Subscribe
eNewsletter
Ready to get certified?
Free CDCES Coach App
eNewsletter
Free CDCES Coach App
Free Med Pocket Cards

CS is a 42-year-old with type 1 diabetes for just over 18 years. In the past year, their A1C changed from 7.4% to 9.1%, and weight increased by 20 pounds. Review of CGM data suggests missed insulin boluses more than 7 times per week, and discussion with CS reveals missed clinic visits due to feeling “burned out”. They score in the moderate range on the Diabetes Distress Scale.
Based on the ADA 2026 Standards of Care, which of the following is the most appropriate next step?


If you’ve considered not renewing your professional practice group membership this year, you’re not alone. Membership in professional organizations has declined as many turn to social media and AI-driven platforms for information and connection. Still, I encourage you not to abandon professional membership in favor of options that may seem cheaper or more convenient.
In a noisy, chaotic landscape of information overload, professional practice groups remain a refuge from the storm. They offer a trusted alternative to clickbait, providing vetted expertise, meaningful connection, and true professional community.
No amount of viral TikTok videos or LinkedIn commentary can replace the depth of connection and sense of purpose that come from active engagement in a professional practice organization. And, here’s why.
Professional practice groups, also known as professional practice organizations, are designed to advance a specific field by providing members with networking opportunities, professional development, and practice resources. In healthcare, these organizations may be tailored to the needs of a single discipline, such as the American Nurses Association, or span interdisciplinary areas of practice, like the Association of Diabetes Care and Education Specialists or the American Diabetes Association.
Some organizations focus primarily on education and credentialing, while others emphasize leadership development and community building. Still others center their work on advocacy related to patient care, access, and insurance coverage.
At its core, most professional practice groups are founded and driven by their members, with membership dues supporting the administrative needs required to operate. As groups grow, they often engage professional management or organizational leadership teams to oversee day-to-day operations such as membership services, programming, finances, legal compliance, and other administrative functions.
Strategic direction and oversight typically remain the responsibility of an elected or appointed governing body. In some cases, professional organizations may choose to hire members, transitioning them from volunteer roles into paid staff positions.
As operating costs rise, often without corresponding increases in salaries or reimbursement, many professional practice groups partner with industry or government organizations for additional financial support. These partnerships can help keep membership dues, educational programming, and events accessible and affordable for members.
It would be easy to blame declining professional membership on COVID, but the reality is this trend started long before the pandemic. Across healthcare, fewer clinicians are joining or renewing professional organizations. Cost is often the biggest factor. When budgets are tight, many people feel forced to choose one membership instead of several. Others question whether the return on investment is still there, especially when education, networking, and professional content are now easy to find online for free.
In my own field of dietetics, I also hear concerns about transparency and alignment with the future of the profession. The move to a master’s degree requirement without a meaningful increase in entry-level pay has created real frustration, particularly for early-career professionals and those from underrepresented backgrounds. Many feel their needs were not fully considered or advocated for during that transition.
These frustrations are valid. But they are also exactly why walking away may not be the answer. Professional practice groups are shaped by the people who show up. If something isn’t working, the most effective way to change it is to get involved.
Despite the challenges, the benefits of professional membership far outweigh the drawbacks, and the opportunity to influence the future of your profession is worth staying engaged.
Social media platforms like LinkedIn, Substack, and X (formerly Twitter) are great for ideas and inspiration, but they rarely offer sustained, reciprocal mentorship. Most interactions are brief, one-sided, or tied to someone selling something.
Professional practice groups offer something different. They foster trusted relationships with people who have walked the same path and understand the realities of the work. Advice is shared openly, support develops over time, and there is no sales funnel attached. It is not a transaction. It is a co-op.
Professional practice groups offer a space to ask questions without worrying about who is watching or how you are being perceived. There is room to be unsure, curious, or quietly ambitious, especially early in your career or during periods of transition.
Unlike social media, which often rewards confidence and visibility, professional groups tend to reward competence, growth, and thoughtful engagement. The focus is less on performance and more on learning and supporting one another as professionals.
Most online content is designed for reach, not rigor. Professional practice groups focus on depth, offering evidence-based, peer-reviewed insights shared by professionals, for professionals. It is not about trends. It is about trust. As these professional practice groups evolve, many are also opening the door to honest conversations about topics once considered off-limits, such as workplace culture, compensation, and career options.
I’ve made meaningful connections on social media and learn something new every day from tools like ChatGPT. Those platforms have their place.
