
Subscribe
eNewsletter
Ready to get certified?
Free CDCES Coach App
eNewsletter
Free CDCES Coach App
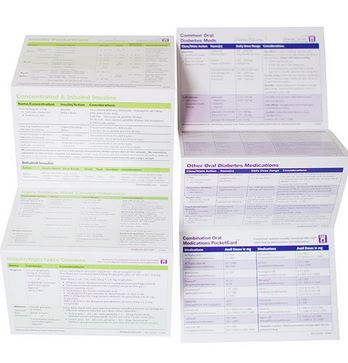
We have two updates to announce that have been captured in our electronic Medication PocketCards.
The DPP-IV Inhibitor Saxagliptin (Onglyza) and combination medication, Kombiglyze XR (saxagliptin/metformin extended-release tablets), have been permanently discontinued, according to manufacturer AstraZeneca.
A recent posting on the Food and Drug Administration’s (FDA) Drug Shortages tracker indicates that both products were discontinued because of a business decision and not due to safety or efficacy-related concerns.
There are three other DPP-IV inhibitors still available along with several combination versions. See our updated electronic ePocketCard that reflects this update.
In late 2022, the FDA approved the use of Dulaglutide (Trulicity for Pediatrics with Type 2 diabetes ages 10-17. Currently, metformin, insulin and the following GLP-1 RA’s are approved for pediatrics with type 2 diabetes, ages 10-17 See updated ePocketCard.
GLP-1 RA list of approved medications for pediatrics.
GLP-1 RAs have the benefit of not only lowering A1C, they also support weight loss and Exenatide XR and dulaglutide only need to be taken once a week. This weekly dosing can be a big advantage for busy families.
Our currently available laminated Diabetes Med PocketCards do not reflect these changes, but we will be reprinting later this year to reflect these updates.
This course will transform your test anxiety into calm self-confidence and test-taking readiness.

“Becoming a Certified Diabetes Care and Education Specialist (CDCES) is one of the best professional and personal decisions I have ever made.” – Coach Beverly Thomassian, RN, MPH, CDCES, BC-ADM
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.

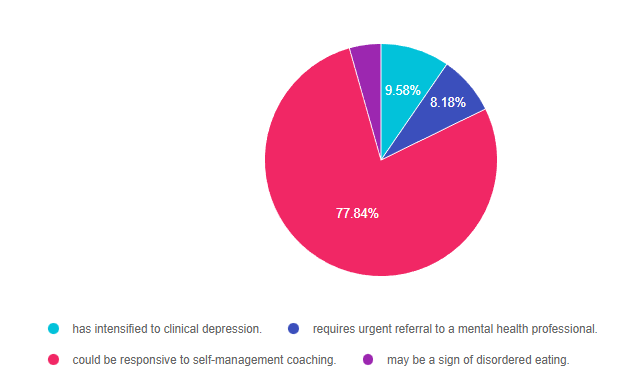
For last week’s practice question, we quizzed participants on diabetes distress. 78% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question: JR has type 1 diabetes and tells you, “My doctor just doesn’t seem to understand how to manage type 1 diabetes. Sometimes, I just skip my appointments because it feels like a waste of time.” JR’s most recent A1C was 8.7% and their time in ranges keeps decreasing with each visit.
Based on this, you realize that JR’s provider-related diabetes distress:
Answer Choices:
If you are thinking about taking the certification exam, this practice test question will set you up for success. Test writers anticipate possible answers based on the details in the question. They will wave those “juicy answers” right under your nose. Your job is to weed through the particulars, pluck out the most important elements, get rid of false answers, do any math very carefully and choose the BEST answer.
Answer 1 is incorrect. 9.58% chose this answer. “has intensified to clinical depression.” This is a tempting answer, but we don’t enough evidence to support that JR is struggling with depression. If we had JR complete the Diabetes Distress Scale, he would certainly score high on provider related distress based on this statement, “My doctor just doesn’t seem to understand how to manage type 1 diabetes. Sometimes, I just skip my appointments because it feels like a waste of time.” These comments certainly fit in the distress category. Through careful questioning and exploration, the diabetes educator could certainly help with problem solving.
Answer 2 is incorrect. 8.18% of you chose this answer. “requires urgent referral to a mental health professional.” Based on JR’s statement, “My doctor just doesn’t seem to understand how to manage type 1 diabetes. Sometimes, I just skip my appointments because it feels like a waste of time,” JR is certainly in distress. However, there is no language indicating that JR is in imminent danger of self-harm. Through careful questioning and exploration, the diabetes educator could certainly carefully assess JR’s mental health state and help with problem solving and referrals as needed.
