
Subscribe
eNewsletter
Ready to get certified?
Free CDCES Coach App
eNewsletter
Free CDCES Coach App
Free Med Pocket Cards
For last week’s practice question, we quizzed participants on ADCES 7 Self-Care Behaviors. 71% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it by clicking here.

When providing Diabetes Self-Management Education (DSME), which of the following list includes the ADCES 7 Self-Care Behaviors?

Answer A is incorrect. 8.94% chose this answer, “Healthy Eating, Being Active, Insulin Adjustment.” This answer is so close. The 7 ADCES Self-Care Behaviors include Healthy Coping, Healthy Eating, Being Active, Taking Medication, Monitoring, Reducing Risk, Problem Solving. Insulin Adjustment is just one component of Taking Medication.
Answer B is correct. 71.95% of you chose this answer, “Monitoring, Problem Solving, Healthy Coping.” Great JOB! This answer is the best answer. The 7 ADCES Self-Care Behaviors include Healthy Coping, Healthy Eating, Being Active, Taking Medication, Monitoring, Reducing Risk, Problem Solving. This great info to be familiar with for any upcoming certification exam in your future!
Answer C is incorrect. About 10.57% of respondents chose this: “Reducing Risks, Being Active, Social Support.” This answer is so close. The 7 ADCES Self-Care Behaviors include Healthy Coping, Healthy Eating, Being Active, Taking Medication, Monitoring, Reducing Risk, Problem Solving. Social Support falls under the category of Healthy Coping and is not it’s own category.
Finally, Answer D is incorrect. 8.54% chose this answer, “Problem Solving, Reducing Risk, Positive Self-Attitude.” Another juicy answer. The 7 ADCES Self-Care Behaviors include Healthy Coping, Healthy Eating, Being Active, Taking Medication, Monitoring, Reducing Risk, Problem Solving. Positive Self-Attitude might fall under the category of Healthy Coping, but is not it’s own category.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Get exam-ready with confidence.
Course credits through AMA PRA Category 1 Credits™, ACPE, ANCC, and CDR!
Full accreditation details are available on the registration page
Our CDCES Boot Camp Online Prep Bundle is a comprehensive, high-impact program built specifically for healthcare professionals preparing for the Certified Diabetes Care and Education Specialist (CDCES) exam who want to level up their clinical knowledge and skills.

This evidence-based study bundle is a comprehensive BC-ADM Boot Camp designed for advanced-level healthcare professionals preparing for the Board Certified in Advanced Diabetes Management (BC-ADM) exam and will also provide you with state-of-the-art information to level up your clinical practice.
Join national experts including Dr. Diana Isaacs (Cleveland Clinic), Beverly Thomassian (30+ years of experience), and Christine Craig for high-impact, virtual learning—no travel required.
✔ Learn from National Experts — Anywhere
Get the same expert-level instruction you’d receive in person, delivered live to your home or office.
✔ 1-year Access
Every year, National Nurses Week invites us to pause and honor a profession rooted in compassion, resilience, and an unwavering commitment to care.
This Nurses Week, I encourage you to take a moment to appreciate a nursing colleague, friend or family member. Let them know how their care and compassion has made a difference in your life!
As I reflect on my 40 years as a nurse, I feel both humbled and energized by the extraordinary legacy we carry forward. Nursing is not just a career—it is a calling shaped by human connection, scientific curiosity, and the courage to show up, again and again, for people in their most vulnerable moments.

The history of nursing is rich with pioneers who transformed care through both innovation and heart. Florence Nightingale is often recognized as the founder of modern nursing, bringing sanitation and data-driven care to the forefront. But beyond her statistics and systems, she modeled something deeper—the importance of presence. That legacy continues today in every nurse who sits at the bedside, listens without judgment, and advocates fiercely for those in their care.
The observance recognizes the critical role of nurses in patient care, research, leadership, and education. It raises public awareness of the challenges nurses face, such as staffing shortages and workplace stress – and promotes professional pride and public gratitude. The ANA and partner bodies like the American Association of Critical-Care Nurses host webinars, award ceremonies, and advocacy events to spotlight the profession’s impact
Today, nurses represent the largest group of healthcare professionals specializing in diabetes. Nearly half (46%) of those who hold a CDCES credential are nurses. That’s not just a statistic—it’s a reflection of the profound impact nurses have in shaping how diabetes care is delivered, understood, and experienced every day.