But when I want to understand where a profession is really headed, I look to professional practice groups. Who is presenting the research? What study resources are being recommended? Who is mentoring, volunteering, and helping shape the future of the field? These groups create space to contribute, learn, and grow alongside peers who care deeply about the work.
I’ve always respected my work colleagues, but I truly value my professional practice peers. I hope you will, too.
References:
Sarah is the owner of Sarah Hormachea: Diabetes Care and Education, LLC. She is a long-time member of the Academy of Nutrition and Dietetics, the Association of Diabetes Care and Education Specialists (ADCES), and the American Diabetes Association (ADA). She currently serves as Webinar Chair for the Academy’s Diabetes Practice Group and is an incoming member of the ADCES Board of Directors. She is also enrolled in a women’s leadership development program through the ADA.


This year’s National Nutrition Month’s theme is “Discover the Power of Nutrition.” Nutrition has the power to help individuals and communities thrive.
The nutrition profession offers diverse career pathways spanning clinical care, community health, education, research, industry, leadership, and private practice, allowing Registered Dietitian Nutritionists (RDNs), also known as Registered Dietitians (RDs), to grow and evolve their careers over time.
RDs leverage “the power of nutrition” while delivering evidence-based medical nutrition therapy (MNT) across the diabetes care continuum.
Nutrition is both a challenge and an opportunity for individuals living with diabetes and can have direct impacts on health outcomes.
As of February 2026, more than 113,900 RDNs are credentialed in the United States.1 In 2025, just over 8,600 RDNs also held the Certified Diabetes Care and Education Specialist (CDCES) credential, representing approximately 45% of all CDCES professionals2. Employment for dietitians is projected to grow by 6%3. However, the field has recently seen a decline in new graduates, likely due to post-pandemic enrollment shifts and the 2024 transition to a required master’s degree4. Supervised practice hours and passing the national examination continue to be required. Despite these challenges, the RDN credential remains the gold standard for evidence-based nutrition practice and new career opportunities continue to evolve.
Dietitians in diabetes care practice in a wide range of settings, including hospitals and outpatient clinics, primary care and endocrinology offices, federally qualified health centers, public health programs, academia, digital health, industry, community-based organizations and more. Increasingly, entrepreneurship has also emerged as another pathway. Approximately 12% of RDNs in the United States are self-employed.5
ADCES recently launched an Entrepreneurship Community of Interest (COI) group, leaning into this growing career trend. For many dietitians, private practice offers an opportunity to meet an unmet need or specialization, schedule flexibility, and a space to design new programs and interventions.
Both the American Diabetes Association and the Academy of Nutrition and Dietetics recommend referral to MNT for individuals with diabetes, yet fewer than 10%6 receive these services. Barriers include limited access to RDNs within health systems, fragmented referral networks, and inconsistent insurance coverage for nutrition care.7 These gaps in access were a key motivator for my own entrepreneurial venture, reinforcing that many successful innovations are often driven by unmet needs.
In 2023, I founded Nutrition for Daily Living to help address access barriers within my own local community. Building a business required learning the business of nutrition including marketing, finances, legal requirements, and navigating insurance for MNT. What began as a part-time side hustle has now become a full-time practice, enabling me to work towards my goal of delivering personalized care while fostering long-term partnerships with clients. No matter your setting, innovation can start with awareness and creativity and when paired with courage, it can open doors to meaningful impact and success.
Dietitians in diabetes care play an important role in advancing our profession by bridging nutrition innovations, clinical care expertise, behavioral strategies, and collaboration with patients, communities, and care teams. With the increasing complexity of diabetes management, RDNs bring essential skills in leadership, problem-solving, and patient-centered care. Individuals with an entrepreneurial spirit, no matter the care setting, can pilot new approaches, identify unmet needs, and design new care models. As we celebrate National Nutrition Month together, let’s recognize the many important contributions RDNs provide in transforming diabetes care.
References:
Course credits through AMA PRA Category 1 Credits™, ACPE, ANCC, and CDR!
Get exam-ready with confidence.
Our CDCES Boot Camp Online Prep Bundle is a comprehensive, high-impact program built specifically for healthcare professionals preparing for the Certified Diabetes Care and Education Specialist (CDCES) exam who want to level-up their clinical knowledge and skills.
✔ Learn at your pace with expert-led, exam-focused content
✔ Everything you need—organized, practical, and in one place
✔ Perfect for self-directed learners who want complete, person-centered content for clinical practice and exam prep.
