
Subscribe
eNewsletter
Ready to get certified?
Free CDCES Coach App
eNewsletter
Free CDCES Coach App
KS is 14 years old and recently diagnosed with type 2 diabetes. Their A1C is 8.6%, LDL cholesterol is 137 mg/dL and their GFR is greater than 90.
Based on this clinical information and the ADA Standards for Pediatric Care, in addition to lifestyle and behavior changes, what medication(s) would be recommended?
Click Here to Test your Knowledge
This course includes updated goals & guidelines for children living with type 1 or type 2 diabetes. This course discusses the special issues diabetes educators need to be aware of when working with children with diabetes & their families. We discuss the clinical presentation of diabetes, goals of care, & normal growth & development through the early years through adolescence. Strategies to prevent acute & long-term complications are included with an emphasis on positive coping for families & children with diabetes.
Objectives:
Intended Audience: A great course for healthcare professionals seeking information about providing care for children with diabetes and their families.
Don’t worry if you can’t make it live. Your registration guarantees access to the recorded version in the Online University.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
Join us live on August 30th, 2023, at 11:30 am PST for our NEW: Diabetes Technology Data Toolkit: Hands-on Data Interpretation Workshop with Dr. Diana Isaacs
As diabetes technology is becoming commonplace in our practice, figuring out how to make sense of all the data can seem overwhelming. Dr. Isaacs has a special knack for breaking down the essential elements of the Ambulatory Glucose Profile (AGP) and other reports to provide participants with a clear road map for data interpretation. She includes many sample practice cases utilizing CGM, connected pens, and insulin pumps.
By attending this interactive workshop, participants will become more confident in interpreting the AGP and continuous glucose monitor (CGM) data and determining needed medication and lifestyle adjustments.
Topics include:
Instructor: Diana Isaacs, PharmD, BCPS, BCACP, CDCES, BC-ADM, FADCES, FCCPCES, was awarded ADCES Diabetes Care and Educational Specialist of the Year for her educational platform promoting the use of CGM for people with diabetes and other innovations. She is the Director of Education & Training in Diabetes Technology at the Cleveland Clinic. She has numerous diabetes publications and research projects focusing on medications, CGM, and diabetes technology. You won’t want to miss this hands-on workshop with an international expert in the field.
All hours earned count toward your CDCES or BC-ADM
Accreditation Information: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.* The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.

Your team is invited to our Virtual DiabetesEd™ Training Conference! Set your team apart and prepare for diabetes certification!
Join this state-of-the-art conference taught by content experts, Diana Isaacs, PharmD, BCPS, BCACP, BC-ADM, CDCES, Beverly Thomassian RN, MPH, CDCES, BC-ADM, and Ashley LaBrier who are passionate about improving diabetes care.
Group discounts are available!*
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
Last week, a disheartened individual arrived for their initial diabetes appointment. With slumped shoulders, they shared how a provider had lectured them about their elevated A1C and insisted they add an additional diabetes medication.
This person described how they had made significant progress in healthy eating and moving more, but that didn’t seem to matter to the provider. Worse, this individual just felt like giving up.
The good news is that this heartbreaking story inspired me to take action.
I penned an article on Person-Centered Coaching and then created a PDF Cheat Sheet that you can reference and share with your colleagues.
My hope is that we can all be a part of lifting people up and acknowledging even those tiny lifestyle changes that are so difficult to initiate and sustain. Through careful listening, reflection, and collaboration, we can make meaningful connections that support change in the long run and improve well-being.
We also reflect on one year of action in celebration of Earth Day. Our family is committed to making ten changes in our daily lives to give back to this incredible planet we get to inhabit. In addition, the crew at Diabetes Education Services decided to highlight the benefits of our domestic pets. They not only enhance our work day but also improve the health outcomes of people with diabetes.
Lastly, we are excited to share that people with diabetes can lower their blood sugars by changing the order of the foods consumed. You can read more about these exciting topics below, plus take a stab at our Question and Rationales of the Week.
