Subscribe
eNewsletter
Ready to get certified?
Free CDCES Coach App
eNewsletter
Free CDCES Coach App
Like many health care professionals, I live with the shadows of early childhood trauma. We all manage these painful childhood events in different ways and their impact may only be discovered as we move into adulthood or even later in life. Recognizing and acknowledging our trauma and the trauma of the people we serve is an important first step toward healing.
As diabetes specialists, our awareness of trauma and toxic stress can lead to providing more informed and compassionate care. As health care providers, we may misperceive a person’s no-show or negative attitude as a sign that they don’t care about their diabetes self-care or the health consequences. With some exploration, we may gain a better understanding of the shadows that are blocking their path forward.

Adverse Childhood Experiences (ACEs) are common. At least two-thirds of people living in the U.S. have experienced one ACE and over 15% have experienced 4 or more.
Furthermore, a dose-response relationship exists: as the number of adverse experiences increases so does the risk of problems from childhood through adulthood.
These childhood traumas can lead to toxic stress which, over time, can change the biology of our body and increase the risk of diabetes, heart disease, and more.
People with elevated ACE scores are more likely to experience a variety of mental health issues, which is not surprising given their painful, confusing, and unsafe childhoods. Based on sound research by the CDC and Kaiser, they are also more likely to suffer from physical diseases, like heart attack and stroke, diabetes, and cancer. They are more likely to break bones and experience unintended pregnancies.
There is hope for healing. Diabetes specialists can make a difference. Through the use of screening tools and careful listening to the words and body language of the individuals we serve, we can start the movement toward healing and collaborative working relationships.

Adverse childhood experiences (ACE) are associated with an increased risk of diabetes, heart disease, cancer, and a variety of other health consequences for adults. This session reviews how diabetes care and education specialists can provide screening, assessment, and trauma-informed care to individuals who experienced ACEs and are living with toxic stress. We will explore strategies to address ACES and improve outcomes for individuals and communities. Throughout, we will focus on supporting self-care with a focus on recognizing and promoting resilience.
Topics include:
Want to learn more about ACEs and Healing?
ADCES National Virtual Meeting – Ready for Viewing
California Coordinating ADCES Chapter – September 30, 2021 at 4:45pm PST
Diabetes Ed Services Webinars – he Impact of Adverse Childhood Experiences on Health: A Personal Story of Resilience & Hope with Coach Beverly
ACE Screening Tool and Resilience Inventory
Becoming ACE-Aware Training Program
Nadine Burke Harris, MD TED Talk on How Childhood Trauma affects health
NPR Article – Take the ACE Score and Learn what it does and doesn’t mean
Trauma-Informed Care Fact Sheet
Why should I care about my number?
CDC Vital Signs – Impact of ACES
CDC Mortality and Morbidity Weekly Report on ACEs – 2019
What happened to you? Conversations on Trauma, Resilience, and Healing – authors Oprah Winfrey and Bruce D. Perry, M.D., Ph.D.
Did you miss the live conference? No worries! You can register now to watch on-demand
Whether you are new to diabetes or a seasoned expert, you’ll benefit from this virtual conference with the latest research plus critical content that you can immediately apply to your clinical practice.
If you are seeking a state-of-the-art review of current diabetes care, this course is for you. Our team has been fine-tuning this course for over fifteen years, and we know what you need. This program can also be a great addition to your CDCES or BC-ADM exam study plan.
Team of expert faculty includes:
In addition to informative lectures, we also use group activities and case studies to highlight the essential knowledge, skills, and strategies needed to succeed in diabetes education today!

CEs: Includes over 30 CEs
Program Info: 2021 Diabetes Educator Course Flyer & Schedule (subject to change)
Speakers: View Conference Faculty.
Dates: Your registration fee includes access to FREE podcast and all recorded webinars for one year.
Two Registration Options
Virtual DiabetesEd Specialist Conference Deluxe | Oct. 6-8 | 30+ CEs
Deluxe Virtual Program for $459 includes:
+Plus Syllabus, Standards and Swag:
2021 Diabetes Educator Course Flyer & Schedule (subject to change)
Virtual DiabetesEd Specialist Conference Basic | Oct. 6-8 | 30+ CEs
Basic virtual program for $359 includes:
2021 Diabetes Educator Course Flyer & Schedule (subject to change)
Team of Experts: Our team of expert faculty has been fine-tuning this course for over fifteen years and we know what you need to succeed! In addition to informative lectures, we also use group activities and case studies to highlight the essential knowledge, skills, and strategies needed to succeed in diabetes education today!