✔ Build knowledge, sharpen test-taking skills, and prepare with confidence—on your schedule.
Focused. Flexible. Proven.
Basic & e-Deluxe CDCES Boot Camp Bundle Includes:

Course credits through AMA PRA Category 1 Credits™, ACPE, ANCC, and CDR!
Get exam-ready with confidence.
Our comprehensive BC-ADM Online Study Programs are specifically designed for healthcare professionals who are studying for the Board Certified in Advanced Diabetes Management (BC-ADM) exam.
✔ Learn at your pace with expert-led, exam-focused content
✔ Everything you need—organized, practical, and in one place
✔ Perfect for self-directed learners who want complete, person-centered content for clinical practice and exam prep.
✔ Build knowledge, sharpen test-taking skills, and prepare with confidence—on your schedule.
Focused. Flexible. Proven.
Basic & e-Deluxe BC-ADM Boot Camp Bundle include:
Gain fresh insights, practical tools, and a deeper understanding of the latest in person-centered diabetes care. Our expert team brings the ADA Standards of Care to life—covering medications, behavior change, technology, and more!


Did you know that in ancient times, diabetes was identified by the sweet taste of a person’s urine?
Thankfully, science has come a long way from this ancient practice! The introduction of fingerstick blood glucose meters in the 1970s and continuous glucose monitors (CGMs) in the early 2000’s marked significant advancements in blood glucose monitoring. With more than 800 million people worldwide living with diabetes, interest in pain-free glucose testing is growing.1
Although current CGMs and fingerstick methods still require skin penetration, needle-free alternatives are being promoted, prompting many questions. Let’s discuss how healthcare professionals can address these products using evidence-based information.
Noninvasive (NI) glucose monitoring is a method of measuring blood glucose that does not involve breaking the skin. NI glucose monitoring technology under development includes: 2
FDA approval is granted for glucose monitoring devices used for either medical or lifestyle management. FDA approval for medical management is based on sufficient evidence of safety and accuracy for people living with diabetes. FDA approval ensures adequate evidence to guide treatment decisions, such as insulin dosing. FDA approval for lifestyle use applies to individuals who do not use the device for the medical management of diabetes and who are not on insulin therapy.
Currently, no NI glucose monitoring devices have received FDA approval for medical management of diabetes. In 2024, the FDA issued a safety announcement that NI glucose devices could pose a possible threat to those with diabetes, as the FDA has not approved them.3 Numerous companies are currently in the research process to advance NI glucose monitoring devices toward FDA approval.
When considering noninvasive glucose monitoring, it’s essential to understand how these devices fit into everyday diabetes care. Despite the lack of FDA approval, clients can purchase NI glucose monitoring devices without a prescription. Clients may be using these before the healthcare provider is ever aware.
Individuals living with diabetes should be aware that many factors, including hydration status, skin characteristics, temperature, and movement, can affect NI glucose device readings. These devices may be better suited for detecting general trends but are not approved for making real-time treatment decisions. As diabetes healthcare professionals, we can provide guidance on the use of FDA-approved devices to verify readings and inform treatment decisions. Arming our clients with this information can help avoid frustration and unsafe treatment decisions.
Diabetes healthcare providers often approach noninvasive (NI) glucose monitoring with cautious optimism. While the appeal of “no more pokes” is understandable, clients may be influenced by strong marketing claims. As providers, our role is to meet clients where they are to start the conversation.
As with any other FDA-approved diabetes technology, not every device is the right fit for everyone. Ask clients about their diabetes goals, barriers, and assess their digital literacy. Address what clients are seeing on social media and online ads, and how these NI devices compare to current FDA-approved blood glucose monitoring technology.
Here are some helpful tips that can further the conversation:
As technology advances, we hope to see accurate and safe NI glucose monitoring options for those living with diabetes. Until then, we can partner with our clients to provide education and clinical insights on the latest trends in diabetes technology.
References:
Course credits through AMA PRA Category 1 Credits™, ACPE, ANCC, and CDR!
Get exam-ready with confidence.
Our CDCES Boot Camp Online Prep Bundle is a comprehensive, high-impact program built specifically for healthcare professionals preparing for the Certified Diabetes Care and Education Specialist (CDCES) exam who want to level up their clinical knowledge and skills.