In the world of diabetes care, nurses have been at the center of transformation. From the early days of checking urine glucose to administering pork and beef insulin to today’s advanced technologies, nurses have led the way. As early adopters of continuous glucose monitoring and automated insulin delivery systems, nurses have bridged the gap between complex science and real-life application. We are educators, coaches, and translators—helping people make sense of numbers, medications, and daily decisions that can feel overwhelming.
What makes diabetes nursing uniquely powerful, is the ongoing contact nurses often maintain with individuals over a lifetime. Diabetes doesn’t take a day off, and neither does the emotional weight that often accompanies it. In my work, I’ve learned that the most meaningful breakthroughs don’t come from adjusting a medication or starting a CGM, they come from creating a space where someone feels seen, heard, and supported.
Over the decades, I’ve witnessed incredible advancements in diabetes care—new medications, smarter devices, and more personalized approaches. Nurses, along with their colleagues, are often the steady thread in a fragmented healthcare system. We are the ones who notice subtle changes, ask deeper questions, and advocate when something doesn’t feel right. In diabetes care, this might mean recognizing patterns in glucose trends, addressing social determinants of health, or simply acknowledging the burnout a person feels after years of self-management. These moments matter more than we often realize.
As I reflect on my journey, from bedside nursing to education, from rural clinics to national stages – I am continually reminded that our greatest impact comes not from having all the answers, but from presence. The simple act of sitting with someone, validating their experience, and walking alongside them can be profoundly healing – for them and for us. This mutual growth is at the heart of sustainable, meaningful care.
In hospitals, clinics, schools, and beyond – you show up at every hour of the day and night, bringing skill, compassion, and unwavering dedication. You give of yourselves in ways both seen and unseen, helping others heal, receive comfort, and feel cared for in their most vulnerable moments.
National Nurses Week offers us a moment to pause and honor your service and a profession grounded in compassion, resilience, and an unwavering commitment to showing up for others. Thank YOU!
Coach Beverly, RN and author of Healing through Connection for Healthcare Professionals!
Get exam-ready with confidence.
Course credits through AMA PRA Category 1 Credits™, ACPE, ANCC, and CDR!
Full accreditation details are available on the registration page
Our CDCES Boot Camp Online Prep Bundle is a comprehensive, high-impact program built specifically for healthcare professionals preparing for the Certified Diabetes Care and Education Specialist (CDCES) exam who want to level up their clinical knowledge and skills.
This evidence-based study bundle is a comprehensive BC-ADM Boot Camp designed for advanced-level healthcare professionals preparing for the Board Certified in Advanced Diabetes Management (BC-ADM) exam and will also provide you with state-of-the-art information to level up your clinical practice.
Join national experts including Dr. Diana Isaacs (Cleveland Clinic), Beverly Thomassian (30+ years of experience), and Christine Craig for high-impact, virtual learning—no travel required.
✔ Learn from National Experts — Anywhere
Get the same expert-level instruction you’d receive in person, delivered live to your home or office.
✔ 1-year Access

A 45 year old man with type 2 diabetes is referred to a CDCES with a persistently elevated A1c (9.4%). He has missed multiple follow-up appointments and reports inconsistent medication use.
During the visit, he shares that he recently lost his job, is staying intermittently with friends, and often skips meals due to limited food access. He reports feeling “constantly stressed” and “burned out” with diabetes management.
A Diabetes Distress Scale (DDS) score indicates moderate distress, and a PHQ-9 score is 4 (minimal depressive symptoms). He denies suicidal ideation.
Which of the following is the most appropriate next step for the CDCES?
Get exam-ready with confidence.
Course credits through AMA PRA Category 1 Credits™, ACPE, ANCC, and CDR!
Full accreditation details are available on the registration page
Our CDCES Boot Camp Online Prep Bundle is a comprehensive, high-impact program built specifically for healthcare professionals preparing for the Certified Diabetes Care and Education Specialist (CDCES) exam who want to level up their clinical knowledge and skills.

This evidence-based study bundle is a comprehensive BC-ADM Boot Camp designed for advanced-level healthcare professionals preparing for the Board Certified in Advanced Diabetes Management (BC-ADM) exam and will also provide you with state-of-the-art information to level up your clinical practice.
Join national experts including Dr. Diana Isaacs (Cleveland Clinic), Beverly Thomassian (30+ years of experience), and Christine Craig for high-impact, virtual learning—no travel required.
✔ Learn from National Experts — Anywhere
Get the same expert-level instruction you’d receive in person, delivered live to your home or office.