When you register for our Virtual Course, you have immediate access to these Bonus DiabetesEd University Online Courses – for FREE!
2021 Diabetes Educator Course Flyer & Schedule (subject to change)
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
HM is living with type 2 diabetes and is 90 years old with a BMI of 32. HM’s most recent A1c was 9.3% and their GFR is 16. The provider stopped the metformin due to the diminished kidney function and HM is currently on no diabetes medications. To manage HM’s blood sugar, the provider ordered a low-calorie restrictive meal plan for HM. HM was a chef for 40 years and tells you, “they feel hungry” all the time. Based on this assessment, you decide to contact the provider.
Which of the following would be the best suggestion?
Click here to test your knowledge!
Want to learn about this question and more as you’re studying for the CDCES Exam?
This bundle includes our CDCES Online Prep Bundle (featured above) plus the ADCES Review Guide – 5th Edition-Revised. The online bundle includes Level 1, Level 2, and Level 3 (Boot Camp), plus two bonus courses. The ADCES Review Guide offers over 480+ practice questions and is a fantastic independent study tool and comprehensive resource for the Diabetes Care and Education Specialist Exam.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
Adverse childhood experiences (ACE) are associated with an increased risk of diabetes, heart disease, cancer and a variety of other health consequences for adults. This session reviews how diabetes care and education specialists can provide screening, assessment, and trauma-informed care to individuals who experienced ACEs and are living with toxic stress. We will explore strategies to address ACES and improve outcomes for individuals and communities. Throughout, we will focus on supporting self-care with a focus on recognizing and promoting resilience.
Topics include:
Watch Webinar for FREE
This option does not come with CEs.
Purchase for $19
This includes access to the recorded version of this webinar on your Online University Student Portal and 1.0 CE.
Intended Audience: This course is a knowledge-based activity designed for individuals or groups of diabetes educators, including RNs, RDs, Pharmacists, Nurse Practitioners, Clinical Nurse Specialists, Physician Assistants, and other health care providers interested in enhancing their diabetes medication knowledge.
Instructor: Beverly Thomassian RN, MPH, CDCES, BC-ADM is a working educator and a nationally recognized diabetes expert.
*Certified Diabetes Care and Education Specialist® and CDCES® are registered marks owned by NCBDE. The use of DES products do not guarantee successful passage of the CDCES® exam. NCBDE does not endorse any preparatory or review materials for the CDCES® exam, except for those published by NCBDE.”
JR is a 33-year-old who is non-binary and was recently diagnosed with type 2 diabetes. During your assessment, JR asks if diabetes can affect their sexual health.
What is the best response?
Click here to test your knowledge!
Want to learn more about this topic and more?
Whether you are new to diabetes or a seasoned expert, you’ll benefit from this virtual conference with the latest research plus critical content that you can immediately apply to your clinical practice.
If you are seeking a state-of-the-art review of current diabetes care, this course is for you. Our team has been fine-tuning this course for over fifteen years, and we know what you need. This program can also be a great addition to your CDCES or BC-ADM exam study plan.
Team of expert faculty includes:
In addition to informative lectures, we also use group activities and case studies to highlight the essential knowledge, skills, and strategies needed to succeed in diabetes education today!
CEs: Includes over 30 CEs
Program Info: 2021 Diabetes Educator Course Flyer & Schedule (subject to change)
Speakers: View Conference Faculty.
Dates: Your registration fee includes access to FREE podcast and all recorded webinars for one year.
Two Registration Options
Virtual DiabetesEd Specialist Conference Deluxe | Oct. 6-8 | 30+ CEs
Deluxe Virtual Program for $459 includes:
+Plus Syllabus, Standards and Swag:
2021 Diabetes Educator Course Flyer & Schedule (subject to change)
Virtual DiabetesEd Specialist Conference Basic | Oct. 6-8 | 30+ CEs
Basic virtual program for $359 includes:
2021 Diabetes Educator Course Flyer & Schedule (subject to change)
Team of Experts: Our team of expert faculty has been fine-tuning this course for over fifteen years and we know what you need to succeed! In addition to informative lectures, we also use group activities and case studies to highlight the essential knowledge, skills, and strategies needed to succeed in diabetes education today!
