify the process.