
Subscribe
eNewsletter
Ready to get certified?
Free CDCES Coach App
eNewsletter
Free CDCES Coach App
Free Med Pocket Cards

JR is hospitalized with influenza. They have a history of prediabetes but now have persistent glucose readings between 220–260 mg/dL and are started on basal-bolus insulin.
JR is upset and states: “I’ve been reading that pancreatic parasites can cause of diabetes. No one is treating my infection.”
What is the BEST response?
Get exam-ready with confidence.
Course credits through AMA PRA Category 1 Credits™, ACPE, ANCC, and CDR!
Full accreditation details are available on the registration page
Our CDCES Boot Camp Online Prep Bundle is a comprehensive, high-impact program built specifically for healthcare professionals preparing for the Certified Diabetes Care and Education Specialist (CDCES) exam who want to level up their clinical knowledge and skills.

This evidence-based study bundle is a comprehensive BC-ADM Boot Camp designed for advanced-level healthcare professionals preparing for the Board Certified in Advanced Diabetes Management (BC-ADM) exam and will also provide you with state-of-the-art information to level up your clinical practice.
Join national experts including Dr. Diana Isaacs (Cleveland Clinic), Beverly Thomassian (30+ years of experience), and Christine Craig for high-impact, virtual learning—no travel required.
✔ Learn from National Experts — Anywhere
Get the same expert-level instruction you’d receive in person, delivered live to your home or office.
✔ Interactive & Flexible
Walk away with tools you can apply immediately in clinical practice or while preparing for CDCES or BC-ADM exams. From insulin dosing protocols to behavior change strategies that work in the real world—this content bridges theory and practice.
Enjoy this poem by Coach Bev that summarizes steps to achieve diabetes certification success in 53 seconds!
Get Ready for Diabetes Certification Success
___________________
We know you’re excited to take your certification exam — and we want you to walk in feeling confident, calm, and completely prepared. 🖥️ To make sure you have the content you need, we have moved up the dates for our Level 3 and Level 4 live courses by a few months. We will complete Level 3 live course updates by April 30th and Level 4 updates will wrap up by June 20th. 📆Download Boot Camp flyers for complete date listings. |
We are always keeping you in mind! All of our accredited content is person-focused and evidence-based. Plus, we make sure you have fun and feel engaged during our programs. |
To prepare for your CDCES, we recommend enrolling in our CDCES Boot Camp, which includes:
✔ Level 1 – Fundamentals (2026) Recorded and ready for immediate viewing. Build your foundation and master the core concepts.
✔ Level 2 – ADA Standards Intensive 2026. Live throughout February and March. We break down the Standards of Care so they actually make sense — and stick.
✔ Level 3 – Final Exam Prep Mastery. Originally scheduled for June… but you told us that was too late. We heard you.
Level 3 now begins in March and runs through April 30th — giving you earlier access to focused exam mastery and test-taking strategy.
⬇️Download CDCES Boot Camp Flyer with New 2026 Dates!
This is your CDCES step-by-step path: Level 1 → Level 2 → Level 3. From fundamentals to final confidence 🏆.
To prepare for your BC-ADM, we recommend enrolling in our BC-ADM Boot Camp, which includes:
✔ Level 2 – ADA Standards Intensive 2026.
✔ Level 3 – Final Exam Prep Mastery. Begins in March and runs through April 30th.
✔ Level 4 – Final Exam Prep Mastery. Begins in April and runs through June 20th.
⬇️ Download BC-ADM Boot Camp Flyer with New 2026 Dates
This is your BC-ADM step-by-step path: Level 2 → Level 3 → Level 4. From Standards to advanced to final confidence 🏆.
You are the reason that diabetes care gets better.
We appreciate your hard work, advocacy, and the care you give every day!
💜Coach Beverly, Bryanna, Astraea, and Katarina
Get exam-ready with confidence.
Course credits through AMA PRA Category 1 Credits™, ACPE, ANCC, and CDR!