✔ 1-year Access
For last week’s practice question, we quizzed participants on how much protein is recommended. 73% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it by clicking here.
AR is a 63-year-old with type 1 diabetes and mild hypertension. Their GFR is 41 mL/min/1.73m² and UACR is 312 mg/g and their BMI is 24. The provider asks you to instruct AR on a low-protein diet, since AR is in stage 3 CKD. What is your best response?

Answer A is incorrect. 16.88% chose this answer, “Agree to provide education for AR low protein (0.6 -0.8 g/kg/day) to slow kidney disease progression.” This answer is incorrect. Very low-protein diets (<0.6 g/kg/day) have not consistently shown additional renal benefit and may increase the risk of malnutrition, sarcopenia, and frailty, especially in older adults like AR (age 63).
Answer B is correct. 73.05% of you chose this answer, “Reframe and suggest protein intake of about 0.8 g/kg/day as supported by ADA guidelines.” This answer is correct. GREAT Job! People with stage 3 CKD need adequate plant-based or animal protein intake to maintain muscle mass and optimize health and well-being.
Answer C is incorrect. About 2.52% of respondents chose this: “Suggest AR eliminates most protein sources and focus primarily on fiber, carbohydrates and fats.” This answer is incorrect. Since people with diabetes need to consume adequate amounts of either plant-based on animal protein (~0.8 g/kg/day) to maintain muscle mass and optimize health.
Finally, Answer D is incorrect. 7.56% chose this answer, “Reinforce that a protein intake of 1.3 g/kg/day is warranted to prevent sarcopenia and maintain muscle mass.” This answer is incorrect. Higher protein intake (>1.3 g/kg/day) may increase intraglomerular pressure and albuminuria, potentially accelerating kidney decline.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Join national experts including Dr. Diana Isaacs (Cleveland Clinic), Beverly Thomassian (30+ years of experience), and Christine Craig for high-impact, virtual learning—no travel required.
✔ Learn from National Experts — Anywhere
Get the same expert-level instruction you’d receive in person, delivered live to your home or office.
✔ Interactive & Flexible
Get exam-ready with confidence.
Course credits through AMA PRA Category 1 Credits™, ACPE, ANCC, and CDR!
Full accreditation details are available on the registration page
Our CDCES Boot Camp Online Prep Bundle is a comprehensive, high-impact program built specifically for healthcare professionals preparing for the Certified Diabetes Care and Education Specialist (CDCES) exam who want to level up their clinical knowledge and skills.
This evidence-based study bundle is a comprehensive BC-ADM Boot Camp designed for advanced-level healthcare professionals preparing for the Board Certified in Advanced Diabetes Management (BC-ADM) exam and will also provide you with state-of-the-art information to level up your clinical practice.
Cardiovascular disease remains the leading cause of mortality in individuals with both type 1 and type 2 diabetes, emphasizing the importance of risk reduction.
The current Standards of Care in Diabetes from the American Diabetes Association (ADA) recommend comprehensive risk reduction through screening, pharmacologic therapy to achieve individualized blood pressure and lipid goals, and lifestyle interventions focused on diet and physical activity.
The 2026 Dyslipidemia Guideline from the American College of Cardiology and the American Heart Association (ACC/AHA), together with guidance from multiple professional societies, provides updated recommendations for assessing cardiovascular risk assessment and treatment.
Both guidelines emphasize the importance of screening (with new additions within the ACC/AHA guidelines), pharmacologic treatment for primary and secondary prevention and highlight lifestyle management to reduce atherosclerotic cardiovascular disease (ASCVD).
The 2026 ADA Standards of Care recommend individualized medical nutrition therapy (MNT) based on an individual’s eating patterns, preferences, age, comorbidities, treatment plan, and metabolic goals.1 Recommended patterns include Mediterranean-like diet, Dietary Approaches to Stop Hypertension (DASH), and plant-based approaches, all of which are associated with reduced ASCVD risk.