Answer 3 is correct. About 77.84% of respondents chose this. “could be responsive to self-management coaching.” YES. This is the best answer. We could start by administering the Diabetes Distress Scale and then hone in on the high scoring areas. Then through careful questioning and exploration, the diabetes educator could certainly help with problem solving and identify if additional resources or referrals are needed.
Finally, Answer 4 is incorrect. 4.39% chose this answer. “may be a sign of disordered eating.” but we don’t enough evidence to support that JR is experiencing disordered eating. However, if we had JR complete the Diabetes Distress Scale, he would certainly score high on provider related distress based on this statement, “My doctor just doesn’t seem to understand how to manage type 1 diabetes. Sometimes, I just skip my appointments because it feels like a waste of time.”
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Addressing diabetes distress can be tricky, even for seasoned healthcare professionals.
We invite you to attend this hands-on training program that provides the essential steps to address diabetes distress combined with an innovative approach to glucose management. Our experts offer realistic strategies to address diabetes distress that you can immediately apply to your practice setting. Plus, the ReVive 5 Program provides a breadth of tools and resources to create more meaningful connections with people with diabetes.
“ReVive 5” breathes new life into our relationship with diabetes, bringing a fresh perspective to both the person with diabetes and the provider.
Team of Experts: ReVive 5 is taught by a team of 3 Interdisciplinary Experts:

Accredited Training Program:
Speakers Interviews – Learn more about the ReVive 5 Team
What is the Biggest Takeaway when Addressing Diabetes Distress? – Dr. Susan Guzman
Do you have to be a Mental Health Expert to Tackle Diabetes Distress? – Dr. Lawrence Fisher
Why I Transformed my Approach to Diabetes Self-Management Education- Coach Beverly
Don’t worry if you can’t make it live. Your registration guarantees access to the recorded version in the Online University.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
LR is 78 years old with a new diagnosis of diabetes. Their A1C is 7.9%, LDL cholesterol is 98 mg/dL, GFR is 58 mg/g and their BP is 124/78. The provider recommends a referral to the RD and DSME program and writes a prescription for metformin XR 500mg daily and lovastatin 20mg. LR is worried about taking a statin because they heard it can cause dementia.
Based on the ADA Standards, what is the best response?
Click Here to Test your Knowledge
Join us live on May 16, 2023, at 11:30 am PST
We are living longer & more people are getting diabetes. The American Diabetes Association has updated the Older Adults Standards, with special attention to considering the reduction of medication & insulin therapy intensity. The older population has unique issues & special needs that require consideration as we provide diabetes self-management education. This online course highlights key areas of assessment, intervention, and advocacy for older clients living with diabetes.
Objectives:
Intended Audience: An important course for healthcare professionals seeking to gain an understanding of the special issues and goals for older adults.
Don’t worry if you can’t make it live. Your registration guarantees access to the recorded version in the Online University.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.

Last year, we came up with a list of 10 Simple Steps to improve planetary health. Me and my family committed to making all 10 of these changes and I wanted to report on how we fared for the year. We weren’t perfect, but we definitely made some good progress! Check out our report below!
We are transforming our yard, plant by plant, with native species. The effort is paying off. The diversity of our bird and butterfly population has dramatically increased, along with a new host of amphibious friends.
By choosing plants that originated from your geographic area, you help support your regional ecosystem and offer pollinators, birds, butterflies, and other healthy critters needed food, pollen, and building materials for their survival.
Read more on our blog, Earth Day Secrets to Improving Planet Health
This year, we purchased a Lomi Composter from Pela Earth, and we love it. All of our food scraps go into the Lomi and from this food waste, nutrient-rich compost is created, and serves as the BEST fertilizer, ever. My house and outdoor plants have never looked so good!
My husband, a committed meat eater, recently discovered that his cholesterol was elevated. Overnight, he reached back in time and started cooking the vegetarian dishes of his Armenian grandparents. My kitchen has never smelled so good and the flavors coupled with joy, make each dish extra special. Plus, our fiber intake has dramatically increased and we are all learning more about traditional Armenian foods (so delicious).