Full accreditation details are available on the registration page
Our CDCES Boot Camp Online Prep Bundle is a comprehensive, high-impact program built specifically for healthcare professionals preparing for the Certified Diabetes Care and Education Specialist (CDCES) exam who want to level up their clinical knowledge and skills.
This evidence-based study bundle is a comprehensive BC-ADM Boot Camp designed for advanced-level healthcare professionals preparing for the Board Certified in Advanced Diabetes Management (BC-ADM) exam and will also provide you with state-of-the-art information to level up your clinical practice.
Join national experts including Dr. Diana Isaacs (Cleveland Clinic), Beverly Thomassian (30+ years of experience), and Christine Craig for high-impact, virtual learning—no travel required.
✔ Learn from National Experts — Anywhere
Get the same expert-level instruction you’d receive in person, delivered live to your home or office.
✔ Interactive & Flexible
Walk away with tools you can apply immediately in clinical practice or while preparing for CDCES or BC-ADM exams. From insulin dosing protocols to behavior change strategies that work in the real world—this content bridges theory & practice.
For last week’s practice question, we quizzed participants on TIR (Time of Range) of 89% , and what is your concern. 62.2% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question

JZ is proud of their Time of Range of 89%. You notice their time below range is 7%. JZ uses a rapid-acting insulin pen 4–6 times daily to keep glucose in target range and occasionally increases the glargine dose when evening glucose is elevated.
What is your primary concern?
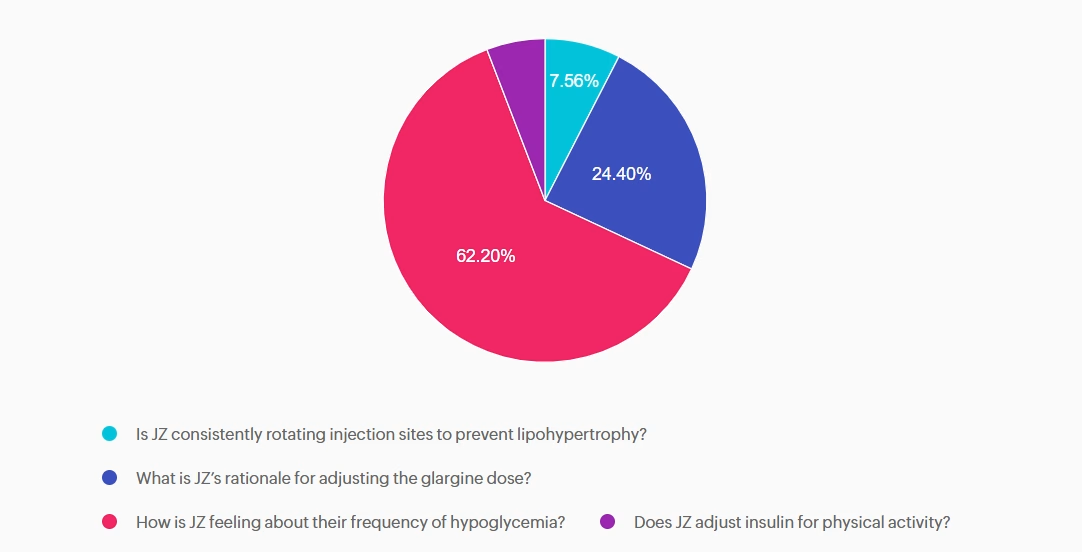
Answer A is incorrect: 7.56% chose this answer, “Is JZ consistently rotating injection sites to prevent lipohypertrophy?” Injection site rotation is important for preventing lipohypertrophy and absorption variability, but not the most immediate safety risk.
Answer B is incorrect: 24.4% chose this answer, “What is JZ’s rationale for adjusting the glargine dose?” Basal insulin is generally titrated based on overnight and fasting blood glucose levels, not reactively based on the evening glucose. This is clinically relevant, but still secondary to hypoglycemia risk.
Answer C is correct: 62.2% chose this answer, “How is JZ feeling about their frequency of hypoglycemia?” Since JZ is experiencing hypoglycemia more than the target below target range of 5%, we want to explore their feelings around their diabetes and diabetes distress.