Thanks for helping to lift people up,
Coach Beverly and Bryanna
Announcements
__________________________
Upcoming Webinars
People with diabetes are at increased risk of Lower Extremity Complications. This course reviews the steps involved in performing a detailed assessment of the lower extremities, including how to use a monofilament and tuning fork to detect neuropathy. We also discuss the significance of the Ankle Brachial Index and strategies to prevent lower extremity complications.
Objectives:
Intended Audience: This is a great course for healthcare professionals who want to learn the steps involved in providing a thorough lower extremity assessment.
Don’t worry if you can’t make it live. Your registration guarantees access to the recorded version in the Online University.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.

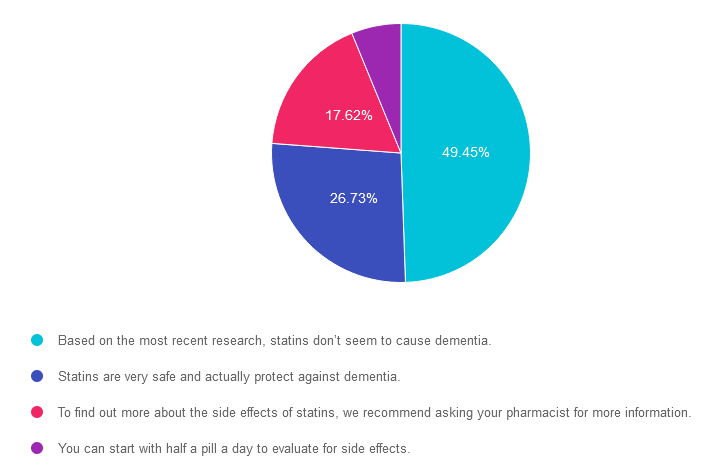
For last week’s practice question, we quizzed participants on statins & the risk of dementia. 49% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question: LR is 78 years old with a new diagnosis of diabetes. Their A1C is 7.9%, LDL cholesterol is 98 mg/dL, GFR is 58 mg/g and their BP is 124/78. The provider recommends a referral to the RD and DSME program and writes a prescription for metformin XR 500mg daily and lovastatin 20mg. LR is worried about taking a statin because they heard it can cause dementia.
Based on the ADA Standards, what is the best response?
Answer Choices:
If you are thinking about taking the certification exam, this practice test question will set you up for success. Test writers anticipate possible answers based on the details in the question. They will wave those “juicy answers” right under your nose. Your job is to weed through the particulars, pluck out the most important elements and choose the BEST answer.
Answer 1 is correct. 49.45% chose this answer. “Based on the most recent research, statins don’t seem to cause dementia.” YES, is the BEST answer. According to ADA 2023 SOC 10 a recent systematic review of the U.S. Food and Drug Administration’s (FDA’s) postmarketing surveillance databases, randomized controlled trials, and cohort, case-control, and cross-sectional studies evaluating cognition in patients receiving statins found that published data do not reveal an adverse effect of statins on cognition (138). Therefore, a concern that statins or other lipid-lowering agents might cause cognitive dysfunction or dementia is not currently supported by evidence and should not deter their use in individuals with diabetes at high risk for ASCVD (138).
Answer 2 is incorrect. 26.73% of you chose this answer. “Statins are very safe and actually protect against dementia.” Although the first part of this statement is correct, statins are safe, there is no evidence presented in the ADA Standards that statins protect against dementia.
Answer 3 is incorrect. About 17.62% of respondents chose this. “To find out more about the side effects of statins, we recommend asking your pharmacist for more information.” Although pharmacists are incredibly knowledgeable about medications, diabetes specialists can relate evidence based information to the people we serve, instead of making them take additional action to get the information they need to move forward. The good news is that there is no evidence that statins or other lipid-lowering agents might cause cognitive dysfunction or dementia and their use is recommended in individuals with diabetes at high risk for ASCVD.
Finally, Answer 4 is incorrect. 6.19% chose this answer. “You can start with half a pill a day to evaluate for side effects.” This approach is tempting, but it doesn’t address the fear of the statin causing dementia. The good news is that there is no evidence that statins or other lipid-lowering agents might cause cognitive dysfunction or dementia and their use is recommended in individuals with diabetes at high risk for ASCVD.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
We are living longer & more people are getting diabetes. The American Diabetes Association has updated the Older Adults Standards, with special attention to considering the reduction of medication & insulin therapy intensity. The older population has unique issues & special needs that require consideration as we provide diabetes self-management education. This online course highlights key areas of assessment, intervention, and advocacy for older clients living with diabetes.