Key strategies include increasing plant-based proteins, reducing saturated fat (replacing it with monounsaturated and polyunsaturated fats), increasing dietary omega-3 fatty acids, increasing fiber rich carbohydrates (particularly soluble fiber), and increasing plant stanols or sterols.1 Limited research exists regarding ASCVD prevention specifically for individuals living with type 1 diabetes, so most recommendations are extrapolated from type 2 diabetes research, including dietary approaches, with implied benefit for both groups.1
The 2026 Dyslipidemia Guideline has comparative recommendations, encouraging a dietary pattern rich in fruits, vegetables, nuts, legumes, whole grains, and fiber, while reducing saturated fat and replacing it with mono and polyunsaturated fats. It noted that dietary patterns that reduce saturated fat and increase unsaturated fat was more effective than restricting dietary cholesterol.2
The guideline reinforces the cardiovascular benefits of the Mediterranean, DASH, and vegetarian eating patterns and highlights the under-recognized Portfolio dietary pattern, which was shown to lower LDL by approximately 26 mg/dL. This dietary pattern emphasizes inclusion of 50 grams of plant-based protein per day, 45 grams of nuts, at least 10 grams of viscous fiber, and 2 grams of plant sterols per day.3
Additional guidelines are given for hypertriglyceridemia depending upon level of elevation2. If triglycerides (TGs) are 150-499, added sugars are limited to 6% of calories, total fat is 30-35%, and alcohol is to be avoided. If TGs are 500-999, added sugars are limited to <5% of calories, total fat to 20-25%, and it is recommended to abstain completely from alcohol. If TGs are over 1000 mg/dl, added sugars are eliminated, total fat is limited to 10-19%, and again, alcohol abstinence is recommended.
For all groups, 150 minutes of activity is recommended, and 5-10% weight loss is considered for individuals who may benefit. Consideration of the amount, type, and quality of carbohydrates shows efficacy in lowering TGs. In addition to LDL and TG lowering, dietary patterns aim to improve overall metabolic health, including weight reduction, reduced inflammation, and improved blood pressure and glucose control.2
45% of CVD-related deaths are linked to poor diet quality4; however, the Dyslipidemia Guidelines call out the conundrum of individual variability in LDL response to dietary changes, particularly reductions in saturated fat intake2. While replacing saturated fats with foods high in monounsaturated and polyunsaturated fats is consistently associated with LDL-C reduction4, individual responses vary widely.5
These individual differences mean that two people on the same heart-healthy diet may see different LDL outcomes.

For example, some genetic variants affect how efficiently the body clears LDL particles.5 Inflammation and insulin resistance may influence dietary LDL lowering, since hyperinsulinemia impacts hepatic lipid synthesis, clearance, and LDL particle composition.6 Variations in bile acid synthesis and reabsorption also contribute, since bile acids play a key role in cholesterol homeostasis. Finally, overall dietary and other lifestyle patterns affect LDL response, highlighting the importance of comprehensive and personalized strategies.
Healthful dietary patterns reflect the synergy of the overall diet, not just a single macronutrient change.
The ADA Standard of Care and the ACC/AHA Dyslipidemia guidelines align in recommending dietary patterns based on whole foods, increased fiber intake, reduced red meat and processed meat consumption, reduced saturated fat intake, and comprehensive lifestyle interventions. However, gaps remain.
More research is needed to clarify how specific individual differences influence dietary needs, how dietary patterns affect emerging lipid markers (ApoB, endothelial function, inflammation, etc.), nutrition interventions impacting cardiovascular risk reduction for individuals with type 1 diabetes, and the long-term impact of nutrition interventions over a lifetime4.
Cardiovascular risk reduction requires team-based care, addressing not only diet but social determinants of health, activity, tobacco cessation, sleep hygiene, and pharmacotherapy to manage cholesterol, blood glucose, blood pressure, and comorbidities increasing risk. As evidence evolves, diabetes health care professionals can help translate these guidelines into practical, personalized strategies to support heart health.
Christine Craig, MS, RDN, CDCES
Founder: Nutrition for Daily Living
Get exam-ready with confidence.
Course credits through AMA PRA Category 1 Credits™, ACPE, ANCC, and CDR!
Full accreditation details are available on the registration page
Our CDCES Boot Camp Online Prep Bundle is a comprehensive, high-impact program built specifically for healthcare professionals preparing for the Certified Diabetes Care and Education Specialist (CDCES) exam who want to level up their clinical knowledge and skills.
This evidence-based study bundle is a comprehensive BC-ADM Boot Camp designed for advanced-level healthcare professionals preparing for the Board Certified in Advanced Diabetes Management (BC-ADM) exam and will also provide you with state-of-the-art information to level up your clinical practice.
When providing Diabetes Self-Management Education (DSME), which of the following list includes the ADCES 7 Self-Care Behaviors?
Get exam-ready with confidence.
Course credits through AMA PRA Category 1 Credits™, ACPE, ANCC, and CDR!