Answer D is incorrect: 5.84% chose this answer, “Does JZ adjust insulin for physical activity?” Adjusting insulin for exercise is essential for self-management, yet the first priority is identifying whether dangerous lows are occurring.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Course credits through AMA PRA Category 1 Credits™, ACPE, ANCC, and CDR!
Get exam-ready with confidence.
Our CDCES Boot Camp Online Prep Bundle is a comprehensive, high-impact program built specifically for healthcare professionals preparing for the Certified Diabetes Care and Education Specialist (CDCES) exam who want to level up their clinical knowledge and skills.
✔ Basic CDCES Boot Camp – From the fundamentals, to the ADA standards, to test strategies and exam mastery! This complete exam prep includes Levels 1, 2, and 3 (30+ courses, 50+ CEs, 400+ practice questions)
✔ e-Deluxe CDCES Boot Camp – Everything in Basic PLUS the [e-Book] ADCES Certification Review Guide | 6th Edition (475+ practice questions)
✔ Mini CDCES Boot Camp – Accelerated program for experienced healthcare professionals (skips Level 1 | Diabetes Fundamentals, includes Levels 2 & 3, 20+ courses, 40+ CEs, 325+ practice questions).
Course credits through AMA PRA Category 1 Credits™, ACPE, ANCC, and CDR!
Get exam-ready with confidence.
Our comprehensive BC-ADM Online Study Programs are specifically designed for advanced level healthcare professionals who are studying for the Board Certified in Advanced Diabetes Management (BC-ADM) exam.
✔ Basic BC-ADM Boot Camp – Complete exam prep includes Levels 2, 3, and 4 (30+ courses, 50+ CEs, 400+ practice questions)
✔ e-Deluxe BC-ADM Boot Camp – Everything in Basic PLUS the ADCES Certification Review Guide E-book with an additional 475+ practice questions.
Gain fresh insights, practical tools, and a deeper understanding of the latest in person-centered diabetes care. Our expert team brings the ADA Standards of Care to life—covering medications, behavior change, technology, and more!
The world of diabetes technology is advancing at a record pace. There is no doubt that technology intends to make life with diabetes a bit easier. In the United States, over 50% of adults living with diabetes have experienced some level of diabetes distress.¹ The impact of diabetes technology on mental well-being is complicated. Diabetes technology, including insulin pumps, continuous glucose monitors (CGMs), and connected insulin pens, can either lessen or aggravate diabetes distress.

The American Diabetes Association (ADA) defines diabetes distress as “significant negative psychological reactions related to emotional burdens and worries specific to an individual’s experience in having to manage a demanding chronic condition such as diabetes.”.² Diabetes distress is a natural reaction to the daily burden of managing diabetes. Signs of diabetes distress can include avoiding blood glucose monitoring, omitting medications, and struggling to achieve personal hemoglobin A1c targets.
The ADA recommends screening for diabetes distress at least annually. More frequent screening is recommended if clients are not meeting treatment goals, develop diabetes-related complications, and during times of life transitions.²
To access these validated diabetes distress screening tools in English and Spanish, I encourage you to visit this helpful website, DiabetesDistress.org
Let’s explore how diabetes technology can have a positive impact on diabetes distress.
✅ CGMs: With current CGMs, fewer fingerstick readings are needed to make treatment decisions. CGMs provide information on blood glucose trends and impending hyperglycemia or hypoglycemia, creating more peace of mind.
✅ Record Keeping: Various forms of diabetes technology can log blood glucose values, insulin doses, site changes, and total daily doses of insulin. This eliminates the need for clients to worry about detailed record-keeping.
✅ Automated Insulin Delivery: Automated insulin pumps can decrease decision fatigue by making automated adjustments to both basal and correction insulin doses. This approach to insulin delivery can also benefit individuals with an active lifestyle. Utilizing wearable insulin delivery devices and algorithms can reduce the mental burden of diabetes self-management.
✅ Connectivity: Remote data sharing supports communication with parents, caregivers, and friends to create a diabetes support team. Connectivity with healthcare providers enhances communication with the care team, allowing adjustments to treatment plans between clinic visits.