✔ Basic CDCES Boot Camp – From the fundamentals, to the ADA standards, to test strategies and exam mastery! This complete exam prep includes Levels 1, 2, and 3 (30+ courses, 50+ CEs, 400+ practice questions)
✔ e-Deluxe CDCES Boot Camp – Everything in Basic PLUS the [e-Book] ADCES Certification Review Guide | 6th Edition (475+ practice questions)
✔ Mini CDCES Boot Camp – Accelerated program for experienced healthcare professionals (skips Level 1 | Diabetes Fundamentals, includes Levels 2 & 3, 20+ courses, 40+ CEs, 325+ practice questions).
Course credits through AMA PRA Category 1 Credits™, ACPE, ANCC, and CDR!
Get exam-ready with confidence.
Our comprehensive BC-ADM Online Study Programs are specifically designed for advanced level healthcare professionals who are studying for the Board Certified in Advanced Diabetes Management (BC-ADM) exam.
✔ Basic BC-ADM Boot Camp – Complete exam prep includes Levels 2, 3, and 4 (30+ courses, 50+ CEs, 400+ practice questions)
✔ e-Deluxe BC-ADM Boot Camp – Everything in Basic PLUS the ADCES Certification Review Guide E-book with an additional 475+ practice questions.
Gain fresh insights, practical tools, and a deeper understanding of the latest in person-centered diabetes care. Our expert team brings the ADA Standards of Care to life—covering medications, behavior change, technology, and more!

Coach Beverly is thrilled you will be joining this special gathering and celebration!
During this virtual book launch, a special guest interviewer will join Coach Bev for a heartfelt conversation about why this book matters now and the real stories from clinical practice that inspired it. Coach Bev will also share the personal journey of writing Healing through Connection and how she discovered her voice along the way. We will conclude with an interactive question-and-answer session and allow time for connection.
Come celebrate connection, healing, and the power of story as we honor the shared human experience at the heart of healthcare.

Have you heard about the twiist insulin pump? If not, don’t worry – we are here to keep you in the loop! The twiist is the latest automated insulin delivery (AID) system to join the diabetes treatment toolbox. This insulin pump features a unique algorithm powered by Tidepool Loop Technology, offering clients another option in insulin management.
The twiist is an AID system that looks and acts a bit differently than current insulin pumps. FDA-approved for individuals 6 years old and older, it is a circular-shaped insulin pump. There is a bladder-type reservoir, called a cassette, that holds up to 300 units of insulin. The twiist AID system is currently compatible only with the Libre 3+ continuous glucose monitor (CGM) and iPhone. Meal and correction boluses are delivered via the phone app or Apple Watch for discreet diabetes management. Humalog (insulin lispro) U-100 and Novolog (insulin aspart) are the insulins approved for use with the twiist insulin pump.
The twiist AID system uses iiSure technology within the pump and the cassette to dose insulin. Sound waves are used for direct volume measurement to ensure accurate insulin dosing. This feature also identifies occlusions faster than other currently available AID
systems.¹ Insulin moves through the pump chamber into the iiSure chamber, where sound waves use four checkpoints to verify insulin flow and correct dosing:
1. A baseline measurement is taken of the empty iiSure chamber before the insulin reaches this part of the cartridge.
2. The iiSure chamber fills with the determined dose of insulin and is measured for accuracy.
3. A second check of the iiSure chamber is verified for accuracy.
4. After insulin delivery, the pump measures the iiSure chamber to calculate the amount of insulin delivered. ¹ Tidepool Loop is the algorithm that powers the twiist AID system. Tidepool Loop creates a 6-hour glucose prediction forecast based on pump settings, insulin on board, recent carbohydrate entries, and CGM history. This information is collected every 5 minutes to create a 6-hour glucose forecast. Clients using twiist can view this glucose forecast to help make treatment decisions.
As we have discussed, twiist not only looks different but also functions slightly differently from other AID systems.
Here are a few more unique features:
Target Range: One of the most interesting twiist differences is that the lowest target range setting is 87 mg/dL, with the highest being 180 mg/dL for insulin delivery recommendations.
Retroactive Meal Adjustment: Users can adjust the CHO amount for a meal or snack bolus if they consume fewer carbs than planned.
Emojis: Using meal emojis helps the algorithm set a personalized prediction of food absorption based on carb, fiber, and fat content. If emojis aren’t used, the system defaults to a 3-hour food absorption.
No contracts: The twiist is a pharmacy benefit (rather than a Durable Medical Equipment benefit) and does not require a long-term contract commitment.
Premeal Preset: This option allows the user to temporarily lower the correction range before a meal to help prevent a post-meal glucose spike.