When you register for our Virtual Course, you have immediate access to these Bonus DiabetesEd University Online Courses – for FREE!
2021 Diabetes Educator Course Flyer & Schedule (subject to change)
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.

Our September 21st Question of the week quizzed test takers on Intensive Insulin Therapy with A1c 6.2%. Three quarters (74%) of respondents, chose the best answer. We are excited to share info so you can pass on correct info to people living with diabetes and your colleagues.
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer below: Answer Question
Question: HR is a 78-year-old with a stroke and limited cognition with diabetes for 8 years and is on intensive insulin therapy: HR takes bolus insulin at meals and basaglar at night. HR has an A1c is 6.2% and employs a part time caretaker.
What is the best response in this situation?
Answer Choices:
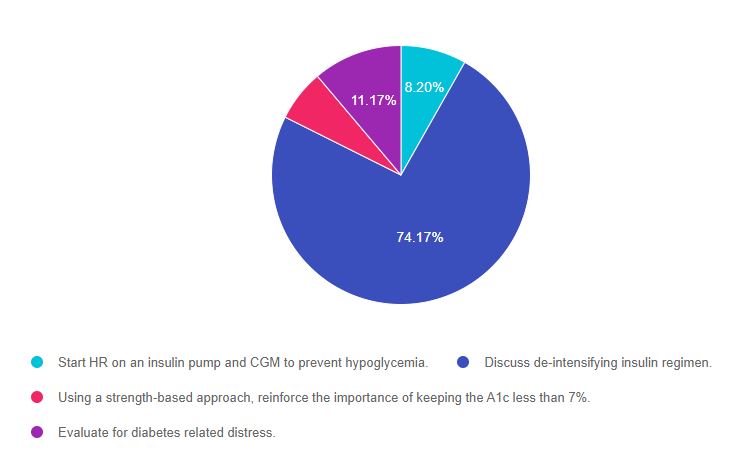
As shown above, the most common choice was option 2, the second most common answer was option 4, then option 1, and finally option 3.
If you are thinking about taking the certification exam, it is helpful to know the goals of care and considerations for people with diabetes across the lifespan. This practice test question will set you up for success. Test writers anticipate possible answers based on the details in the question. They will wave those “juicy answers” that seem so familiar to you, right under your nose. Your job is to weed through the to choose the BEST answer.
Answer 1 is incorrect. 8.20% chose this answer, “Start HR on an insulin pump and CGM to prevent hypoglycemia.” This is not the best answer because we want to provide person-centered care based on the unique situation of this individual. HR has a history of a stroke, limited cognition and relies on a part time caregiver. It doesn’t seem realistic to provide pump and CGM training to HR given the cognitive limitations and the caregiver is only part-time. It is unlikely that the two of them would be comfortable enough or have the skill level to help oversee this complex technology and changing insertion sites.
Answer 2 is correct. 74.17% of you chose this answer, “Discuss de-intensifying insulin regimen.” YES. This is the best answer. Since HR is on multiple daily injections and has an A1c in the low 6% range, we know they are most likely experiencing episodes of hypoglycemia. To address this, we would need to discuss goals of care with HR and their caregivers and share our concerns about the risk and danger of hypoglycemia. We need to de-intensify this management plan. Based on the outcome of the discussion with HR, this could be accomplished by: reducing the overall insulin dose, switching to twice a day 70/30 insulin, or evaluating if oral medications could be trialed to reduce the need for insulin.
Answer 3 is incorrect. 6.46% of respondents chose this answer, “Using a strength-based approach, reinforce the importance of keeping the A1c less than 7%.” Using a strength-based approach is always a good idea, but the main issue in this question is that HR’s A1c is only 6.2%. According to the ADA Standards of Care, the A1c target in this situation would be individualized based on safety considerations, quality of life, and the goals and values of the person living with diabetes. For older, frail individuals at risk of hypoglycemia, a safer A1c target would be 7% – 8%.