✅ Empowerment: The data trends can empower individuals living with diabetes to take control and gain confidence in making and evaluating medication and lifestyle adjustments in response to changes in glycemic control.
As diabetes healthcare professionals, it is important to understand how diabetes technology can negatively impact diabetes distress.
❌ Information Overload: Diabetes technology generates an enormous amount of data. This can cause distress by constantly feeling the need to monitor glucose trends and numbers throughout the day and night, leading to feelings of anxiety and overwhelm.
❌ Alarms: Alarms on diabetes technology are rooted in safety, but for those living with these devices, this can lead to diabetes distress. Alarms can disrupt sleep or bring unwanted attention from others in public. Erroneous alarms for hyperglycemia or hypoglycemia can cause stress, frustration, and alarm fatigue.
❌ Perfectionism: Diabetes technology provides a continuous insight into glycemic control, which for some can create a need for perfection. Some clients feel like they fail when they don’t reach their time-in-range goal each day.
❌ Physical Impact: Wearable devices not only carry a psychological burden but can also cause physical distress. Skin irritation and allergic reactions to adhesives cause physical pain and embarrassment. Those who wish to keep diabetes private, wearing a CGM, insulin pump, or other wearable device that puts diabetes on display, causing distress.
❌ Technical issues: Losing connectivity with CGMs or an AID system can cause frustration and make it challenging to achieve optimal glycemic control. Insurance coverage, prior authorizations, out-of-pocket costs, and access to supplies for diabetes technology can all contribute to or worsen diabetes distress.
The 7A’s Framework provides a useful interview tool when assessing for Diabetes Distress:
Here are some other actionable tips you can use to help those with diabetes distress:
Alexander, D.S., Saelee, R., Betsy Rodriguez, B., Koyama, A. K., Cheng, Y. J., Tang, S., Rutkowski, R. E., & Bullard, K. M. (2025). Diabetes distress among US adults with diagnosed diabetes, 2021. Preventing Chronic Disease: Public Health Research, Practice, and Policy, 22(E07), 1-7. https://www.cdc.gov/pcd/issues/2025/24_0287.htm#:~:text=Among%20US%20adults%20with%20diabetes%2C%20an%20estimated%201.6%20million%20(6.6,income%20compared%20with%20their%20counterparts.
Gain fresh insights, practical tools, and a deeper understanding of the latest in person-centered diabetes care. Our expert team brings the ADA Standards of Care to life—covering medications, behavior change, technology, and more!
After the initial assessment JM is scheduled for an individual visit instead of a group DSMES class.
According to Medicare guidelines, which of the following would NOT justify providing individual DSMES instead of group DSMES?
Course credits through AMA PRA Category 1 Credits™, ACPE, ANCC, and CDR!
Get exam-ready with confidence.
Our CDCES Boot Camp Online Prep Bundle is a comprehensive, high-impact program built specifically for healthcare professionals preparing for the Certified Diabetes Care and Education Specialist (CDCES) exam who want to level-up their clinical knowledge and skills.
✔ Learn at your pace with expert-led, exam-focused content
✔ Everything you need—organized, practical, and in one place
✔ Perfect for self-directed learners who want complete, person-centered content for clinical practice and exam prep.
✔ Build knowledge, sharpen test-taking skills, and prepare with confidence—on your schedule.
Focused. Flexible. Proven.
Basic & e-Deluxe CDCES Boot Camp Bundle Includes:
Course credits through AMA PRA Category 1 Credits™, ACPE, ANCC, and CDR!
Get exam-ready with confidence.
Our comprehensive BC-ADM Online Study Programs are specifically designed for healthcare professionals who are studying for the Board Certified in Advanced Diabetes Management (BC-ADM) exam.
✔ Learn at your pace with expert-led, exam-focused content
✔ Everything you need—organized, practical, and in one place
✔ Perfect for self-directed learners who want complete, person-centered content for clinical practice and exam prep.