Objectives:
Intended Audience: An important course for healthcare professionals seeking to gain an understanding of the special issues and goals for older adults.
Don’t worry if you can’t make it live. Your registration guarantees access to the recorded version in the Online University.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
JR arrives at the clinic wearing a walking boot due to a recent foot injury. Tells you that they “banged their foot” on some farm equipment and since then it has been warm and swollen. It hurt at first, but the pain has diminished with time.
When JR takes off the boot, you see that the left foot needs attention.
Based on this photo, what diabetes-related foot condition do you suspect?


People with diabetes are at increased risk of Lower Extremity Complications. This course reviews the steps involved in performing a detailed assessment of the lower extremities, including how to use a monofilament and tuning fork to detect neuropathy. We also discuss the significance of the Ankle Brachial Index and strategies to prevent lower extremity complications.
Objectives:
Intended Audience: This is a great course for healthcare professionals who want to learn the steps involved in providing a thorough lower extremity assessment.
Don’t worry if you can’t make it live. Your registration guarantees access to the recorded version in the Online University.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
We have two updates to announce that have been captured in our electronic Medication PocketCards.
The DPP-IV Inhibitor Saxagliptin (Onglyza) and combination medication, Kombiglyze XR (saxagliptin/metformin extended-release tablets), have been permanently discontinued, according to manufacturer AstraZeneca.
A recent posting on the Food and Drug Administration’s (FDA) Drug Shortages tracker indicates that both products were discontinued because of a business decision and not due to safety or efficacy-related concerns.
There are three other DPP-IV inhibitors still available along with several combination versions. See our updated electronic ePocketCard that reflects this update.
In late 2022, the FDA approved the use of Dulaglutide (Trulicity for Pediatrics with Type 2 diabetes ages 10-17. Currently, metformin, insulin and the following GLP-1 RA’s are approved for pediatrics with type 2 diabetes, ages 10-17 See updated ePocketCard.
GLP-1 RA list of approved medications for pediatrics.
GLP-1 RAs have the benefit of not only lowering A1C, they also support weight loss and Exenatide XR and dulaglutide only need to be taken once a week. This weekly dosing can be a big advantage for busy families.
Our currently available laminated Diabetes Med PocketCards do not reflect these changes, but we will be reprinting later this year to reflect these updates.
This course will transform your test anxiety into calm self-confidence and test-taking readiness.

“Becoming a Certified Diabetes Care and Education Specialist (CDCES) is one of the best professional and personal decisions I have ever made.” – Coach Beverly Thomassian, RN, MPH, CDCES, BC-ADM
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
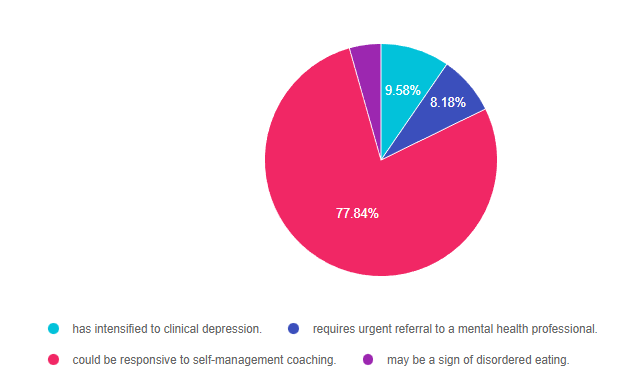
For last week’s practice question, we quizzed participants on diabetes distress. 78% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question: JR has type 1 diabetes and tells you, “My doctor just doesn’t seem to understand how to manage type 1 diabetes. Sometimes, I just skip my appointments because it feels like a waste of time.” JR’s most recent A1C was 8.7% and their time in ranges keeps decreasing with each visit.