Finally, Answer 4 is incorrect. 11.17% chose this answer, “Evaluate for diabetes-related distress.” Even though it is always important to consider people’s emotional response to diabetes, this answer does not address the key issue presented in this question. The first priority would be to make sure HR is safe, with a reduced risk of hypoglycemia and a realistic insulin regimen.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Did you miss the live conference? No worries! You can register now to watch on-demand
Whether you are new to diabetes or a seasoned expert, you’ll benefit from this virtual conference with the latest research plus critical content that you can immediately apply to your clinical practice.
If you are seeking a state-of-the-art review of current diabetes care, this course is for you. Our team has been fine-tuning this course for over fifteen years, and we know what you need. This program can also be a great addition to your CDCES or BC-ADM exam study plan.
Team of expert faculty includes:
In addition to informative lectures, we also use group activities and case studies to highlight the essential knowledge, skills, and strategies needed to succeed in diabetes education today!
CEs: Includes over 30 CEs
Program Info: 2021 Diabetes Educator Course Flyer & Schedule (subject to change)
Speakers: View Conference Faculty.
Dates: Your registration fee includes access to FREE podcast and all recorded webinars for one year.
Two Registration Options
Virtual DiabetesEd Specialist Conference Deluxe | Oct. 6-8 | 30+ CEs
Deluxe Virtual Program for $459 includes:
+Plus Syllabus, Standards and Swag:
2021 Diabetes Educator Course Flyer & Schedule (subject to change)
Virtual DiabetesEd Specialist Conference Basic | Oct. 6-8 | 30+ CEs
Basic virtual program for $359 includes:
2021 Diabetes Educator Course Flyer & Schedule (subject to change)
Team of Experts: Our team of expert faculty has been fine-tuning this course for over fifteen years and we know what you need to succeed! In addition to informative lectures, we also use group activities and case studies to highlight the essential knowledge, skills, and strategies needed to succeed in diabetes education today!
When you register for our Virtual Course, you have immediate access to these Bonus DiabetesEd University Online Courses – for FREE!
2021 Diabetes Educator Course Flyer & Schedule (subject to change)
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
As a diabetes specialist at a local hospital, one of your quality improvement goals is to prevent nocturnal hypoglycemia.
Which of the of following policy changes would most likely lower rates of overnight and morning hypoglycemia?
Click here to test your knowledge!
Did you miss the live conference? No worries! You can register now to watch on-demand
Whether you are new to diabetes or a seasoned expert, you’ll benefit from this virtual conference with the latest research plus critical content that you can immediately apply to your clinical practice.
If you are seeking a state-of-the-art review of current diabetes care, this course is for you. Our team has been fine-tuning this course for over fifteen years, and we know what you need. This program can also be a great addition to your CDCES or BC-ADM exam study plan.
Team of expert faculty includes:
In addition to informative lectures, we also use group activities and case studies to highlight the essential knowledge, skills, and strategies needed to succeed in diabetes education today!
CEs: Includes over 30 CEs
Program Info: 2021 Diabetes Educator Course Flyer & Schedule (subject to change)
Speakers: View Conference Faculty.
Dates: Your registration fee includes access to FREE podcast and all recorded webinars for one year.
Two Registration Options
Virtual DiabetesEd Specialist Conference Deluxe | Oct. 6-8 | 30+ CEs
Deluxe Virtual Program for $459 includes:
+Plus Syllabus, Standards and Swag:
2021 Diabetes Educator Course Flyer & Schedule (subject to change)
Virtual DiabetesEd Specialist Conference Basic | Oct. 6-8 | 30+ CEs
Basic virtual program for $359 includes:
2021 Diabetes Educator Course Flyer & Schedule (subject to change)
Team of Experts: Our team of expert faculty has been fine-tuning this course for over fifteen years and we know what you need to succeed! In addition to informative lectures, we also use group activities and case studies to highlight the essential knowledge, skills, and strategies needed to succeed in diabetes education today!
When you register for our Virtual Course, you have immediate access to these Bonus DiabetesEd University Online Courses – for FREE!
2021 Diabetes Educator Course Flyer & Schedule (subject to change)
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
Did you know that Toujeo U-300 insulin pens are good for 56 days once opened? And that the max dose for Tresiba U-200 FlexTouch Pen is 160 units?