✔ Build knowledge, sharpen test-taking skills, and prepare with confidence—on your schedule.
Focused. Flexible. Proven.
Basic & e-Deluxe BC-ADM Boot Camp Bundle include:
Gain fresh insights, practical tools, and a deeper understanding of the latest in person-centered diabetes care. Our expert team brings the ADA Standards of Care to life—covering medications, behavior change, technology, and more!

Announcements
___________________
Healing through Connection for Healthcare Professionals is available in:
Like me, I am sure you have experienced moments of intense frustration when you wanted to scream or give up!
Maybe you had to show up when you were emotionally spent and felt like you had nothing else to give.
I see you and I celebrate you—the hardworking healthcare professional who shows up day after day with heart and courage. In my book, Healing through Connection, I honor your journey and share strategies to help you care for your own well-being as you care for others.
Join a Virtual Conversation and Interview with Coach Bev on Feb 20th at 11:30am PST to delve into the healing power of creative endeavors.
If you can’t make the interview, enjoy this excerpt from Chapter 6, that dives into the Healing Power of Self-Expression and encourages you to dive into your creativity for healing, rejuvenation, and pure JOY.
Even if you can only commit to engaging creativity for a few minutes or half an hour a week, it makes a difference. Stop thinking about all the reasons you can’t do it, and instead, listen to that internal hum, get in the metaphorical car, turn on the ignition, and drive.
Within you lives a quiet, creative spark waiting for attention and care. When you tend to it, you renew your capacity to show up with presence, compassion, and strength, for yourself and for those in your care.
Healing through Connection is both a reminder and a roadmap; an invitation to care for yourself with the same compassion you offer others. It provides a rare perspective on mutual healing.
As we heal ourselves, we expand our capacity to help others with healing. Within the pages of this book, you’ll find a toolbox for exploring your truth, tapping into your emotions, and cultivating creativity. Together, we’ll explore the often-overlooked connection between your own lived experiences and those of the individuals in your care.
Continue reading to discover how making time for creative expression might offer you some unexpected benefits and opportunities for joy!
Did you know that Nobel Prize recipients are nearly three times more likely to engage in creative hobbies than their scientific counterparts?
Theoretical physicist Albert Einstein often played the violin when he encountered challenges in his theoretical work. He believed that music helped him think creatively and tap into his subconscious, enabling breakthroughs such as the theory of relativity.
Marie Curie, a two-time Nobel laureate for physics in 1903 and chemistry in 1911, went for frequent walks in the countryside, which allowed her to reflect and rejuvenate. These moments of tranquility likely helped her maintain focus during the grueling work of isolating radioactive elements.
It’s because they’re simply more open to having hobbies. They are more open to novel experiences and often turn to their creative endeavors when working through challenges. These seemingly unrelated scientific pursuits and personal hobbies can open doors for scientists to crosspollinate ideas across different fields, enabling them to gain fresh perspectives and uncover new insights.
Now, you may not be working toward securing the title of a Nobel laureate. Still, you might be interested in learning the secrets of expanding your mind, creating new connections, and better integrating the two sides of your brain hemispheres to provide better care or nurture your inner life.
You may be wondering how having an artistic hobby or winning a Nobel Prize in science relates to excelling as a diabetes specialist or healthcare professional. As a healthcare professional, you have likely lived through difficult experiences or witnessed profound suffering firsthand.
Plenty of science supports the idea that engaging in creative pursuits offers an outlet to express complex emotions that are not accessible through words alone.
The act of playing an instrument, taking an art class, exploring nature, or playing the bongo drums may provide a gateway to address unrequited trauma or pain, helping you to become more fully aware and present with your feelings. Did you have a childhood or adult hobby you loved doing? One that made you lose track of time as you entered the zone referred to as “flow”? Have you given yourself permission to make time for that hobby and lose yourself in that creative process?
You may want to take a ceramics or writing class, join the local choir, or start a band. Perhaps you found an old camera and want to learn more about photography or realized you’re good at painting. It can be hard to start as a beginner and potentially look silly or unskilled.