Based on this, you realize that JR’s provider-related diabetes distress:
Answer Choices:
If you are thinking about taking the certification exam, this practice test question will set you up for success. Test writers anticipate possible answers based on the details in the question. They will wave those “juicy answers” right under your nose. Your job is to weed through the particulars, pluck out the most important elements, get rid of false answers, do any math very carefully and choose the BEST answer.
Answer 1 is incorrect. 9.58% chose this answer. “has intensified to clinical depression.” This is a tempting answer, but we don’t enough evidence to support that JR is struggling with depression. If we had JR complete the Diabetes Distress Scale, he would certainly score high on provider related distress based on this statement, “My doctor just doesn’t seem to understand how to manage type 1 diabetes. Sometimes, I just skip my appointments because it feels like a waste of time.” These comments certainly fit in the distress category. Through careful questioning and exploration, the diabetes educator could certainly help with problem solving.
Answer 2 is incorrect. 8.18% of you chose this answer. “requires urgent referral to a mental health professional.” Based on JR’s statement, “My doctor just doesn’t seem to understand how to manage type 1 diabetes. Sometimes, I just skip my appointments because it feels like a waste of time,” JR is certainly in distress. However, there is no language indicating that JR is in imminent danger of self-harm. Through careful questioning and exploration, the diabetes educator could certainly carefully assess JR’s mental health state and help with problem solving and referrals as needed.
Answer 3 is correct. About 77.84% of respondents chose this. “could be responsive to self-management coaching.” YES. This is the best answer. We could start by administering the Diabetes Distress Scale and then hone in on the high scoring areas. Then through careful questioning and exploration, the diabetes educator could certainly help with problem solving and identify if additional resources or referrals are needed.
Finally, Answer 4 is incorrect. 4.39% chose this answer. “may be a sign of disordered eating.” but we don’t enough evidence to support that JR is experiencing disordered eating. However, if we had JR complete the Diabetes Distress Scale, he would certainly score high on provider related distress based on this statement, “My doctor just doesn’t seem to understand how to manage type 1 diabetes. Sometimes, I just skip my appointments because it feels like a waste of time.”
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Addressing diabetes distress can be tricky, even for seasoned healthcare professionals.
We invite you to attend this hands-on training program that provides the essential steps to address diabetes distress combined with an innovative approach to glucose management. Our experts offer realistic strategies to address diabetes distress that you can immediately apply to your practice setting. Plus, the ReVive 5 Program provides a breadth of tools and resources to create more meaningful connections with people with diabetes.
“ReVive 5” breathes new life into our relationship with diabetes, bringing a fresh perspective to both the person with diabetes and the provider.
Team of Experts: ReVive 5 is taught by a team of 3 Interdisciplinary Experts:

Accredited Training Program:
Speakers Interviews – Learn more about the ReVive 5 Team
What is the Biggest Takeaway when Addressing Diabetes Distress? – Dr. Susan Guzman
Do you have to be a Mental Health Expert to Tackle Diabetes Distress? – Dr. Lawrence Fisher
Why I Transformed my Approach to Diabetes Self-Management Education- Coach Beverly
Don’t worry if you can’t make it live. Your registration guarantees access to the recorded version in the Online University.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
LR is 78 years old with a new diagnosis of diabetes. Their A1C is 7.9%, LDL cholesterol is 98 mg/dL, GFR is 58 mg/g and their BP is 124/78. The provider recommends a referral to the RD and DSME program and writes a prescription for metformin XR 500mg daily and lovastatin 20mg. LR is worried about taking a statin because they heard it can cause dementia.
Based on the ADA Standards, what is the best response?
Click Here to Test your Knowledge
Join us live on May 16, 2023, at 11:30 am PST
We are living longer & more people are getting diabetes. The American Diabetes Association has updated the Older Adults Standards, with special attention to considering the reduction of medication & insulin therapy intensity. The older population has unique issues & special needs that require consideration as we provide diabetes self-management education. This online course highlights key areas of assessment, intervention, and advocacy for older clients living with diabetes.
Objectives:
Intended Audience: An important course for healthcare professionals seeking to gain an understanding of the special issues and goals for older adults.
Don’t worry if you can’t make it live. Your registration guarantees access to the recorded version in the Online University.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.