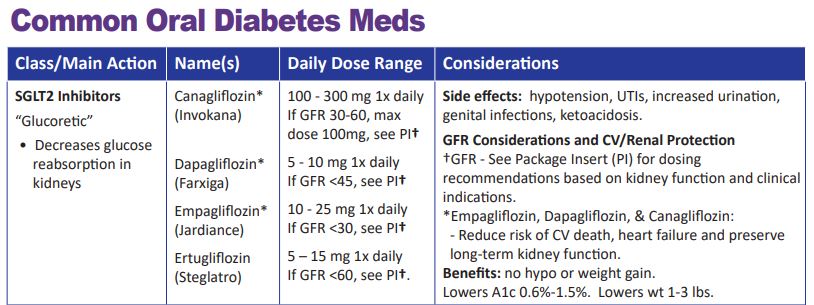
For our latest version of our printed PocketCards, we now include the number of pens in a box, max injection dose, total insulin amount per pen, and shelf life on the Concentrated Insulin Card. We also added Lyumjev KwikPen u200 insulin.
When determining the best insulin for people taking concentrated insulins, shelf life, max dosing, and total units of insulin in each device are important considerations.
We have also updated the GFR parameters for SGLT2 Inhibitors. This class of medication not only substantially lowers blood glucose but also has a profound impact on renal protection.
As more trial data become available, the GFR cutoff levels may change, so periodically refer to the package insert (PI) or our DES electronic pocket care version, for the most up-to-date information.
We update the printed version of our PocketCard once or twice a year.
We update our electronic PocketCard on an ongoing basis.
Fortunately, we can immediately update our electronic version of the PocketCard on our website and CDCES Coach App to reflect the latest medication recommendations and guidelines. In the electronic version, we also include that the GLP-1 Exenatide (Bydureon) is now approved for peds, age 10 and older and the GFR cut-off for empagliflozin is now approved for a GFR 30 or greater (please see package insert for details).

Becoming Board Certified in Advanced Diabetes Management (BC-ADM) provides an opportunity for diabetes specialists with an advanced degree in their field (plus a professional license as an advanced practice nurse, registered dietitian, registered pharmacist, or provider) to increase the breadth and depth of their diabetes knowledge. The scope of advanced diabetes practice includes management skills such as medication adjustment, medical nutrition therapy, exercise planning, counseling for behavior management, and psychosocial issues.
Attaining optimal diabetes management includes using a person-centered approach coupled with assessment, screening, management, and monitoring of acute and chronic diabetes co conditions. This webinar will review changes in requirements for this year’s exam eligibility and test format, strategies to succeed along with a review of study tips and test-taking tactics. We will review sample test questions and the reasoning behind choosing the right answers. We hope you can join us for this webinar.
Can’t make it live? All paid registrants are guaranteed access to the video presentation, handouts and podcasts.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
Our September 14th Question of the week quizzed test takers on a new med. Less than half, 47% of respondents, chose the correct answer. This was a hard question since this finerenone was only recently FDA approved. We are excited to share info about this med along to you, so you can pass on correct info to people living with diabetes and kidney disease.
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer below: Answer Question
Question: JR has a GFR of 43 and lives with type 2 diabetes. JR excitedly brings you an article that talks about finerenone (Kerendia), a newly approved non-steroidal mineralocorticoid receptor antagonist which is indicated for people with chronic kidney disease (CKD) associated with Type 2 diabetes.
If JR is started on this medication, what instruction would you provide?
Answer Choices:
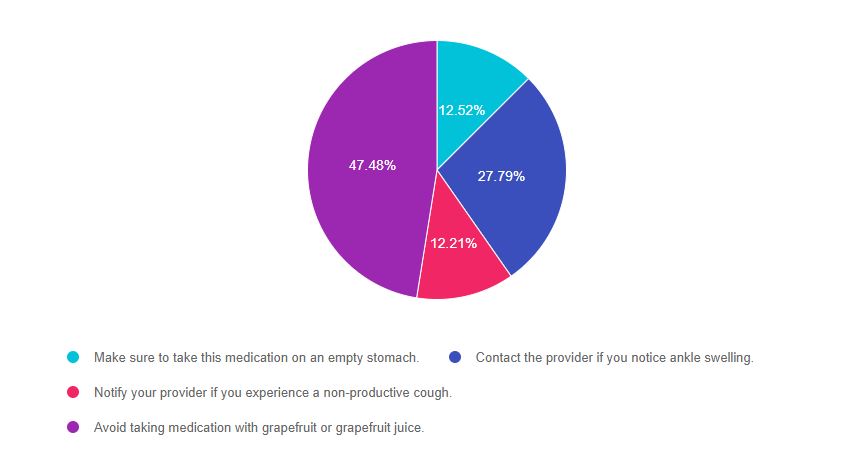
As shown above, the most common choice was option 3, the second most common answer was option 1, then option 4, and finally option 2.