Here’s my advice: Let go of those sky-high expectations. No one expects you to paint like Monet in your first art class.
My motto is, if something makes me uncomfortable, I know I’m in the right place—because that’s where growth happens.
I encourage you to take that leap of faith and tolerate the momentary discomfort for long-term gain. It gets better, and before you know it, you will blossom in ways you never expected.
Download this worksheet to explore 20 creative endeavors that may spark inspiration within you. You may already be practicing some of these—or perhaps you have new ideas to add. Wonderful—keep going!
As a dance teacher for the past twenty years who can still balance a sword on her head, I am reminded every day that it is never too late to rediscover your joy.
Coach Beverly is honored to invite you to this special gathering and intimate conversation. During this virtual book launch, a special guest interviewer will join Coach Bev for a heartfelt conversation about why this book matters now and the real stories from clinical practice that inspired it.
Coach Bev will also share the personal journey of writing Healing through Connection and how she discovered her voice along the way. We will conclude with an interactive question-and-answer session and allow time for connection.
Come celebrate connection, healing, and the power of story as we honor the shared human experience at the heart of healthcare.
Thank you for YOUR support and commitment to promoting healing and connection every day!
For last week’s practice question, we quizzed participants on which of the following responses is the least appropriate (i.e., the WRONG thing to say) to Maria. 58.54% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Maria, a 52‑year‑old woman with type 2 diabetes for 8 years, attends a follow‑up visit. Her A1C has risen from 7.8% to 9.2% over the past year. She reports feeling “overwhelmed” and says she didn’t want to start the medication her clinician recommended at the last visit. She explains, “I’m scared of side effects, and I feel like needing medication means I failed.”
Which of the following responses is the least appropriate (i.e., the WRONG thing to say) to Maria?
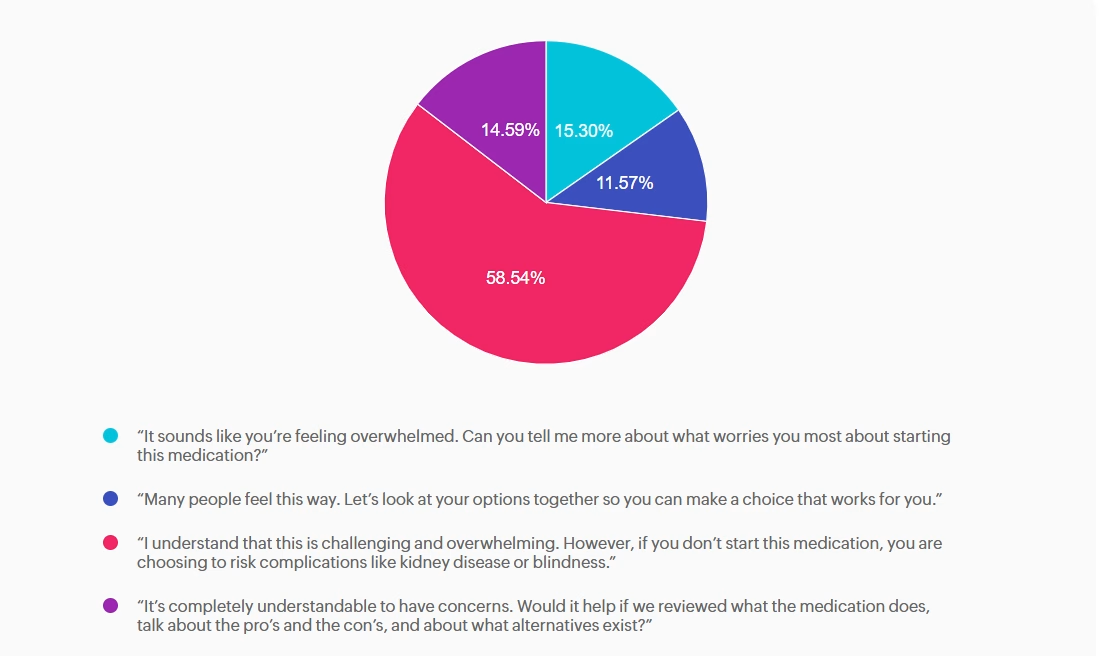
Answer A is incorrect: 15.3% chose this answer,“ It sounds like you’re feeling overwhelmed. Can you tell me more about what worries you most about starting this medication?” Appropriate — Person centered, exploratory. This response uses reflective listening and invites the patient to share her concerns. It aligns with ADA Standards of Care recommendations for collaborative communication and supports assessment of diabetes distress.