In addition to walking out day outside with our furry friends, we needed a new car and decided to go completely electric. I can’t tell you how GREAT it feels to drive without creating emissions (and it’s so quiet). In addition, we have enough solar panels to charge our cars and rarely need to go to a charging station.
My husband and I have decreased our frequency of showering and have replaced the emitters in our yard to prevent water waste. Most of our plants are drought-tolerant too.
Cold water in the washer works as well as warm or hot water for most items. If the weather is bad, we toss wet clothes over chairs and over the headboard. We don’t hang everything to dry, but we are approaching 50%.
This is an ongoing goal that we keep working on. Our computers are on sleep at night, but we keep forgetting to turn them off.
As a family, we try to purchase used items and clothes whenever possible. In addition, we work on maintaining our appliances and other household gadgets to extend their life and avoid putting them into landfill.
Plastic is everywhere and is so hard to avoid. We first committed to no longer buying plastic water bottles and are trying to use refillable soaps, lotions, and other items. When shopping, we bring our reusable bags to the store. The next goal is to avoid buying fresh foods packaged in plastic.
We are at 50% of this goal. Since the new LED bulbs last so long, it has decreased the hassle of changing the bulbs and we love the wonderful light color choices too.
Please send us your stories too at [email protected]. We want to hear from you!
Each action, no matter how small, matters. We can do this!
With wishes for improved planetary health,
Beverly, Chris, Jackson, Robert and Choochi, and Maverick

Coach Beverly’s goal is to support our Diabetes Education Community and provide meaningful resources that are useful for your daily practice.
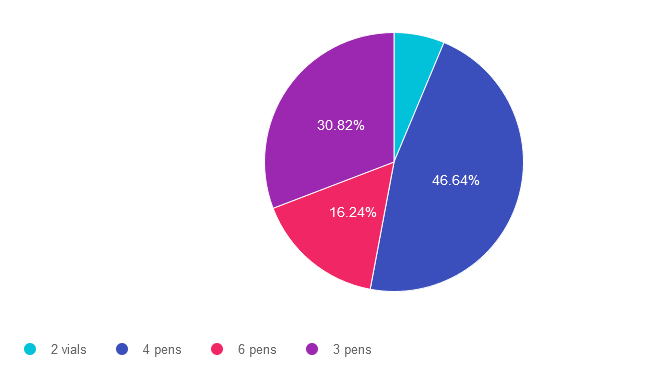
For last week’s practice question, we quizzed participants on counting every pen(ny.) 47% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question: KL takes 5-10 units of insulin glulisine (Apidra) based on an insulin scale before each of their 3 daily meals and 30 units of glargine (Basaglar) at bedtime.
Based on this information, how many u-100 glulisine (Apidra) insulin pens would KL use a month?
Answer Choices:
If you are thinking about taking the certification exam, this practice test question will set you up for success. Test writers anticipate possible answers based on the details in the question. They will wave those “juicy answers” right under your nose. Your job is to weed through the particulars, pluck out the most important elements, get rid of false answers, do any math very carefully and choose the BEST answer.
Answer 1 is incorrect. 6.31% chose this answer. “2 vials.” One way to quickly eliminate a wrong answer is to see if the units in the question match the units in the answer. The question asks, “How many pens” would JR need a month and this answer is in “vials”. We can cross this one off as false. **See complete math explanation below.
Answer 2 is correct. 46.64% of you chose this answer. “4 pens.” YES.. Great job. You not only calculated JR’s insulin needs, but added in extra insulin for priming too! **See complete math explanation below.
Answer 3 is incorrect. About 16.24% of respondents chose this. “6 pens.” This was a juicy answer that lured respondents into adding together the glulisine and glargine dose. The answer only asks for how many glulisine pens would JR need a month. **See complete math explanation below.
Finally, Answer 4 is incorrect. 30.82% chose this answer. “3 pens.” This was the juiciest answer of all. However, it doesn’t take into account the 2 units of insulin used to prime the pen before each injection. Also, if they had 3 pens of 300 units each, what if they made a mistake or wasted a dose, or needed a little extra.. they might be short on insulin. We always want to allow for a little cushion, just in case. **See complete math explanation below.