Workout Preset: This optional setting allows for glucose ranges from 87 mg/dL to 250 mg/dL to be set before, during, or after a workout.
Diabetes healthcare professionals are considered experts in insulin pumps. Whether you are discussing insulin pump options, training, or troubleshooting the twiist insulin pump with clients, here are some helpful clinical pearls:
References:
Gain fresh insights, practical tools, and a deeper understanding of the latest in person-centered diabetes care. Our expert team brings the ADA Standards of Care to life—covering medications, behavior change, technology, and more!
If you’re preparing for the CDCES or BC-ADM exam, this conference, paired with a handful of free bonus courses, serves as the ideal study companion! Plus, this content counts toward the ADA Standards requirements for CDCES Renewal.
With interactive co-teaching, we keep sessions engaging, relevant, and fun.
Let’s learn and grow together!
Course credits through AMA PRA Category 1 Credits™, ACPE, ANCC, and CDR!
Program Objectives:
Upon completion of this activity, participants should be able to:
According to the new 2026 ADA Standards, “type 2 diabetes is associated with insulin secretory defects related to” which of the following?
For last week’s practice question, we quizzed participants on JR studying to take their CDCES exam, and they have questions studying for the 2025 or 2026 ADA Standards of Care. 55.56% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question

JR has been diligently studying to take their CDCES exam at the end of January 2026. They are wondering if they should study the 2025 or 2026 ADA Standards of Care.
As a mentor to healthcare professionals entering the field of diabetes, what do you recommend?
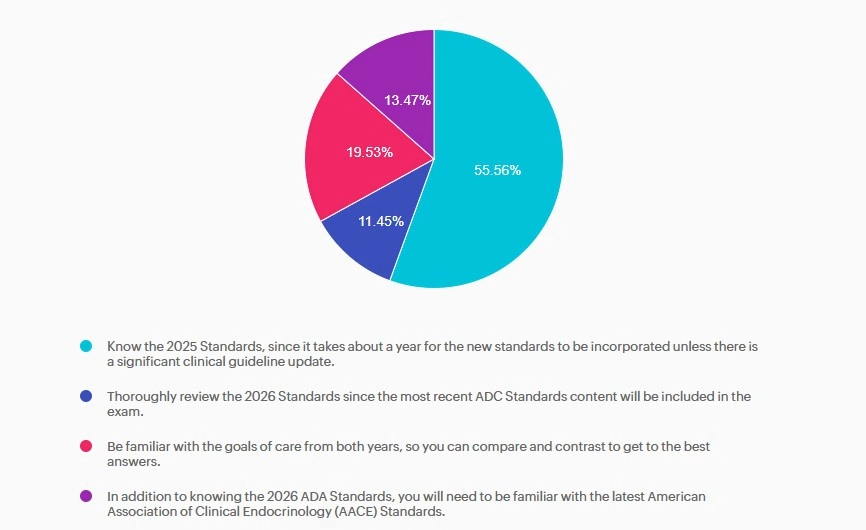
Answer A is correct: 55.56% chose this answer, “Know the 2025 Standards, since it takes about a year for the new standards to be incorporated unless there is a significant clinical guideline update.” Answer A is the BEST answer. It takes at least a year for the CBDCE to update the exam based on the ADA Standards. Knowing the 2025 Standards along with any urgent clinical updates announced in 2026 will help prepare JR for success.
Answer B is incorrect: 11.45% chose this answer, “Thoroughly review the 2026 Standards since the most recent ADC Standards content will be included in the exam.” Answer B is not the best answer. Since it takes at least a year for the CBDCE to update the exam based on the ADA Standards, JR can feel comfortable knowing the 2025 Standards along with any urgent clinical updates announced in 2026.
Answer C is incorrect: 19.53% chose this answer, “Be familiar with the goals of care from both years, so you can compare and contrast to get to the best answers.” Answer C is not the best answer. Thinking about comparing and contrasting two consecutive years standards and lead to testing confusion. JR can feel comfortable knowing the 2025 Standards along with any urgent clinical updates announced in 2026.
Answer D is incorrect: 13.47% chose this answer, “In addition to knowing the 2026 ADA Standards, you will need to be familiar with the latest American Association of Clinical Endocrinology (AACE) Standards.” Answer D is not the best answer. Since it takes at least a year for the CBDCE to update the exam based on the ADA Standards, JR can feel comfortable knowing the 2025 Standards along with any urgent clinical updates announced in 2026.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!