Answer B is incorrect: 11.57% chose this answer, “Many people feel this way. Let’s look at your options together so you can make a choice that works for you.” Appropriate — Normalizes feelings and supports shared decision making. This option reduces stigma by acknowledging that many people experience similar emotions. It reinforces autonomy and partnership, which are core components of effective diabetes self management support.
Answer C is correct: 58.54% chose this answer, “I understand that this is challenging and overwhelming. However, if you don’t start this medication, you are choosing to risk complications like kidney disease or blindness.” Incorrect — Stigmatizing, blaming, and fear based. This statement uses threat based language (“you are choosing to risk complications…”) and implies personal failure. It increases shame, undermines trust, and can worsen diabetes distress. It does not incorporate person first language or collaborative care or help identify barriers and personalized solutions. Oh, and it probably won’t be very successful!
Answer D is incorrect: 14.59% chose this answer, “It’s completely understandable to have concerns. Would it help if we reviewed what the medication does, talk about the pro’s and the con’s, and about what alternatives exist?” Appropriate — Validates concerns and offers. Information without pressure. This response acknowledges the patient’s emotions and provides an opening for education and shared exploration of options. It supports autonomy and reduces the sense of failure associated with medication use.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!

In this course, William H. Polonsky, PhD, CDCES, and Susan Guzman, PhD, examine the powerful role of psychosocial factors in diabetes self-management. Through innovative strategies, participants will learn how to recognize and address common barriers to effective self-care and cardiometabolic medication initiation and maintenance, while fostering respectful, stigma-free clinical encounters.
Through a collaborative and person-centered approach, the course emphasizes communication strategies that enhance motivation, build confidence, and reinforce the value of self-management. Participants will develop skills in diabetes-focused action planning, addressing medication hesitancy, and providing ongoing support and resources to sustain behavior change over time. The goal is to help clinicians make diabetes care more doable, meaningful, and effective for people living with diabetes.

Dietary fiber is a complex carbohydrate and bioactive food compound that has an important role in diabetes management and cardiometabolic health. High-fiber dietary patterns are associated with a lower risk of type 2 diabetes, cardiovascular disease, obesity, gastrointestinal disorders, and certain cancers. ¹,²
In individuals with diabetes, fiber-rich eating patterns have been shown to improve glycemia, reduce postprandial glucose excursions, and improve lipid profiles. ¹ A recent meta-analysis found that for individuals with type 1 diabetes, a high- fiber diet not only supports A1c reduction but is also associated with reduced hypoglycemia risk due to its role in slowing digestion and absorption. ³ Despite this evidence most adults fail to meet recommended fiber intake guidelines, presenting an opportunity for nutrition interventions.
The Dietary Reference Intake (DRI) for fiber, established by the Institute of Medicine, along with the 2026 ADA Standards of Care ¹ , recommends 14 grams of fiber per 1,000 Calories, corresponding to an Adequate Intake of approximately 25–38 grams per day depending on age, gender, and energy needs. 4 Higher-fiber dietary patterns greater than 35 grams per day ³ and up to 50 grams per day 1 may provide additional glycemic benefits for individuals with diabetes.
Both the 2020–2025 and 2025–2030 Dietary Guidelines for Americans 5 emphasize fruits, vegetables, whole grains, and legumes as primary fiber sources; however, the recommended portions of these food groups differ between guidelines. The newly released 2025–2030 guidelines place greater emphasis on overall dietary patterns and whole-food sources, with reduced total grain servings, increased emphasis on legumes, and a prioritization of reduced processed foods rather than focusing on fiber as an isolated nutrient.