**Complete explanation – Doing the math.
If JR takes 5-10 units of insulin glulisine (Apidra) 3 times a day, we have to assume they will be taking the highest dose each time, so they don’t run out of insulin. That means JR uses 30 units a day of glulisine. 30 units a day x 30 days in a month = 900 units. But wait, JR needs to prime the pen first with a 2 unit “air shot” before each injection to make sure insulin is flowing through the needle before each of their 3 injections. So this means that JR is using up to 12 units of insulin 3 times a day or 36 units x 30 days = 1,080 units of glulisine a month. The next thing we need to know is that each U-100 glulisine pen holds 300 units of insulin (see our Insulin Storage Cheat Sheet 2023). Now, we can do the math. JR uses 1,080 units of insulin a day. Since each pen holds 300 units, we take 1080 and divide by 300 for a total of 3.6. This means JR will need 4 pens of glulisine each month to manage their diabetes.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Whether you are a novice or an expert in providing diabetes care, we invite you to attend this exciting training program that provides the essential steps to address diabetes distress combined with an innovative approach to glucose management that will revolutionize your practice.
“ReVive 5” breathes new life into our relationship with diabetes, bringing a fresh perspective to both the person with diabetes and the provider.
Team of Experts: ReVive 5 is taught by a team of 3 Interdisciplinary Experts:
Accredited Training Program:
Speakers Interviews – Learn more about the ReVive 5 Team
What is the Biggest Takeaway when Addressing Diabetes Distress? – Dr. Susan Guzman
Do you have to be a Mental Health Expert to Tackle Diabetes Distress? – Dr. Lawrence Fisher
Why I Transformed my Approach to Diabetes Self-Management Education- Coach Beverly
Don’t worry if you can’t make it live. Your registration guarantees access to the recorded version in the Online University.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.

For some people with diabetes, the thought of “exercise” can seem downright terrifying. We can help lift that fear by encouraging them to start with baby steps and substitute the term “activity” for “exercise”. Reassuring people that “any movement is better than no movement” allows them to shift their perspective and give themselves credit for something as simple as walking to the mailbox.
With spring in the air, it’s a perfect time to take a fresh approach to encourage activity.
The majority of people with diabetes are aware that regular activity is integral to diabetes self-care. With thoughtful coaching, we can support them to meet the target of 150 minutes of walking (or other activity) a week coupled with strength training.
Coach Beverly has outlined five strategies that she has found helpful in encouraging people to move more.
The goal is to accumulate about thirty minutes of activity a day, so taking a 10-minute walk after breakfast means they are one-third of the way there. Other activities that count include; gardening, housework, yard work, shopping, chasing kids, and those dance moves people do when no one is looking,
Starting and keeping new habits is challenging. By integrating activity into everyday life, people are likelier to keep it up. If the movement brings them joy, that is an added benefit. An excellent starting strategy is asking them what activities they like. Then explore if they can add it to their typical day. For example, taking a walk during a lunch break or hitting the gym before heading home. What about lifting weights with the kids or helping with after-dinner cleanup instead of relaxing in that favorite comfy chair? Joining an organized sport or dance class is also an option.
These simple sentences capture people’s attention and help them take that first step toward more movement. Please feel free to borrow and use these sayings in your practice!
Even the best-made plans may go differently than envisioned. Being ready for setbacks early on helps people set realistic expectations. As diabetes specialists, we can prepare people for obstacles and setbacks and remind them that a falter does not equal failure. According to Sylvia Gonsahn-Bollie, MD, assisting individuals to prepare for barriers with a PLAN helps for a quicker recovery.
PLAN stands for:
Encourage people to avoid black-and-white thinking, like, “Well, I missed my planned workout, so I might as well just give up.” Getting back on track as soon as possible keeps the momentum and prevents muscle deconditioning.
Regular physical activity can help prevent disease and improve well-being. Although exercise statistics are disheartening, improvement is possible. As health advocates, we can encourage systemic changes in health care and environmental changes in our neighborhoods to increase activity on a population level.
While waiting for more extensive changes, we have the power to equip individuals with personalized, actionable tools for improving and maintaining physical activity.
Our belief in people’s ability to get active is contagious. A person-centered collaborative approach can help people get moving, one step at a time.
Whether you are a novice or an expert in providing diabetes care, we invite you to attend this exciting training program that provides the essential steps to address diabetes distress combined with an innovative approach to glucose management that will revolutionize your practice.
“ReVive 5” breathes new life into our relationship with diabetes, bringing a fresh perspective to both the person with diabetes and the provider.