If you are thinking about taking the certification exam, it is helpful to know about newly approved diabetes medications, although it may take at least a year to appear in exams. However, this practice test question will set you up for success. Test writers anticipate possible answers based on the details in the question. They will wave those “juicy answers” that seem so familiar to you, right under your nose. Your job is to weed through the to choose the BEST answer.
Answer 1 is incorrect. 12.5% chose this answer, “Make sure to take this medication on an empty stomach.” If you don’t know anything about a particular medication and are forced to guess, this answer is pretty unlikely to be the best answer, for one reason. Most meds don’t need to be taken on an empty stomach. Two diabetes related meds, levothyroxine and oral semaglutide DO need to be taken on an empty stomach, but an empty stomach is not required for most other meds. Finerenone can be taken with or without food.
Answer 2 is incorrect. 27.8% of you chose this answer, “Contact the provider if you notice ankle swelling.” This was another juicy answer that we purposefully included. There is a class of diabetes medications, the TZDs (pioglitazone and rosiglitazone) that can cause ankle swelling, so this answer might have seemed familiar to you. Also when trying to find false answers, you may want to consider that it seems unlikely that a medication that slows kidney failure would have edema as a side effect.
Answer 3 is incorrect. 12.2% chose this answer, “Notify your provider if you experience a non-productive cough.” This juicy answer goes with a common blood pressure medication class, ACE Inhibitors, that people with diabetes are often prescribed to manage hypertension. With finerenone, the major consideration is monitoring the potassium in the first month of initiation.
Answer 4 is correct. 47.5% of respondents chose this answer, “Avoid taking medication with grapefruit or grapefruit juice.” GREAT JOB, this is the best answer. Since finerenone is a CYP3A4 substrate, the package insert recommends to avoid taking finerenone with other strong cype3A4 inhibitors. It also advises to avoid taking finerenone with grapefruit or grapefruit juice. Great job!
Check out our New Updated Med Cheat Sheets 2021 (page 2) and consider attending our Virtual Conference with Dr. Diana Isaacs, who will speak more to this topic. You can also check out our Blog Post on New Meds for Diabetes.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
Did you miss the live conference? No worries! You can register now to watch on-demand
Whether you are new to diabetes or a seasoned expert, you’ll benefit from this virtual conference with the latest research plus critical content that you can immediately apply to your clinical practice.
If you are seeking a state-of-the-art review of current diabetes care, this course is for you. Our team has been fine-tuning this course for over fifteen years, and we know what you need. This program can also be a great addition to your CDCES or BC-ADM exam study plan.
Team of expert faculty includes:
In addition to informative lectures, we also use group activities and case studies to highlight the essential knowledge, skills, and strategies needed to succeed in diabetes education today!
CEs: Includes over 30 CEs
Program Info: 2021 Diabetes Educator Course Flyer & Schedule (subject to change)
Speakers: View Conference Faculty.
Dates: Your registration fee includes access to FREE podcast and all recorded webinars for one year.
Two Registration Options
Virtual DiabetesEd Specialist Conference Deluxe | Oct. 6-8 | 30+ CEs
Deluxe Virtual Program for $459 includes:
+Plus Syllabus, Standards and Swag:
2021 Diabetes Educator Course Flyer & Schedule (subject to change)
Virtual DiabetesEd Specialist Conference Basic | Oct. 6-8 | 30+ CEs
Basic virtual program for $359 includes:
2021 Diabetes Educator Course Flyer & Schedule (subject to change)
Team of Experts: Our team of expert faculty has been fine-tuning this course for over fifteen years and we know what you need to succeed! In addition to informative lectures, we also use group activities and case studies to highlight the essential knowledge, skills, and strategies needed to succeed in diabetes education today!
When you register for our Virtual Course, you have immediate access to these Bonus DiabetesEd University Online Courses – for FREE!
2021 Diabetes Educator Course Flyer & Schedule (subject to change)
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.