However, the Scientific Report of the guidelines does reference an optimal fiber intake range of 25–29 grams per day. ² Aligning with ADA Standards of Care, the focus shifts from individual nutrients to overall eating patterns, supporting health professionals to encourage food choices that help individuals meet evidence-based guidelines for fiber recommendations.
Despite serving-size guidance and scientific evidence on the benefits of fiber, average intake in the United States remains far below recommendations. Fewer than 5-7% of adults meet daily fiber requirements. 5 Disparities in intakes among groups have grown over time, with data from the 2017–2018 USDA Economic Research Service showing that, within Hispanic populations, fiber consumption was highest at about 9 grams per 1,000 Calories, compared with
7.7 grams per 1,000 Calories among non-Hispanic White individuals, and 7.0 grams per 1,000 Calories among Black individuals 6 .
Although the amount varies across groups, most individuals reach only 58% of the daily fiber recommendations. Inadequate intake stems from not only food preferences but tolerance, food cost and access, time constraints, nutrition literacy, as well as, other social determinants of health. To help the U.S. population meet fiber goals, practical strategies consider not only culturally relevant nutrition interventions but food assistance programs, systems planning, and community resources that improve access to fiber-rich foods.
Therapeutically, the type of fiber matters, with insoluble or soluble providing different health benefits. Insoluble fiber creates bulk within the stool and can promote bowel regularity and reduces risk of certain cancers. Whereas, soluble fiber forms a viscous gel in the gastrointestinal tract and provides metabolic benefits, including reduced postprandial glucose responses and lower cholesterol levels. 7
While not specific to type, understanding fiber claims on food labels is a practical entry point for guiding individuals toward higher-fiber food choices. According to FDA labeling regulations, foods may be labeled a “good source” of fiber if they provide 10–19% of the Daily Value per serving (≥3 grams), while an “excellent source” of fiber provides greater than or equal to 20% of the Daily Value per serving (≥5 grams). 8
Additionally, the FDA has approved the use of “will reduce the risk of coronary heart disease” health claims
on food packaging due the cardioprotective effects of high soluble fibers β-glucan (found in oats and barley) and psyllium. 9 Emphasizing dietary patterns, food quality assessment, label literacy, and considerations for additional functional fiber supplementation can support individuals with diabetes to make informed food choices and shifts in their intake.
Practical strategies to promote higher fiber intake are outlined in the 2026 ADA Standards of Care¹ (Check out Nutrition Behaviors to Encourage ¹ within section 5: Facilitating Positive Health Behaviors and Well-being to Improve Health Outcomes) and can be reinforced through simple, actionable “High-Five for Fiber” tips.
These tips are a catchy way to encourage health behaviors that may help individuals gradually add fiber (slow addition improves gut tolerance) to meet daily recommendations. Ideas can include having individuals choose at least one “high- fiber, excellent source” daily (which has more than 5 g fiber per serving), discover high soluble fiber foods, strive for five, or more, servings from vegetables and/or fruits each day, and/or “take five” to plan meals that include whole grains, fruits, vegetables, legumes, and/or nuts and seeds each week. These tips encourage choice, helping individuals find foods that fit their personal preferences, affordability, cultural traditions, and lifestyles ¹ while supporting sustainable, health-promoting dietary patterns.
References:
Focused. Flexible. Proven.
Basic & e-Deluxe CDCES Boot Camp Bundle Includes:
Course credits through AMA PRA Category 1 Credits™, ACPE, ANCC, and CDR!
Get exam-ready with confidence.
Our CDCES Boot Camp Online Prep Bundle is a comprehensive, high-impact program built specifically for healthcare professionals preparing for the Certified Diabetes Care and Education Specialist (CDCES) exam who want to level-up their clinical knowledge and skills.
✔ Learn at your pace with expert-led, exam-focused content
✔ Everything you need—organized, practical, and in one place
✔ Perfect for self-directed learners who want complete, person-centered content for clinical practice and exam prep.
✔ Build knowledge, sharpen test-taking skills, and prepare with confidence—on your schedule.