Team of Experts: ReVive 5 is taught by a team of 3 Interdisciplinary Experts:
Accredited Training Program:
Speakers Interviews – Learn more about the ReVive 5 Team
What is the Biggest Takeaway when Addressing Diabetes Distress? – Dr. Susan Guzman
Do you have to be a Mental Health Expert to Tackle Diabetes Distress? – Dr. Lawrence Fisher
Why I Transformed my Approach to Diabetes Self-Management Education- Coach Beverly
Don’t worry if you can’t make it live. Your registration guarantees access to the recorded version in the Online University.
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
JR has type 1 diabetes and tells you, “My doctor just doesn’t seem to understand how to manage type 1 diabetes. Sometimes, I just skip my appointments because it feels like a waste of time.” JR’s most recent A1C was 8.7% and their time in ranges keeps decreasing with each visit.
Based on this, you realize that JR’s provider-related diabetes distress
Click Here to Test your Knowledge
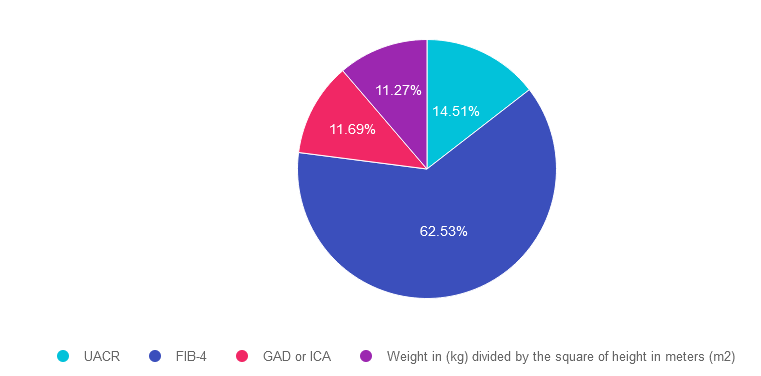
For last week’s practice question, we quizzed participants on being at risk for NASH. 63% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question: JR is 46 years old with type 2 diabetes and a BMI of 33. In addition, JR has hypertension and hyperlipidemia, with elevated liver enzymes (ALT and AST).
According to the latest ADA Standards, which of the following would best help determine if JR is at risk for liver fibrosis and cirrhosis?
Answer Choices:
If you are thinking about taking the certification exam, this practice test question will set you up for success. Test writers anticipate possible answers based on the details in the question. They will wave those “juicy answers” right under your nose. Your job is to weed through the particulars, pluck out the most important elements and choose the BEST answer.
Answer 1 is incorrect. 14.51% chose this answer. “UACR.” This is a juicy answer, however the Urinary Albumin Creatinine Ratio (UACR) evaluates kidney function and doesn’t provide any hepatic insights. Instead we would recommend the Fibrosis-4 Index for Liver Fibrosis helps determine risk of hepatic cirrhosis and inflammation (see answer 2).
Answer 2 is correct. 62.53% of you chose this answer. “FIB-4.” GREAT JOB. The Fibrosis-4 Index for Liver Fibrosis helps determine risk of hepatic cirrhosis and inflammation. By entering the person’s age, AST, ALT and Platelet count using the FIB-4 calculator, a risk level is calculated (see slide below). The hope is that by screening for hepatic issues early, we can take action to protect the liver and improve outcomes.
Answer 3 is incorrect. About 11.69% of respondents chose this. “GAD or ICA.” Although this answer is familiar, it does not match the intent of the question. GAD and ICA are blood tests to determine if someone has autoimmune mediated type 1 diabetes. Instead we would recommend the Fibrosis-4 Index for Liver Fibrosis helps determine risk of hepatic cirrhosis and inflammation (see answer 2).
Finally, Answer 4 is incorrect. 11.27% chose this answer. “Weight in (kg) divided by the square of height in meters (m2).” This answer is also familiar since it is the formula to determine a person’s body mass index (BMI). Instead we would recommend the Fibrosis-4 Index for Liver Fibrosis helps determine risk of hepatic cirrhosis and inflammation (see answer 2).
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity! Learn more by attending our Virtual Conference plus save $100 through April 18, 2023.

Your team is invited to our Virtual DiabetesEd™ Training Conference! Set your team apart and prepare for diabetes certification!
Join this state-of-the-art conference taught by content experts, Diana Isaacs, PharmD, BCPS, BCACP, BC-ADM, CDCES, Beverly Thomassian RN, MPH, CDCES, BC-ADM, and Ashley LaBrier who are passionate about improving diabetes care.
Group discounts are available!*
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.