Full accreditation details are available on the registration page
Our CDCES Boot Camp Online Prep Bundle is a comprehensive, high-impact program built specifically for healthcare professionals preparing for the Certified Diabetes Care and Education Specialist (CDCES) exam who want to level up their clinical knowledge and skills.
This evidence-based study bundle is a comprehensive BC-ADM Boot Camp designed for advanced-level healthcare professionals preparing for the Board Certified in Advanced Diabetes Management (BC-ADM) exam and will also provide you with state-of-the-art information to level up your clinical practice.
For last week’s practice question, we quizzed participants on LDL target for 2026. 55% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it by clicking here.
RZ is 47 years old with type 2 diabetes and hypertension. RZ takes metformin 1000 mg BID, plus lisinopril 20mg daily. RZs LDL is 140 mg/dL.
Based on the most recent ADA Standards, what is the LDL Cholesterol target for RZ?
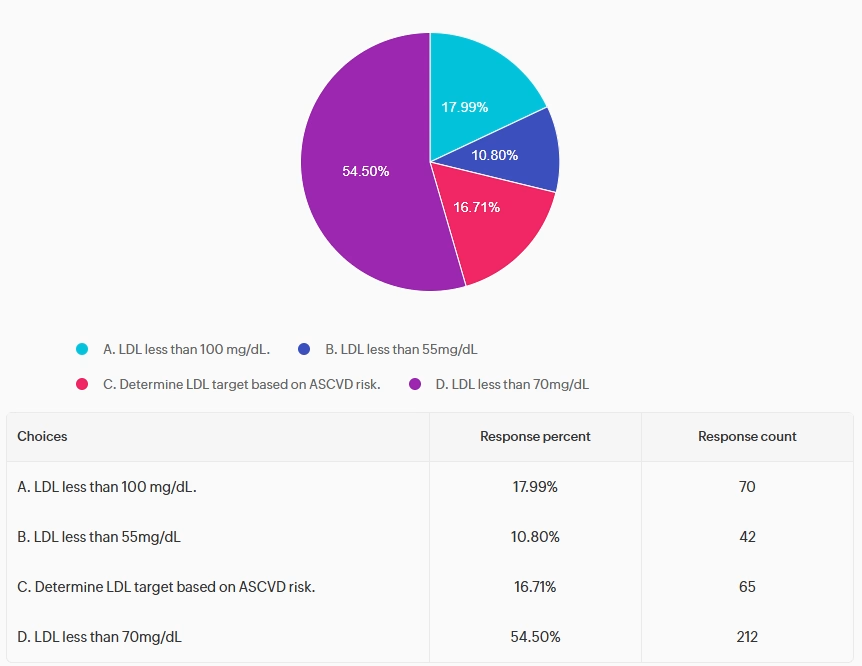
Answer A is incorrect. 17.99% chose this answer, “LDL less than 100 mg/dL.” This juicy answer was the previous goal for LDL.
But for the past few years, the ADA has established an LDL cholesterol goal of less than 70mg/dL (often using high-intensity statins) in diabetes. Reducing the LDL significantly decreases the risk of major cardiovascular events (heart attacks, strokes) by roughly 20% for every 39 mg/dL reduction. This target stabilizes plaque, slows atherosclerosis, and improves mortality, especially for high-risk individuals.
Answer B is incorrect. 10.80% of you chose this answer, “LDL less than 55 mg/dL.” This answer is tempting. The LDL goal off 55 mg/dL is recommended for individuals with diabetes with existing CV disease. Given that RZ has type 2 and hypertension and a LDL of 140 mg/dL, the ADA goal is to get LDL to half of the current value AND less than 70 mg/dL.
Answer C is incorrect. 16.71% chose this answer, “Determine LDL target based on ASCVD risk.” It might be helpful to calculate CV risk, but the ADA Standards make taking action simple and clear. If a person is 40 years or older, the LDL Goal is less than 70mg/dL and 50% reduction from their current LDL level. For people with diabetes with existing CV disease, the LDL goal is less than 55 mg/dL.
Finally, Answer D is correct. 54.50% of respondents chose this: “LDL less than 70mg/dL.” GREAT JOB! Based on the ADA 2026 guidelines, the LDL Goal is less than 70mg/dL and 50% reduction from their current LDL level, for people with diabetes over the age 40 with CV risk factors.
Reducing the LDL significantly decreases the risk of major cardiovascular events (heart attacks, strokes) by roughly 20% for every 39 mg/dL reduction. This target stabilizes plaque, slows atherosclerosis, and improves mortality, especially for high-risk individuals.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Save $75 thru April 30th
Join national experts including Dr. Diana Isaacs (Cleveland Clinic), Beverly Thomassian (30+ years of experience), and Christine Craig for high-impact, virtual learning—no travel required.
✔ Learn from National Experts — Anywhere
Get the same expert-level instruction you’d receive in person, delivered live to your home or office.
✔ 1-year Access
Get exam-ready with confidence.
Course credits through AMA PRA Category 1 Credits™, ACPE, ANCC, and CDR!
Full accreditation details are available on the registration page
Our CDCES Boot Camp Online Prep Bundle is a comprehensive, high-impact program built specifically for healthcare professionals preparing for the Certified Diabetes Care and Education Specialist (CDCES) exam who want to level up their clinical knowledge and skills.
This evidence-based study bundle is a comprehensive BC-ADM Boot Camp designed for advanced-level healthcare professionals preparing for the Board Certified in Advanced Diabetes Management (BC-ADM) exam and will also provide you with state-of-the-art information to level up your clinical practice.

In honor of Earth Day, April 22, 2026, we’re shining a light on the power of native plants in creating vibrant, resilient ecosystems—for wildlife and for people. See our Earth Day List of Resources Here!
Native plants—those that have evolved naturally in a specific region—play a crucial role in supporting local pollinators, birds, butterflies, and other wildlife. These plants provide essential food, pollen, and shelter that many species rely on for survival. And while the benefits to the environment are clear, cultivating native plants also boosts human well-being. Thriving ecosystems support cleaner air and water, increased biodiversity, and create opportunities for people to reconnect with nature.
When Coach Beverly moved into her home 26 years ago, she planted what many of us do—flowers and grasses that looked appealing and could withstand local heat. With an acre of land surrounding her home and office, she had space to experiment, adding a wide variety of foliage and trees for beauty and shade.
But like many at that time, she wasn’t yet aware of the importance of native plants—or how their presence (or absence) affects the animals, insects, and birds that share our space.
Over time, as she learned more about habitat loss and the plight of pollinators, she began to rethink her approach. Through research, visits to a nearby native nursery, and the help of trusted websites, she and her husband began the transformation: reshaping their land into a space that supports bees, butterflies, frogs, birds, lizards, and more. Today, their yard is not only beautiful but also an oasis for wildlife—and a model of sustainable gardening.
In addition to plants, providing a water source can be a game-changer for thirsty pollinators and wildlife. Whether it’s a birdbath, a shallow dish, or a small pond, water invites life into any garden.
Last year, Coach Beverly dug a small frog pond. Within weeks, frogs, toads, and birds made themselves at home. A year later, the pond teems with tadpoles, mosquito fish, dragonflies, water beetles, and countless other tiny creatures.
The pond has become a source of daily joy and fascination for family and visitors alike—a reminder of how deeply nature nurtures our spirits. It has also been a powerful tool for stress relief and mental well-being.
For those managing diabetes, chronic conditions, or everyday stress, spending time in nature and caring for living things can be deeply therapeutic. And it doesn’t have to be complicated.
Start small:
For the more adventurous, creating a native plant garden is a wonderful excuse to get outdoors, move your body, and take pride in a growing, living space. There’s something special about tasting a sun-warmed tomato that’s been nurtured from seed to fruit.
A great place to start is the article Audubon – 20 Common Types of Native Plants, which outlines beneficial plants found across the U.S. To make it local, cross-reference with your zip code using tools like the Native Plant Finder – NWF by the National Wildlife Federation.
For example, in Chico, California, the California Christmas-Berry is drought-tolerant and a favorite food source for local birds.
🌳 Here are a few native plant ideas to consider:
Need help sourcing plants? The Plant Native website offers a helpful directory of native nurseries throughout the U.S.
Many people feel overwhelmed or discouraged by the state of the planet. But there is also a growing awareness of our power to make change—and hope rooted in action.
Whether it’s planting a single native shrub, providing a bowl of water, or simply observing and appreciating the life around us, every effort makes a difference.
Visit www.earthday.org and Project Regeneration for more ideas and inspiration on how to help the Earth thrive.
Each person has the ability to nurture the planet and themselves, starting right at home. Native plants are a simple, beautiful way to support both biodiversity and human well-being.
So this Earth Day, consider taking that first step. Plant something. Provide water. Let nature in. And know that even the smallest actions ripple outward in meaningful ways.
🌎 Happy Earth Day from Coach Beverly and the Diabetes Education Services team.