
Subscribe
eNewsletter
Ready to get certified?
Free CDCES Coach App
eNewsletter
Free CDCES Coach App
A diagnosis of diabetes often carries a significant emotional response. A person with diabetes might report shame, fear, and guilt as they come to terms with their diagnosis and anticipate their future. As diabetes healthcare providers, we can learn to address these feelings while helping people move forward!

This cheat sheet provides a dozen simple coaching strategies for providers to help people believe in their ability to self-manage their diabetes successfully.
Using a person-centered approach, we can identify the individual’s strengths and expertise and then leverage this information to open a door of possibilities. Our choice of communication techniques can spark behavior change in people living with diabetes.
Adopting this style of communication can be a dramatic shift for some providers. Think of it this way: In usual care, the diabetes healthcare provider steers the boat, brings the fuel, and charts the course. Using the person-centered approach, the provider is simply the rudder, serving as a guide, and the individual steers.
DO: Mindfully Listen to the individuals’ problems and fears.
The first strategy is carefully listening to the person’s fears and concerns. If someone struggles with nutrition, meds, or behavioral changes, listen to the struggle, and try not to push, advise, or fix it. Listen and reflect on what you think is happening for the first few minutes.
For example, reflecting back could go something like this: “Taking medications is hard for you because you are not sure if they are really working.” Or, “It’s hard to eat more vegetables because you are a long-haul truck driver.” Or, “It sounds like you blame yourself for having diabetes.”
Listening and then reflecting back on the struggles of the individual is the first phase of energizing the visit.
DO: Focus on curiosity before exploring possible changes in behavior.
With a person-centered approach, spend more time in the “curiosity” phase before moving to the “action” phase.”
We might ask, “As a truck driver, I am curious to learn more about your food choices when driving.” As care providers, we may be slightly overanxious to get to the “action” phase, which involves aspects such as action, planning, goal setting, and looking at specific foods and exercise prescriptions. It can be disorienting for providers to delay the “action” phase and spend most of the time exploring the “curiosity” phase, and there’s a perception that it takes longer. In fact, it’s probably more efficient with time. It’s a redistribution of the provider’s time in that more time is spent listening to the individual’s barriers and fears and responding to them.
Curiosity can provide comfort and open the door to insights.
DO: Listen for individual insights and ideas.
After reflecting on the person’s struggles and feelings, the next phase is the “building change” talk. It combines having the person express how a behavior change would benefit them and realistic ways to move to the action phase.
As genuinely curious providers we ask, “what are your ideas about how you can improve this situation?” Then the provider would listen carefully to what the person shares. Along with the struggles and barriers, the individual might say, “I could buy a veggie tray before heading out in my truck,” or “I could try taking my medication every day for a week to see how they affect my blood sugars.”
We want to fine-tune our listening skills so that we can pick up the scent of the trail. People often allude to what they’re willing to do and drop crumbs when they feel safe and heard during the conversation. All we need to do is pick up on the hints and encourage them down the path.
DO: Ask Questions and Collaborate.
Once the individual has identified their motivation and begins brainstorming on ways to make behavior changes, the door is open for respectful collaboration. You’ll want to explore how much change the individual is willing and able to make at that time.
To keep it real and achievable, we start with a very small step by saying, “So, you think you could buy a vegetable tray before heading out?” or “You think you could take your diabetes meds for a week to see if they work?” and let that sit; let the person describe their thoughts and feelings.
Then we might say, “How, if at all, do you see this plan fitting into your life?” We are careful to avoid any form of prescription or declaration and stick with asking questions. If the person volunteers—”I will monitor my blood sugars for a week to see if these diabetes meds work.” Or “I think I could pick up veggie trays on driving days.” We would absolutely reinforce and support these choices.
AVOID: Pressure, fix, or control.
A person-centered approach energizes individuals to take the lead in managing their condition, in step with their providers and supporters. We are careful to avoid forced solutions or controlling language. As providers, we feel like we have these great ideas that we are sure will fix the person, if only…. However, the truth is, our job is to help the person with diabetes find their own answers and solutions.
Let’s stop “Shoulding” on people.
It’s time to let go of terms like “You must, you should, you have to, it’s better, it’s important, do it for me” since they fall under the category of “controlling motivation”—which can be hurtful and lead to the individual becoming defensive or shutting down. We avoid controlling language because it elicits resistance and defiance. The literature is quite clear about people doing something because someone made them feel guilty, ashamed, or pressured them. The long-term prognosis for behavior change using this approach is underwhelming.
DON’T employ Scare Tactics.
As providers, we genuinely care about people’s health and may try to energize behavior change using fear. Such as, “If you don’t get your A1C down, you are heading for dialysis or amputation.” or “Don’t you want to see your kids grow up?” We don’t generally motivate people by scaring them since research shows it is ineffective, and they may never return for that follow-up appointment.
Short-term, people are usually willing to make changes when they’re terrified—when they first get diagnosed–but that wanes in a relatively short period of time. The question is how to keep the person energized when the initial fear has worn off.
Making behavior changes, like losing weight or adjusting lifelong eating habits, can be extremely difficult.
Find a way to recognize and affirm their efforts even if there is no or little change in clinical measures.
If someone’s A1C has not moved, but they took their medications daily or ate their vegetables, we say, “Wow, I want to recognize the effort you put into this.”
Respond kindly and compassionately to their disappointment, frustration, and fear. It won’t fix the immediate problem, but it helps the person feel that their effort was well-spent. It helps them feel heard instead of just “fixing it” and saying, “Okay, we’ll try a new medication.” Over time, your empathy builds bridges and trust, leading to long term collaboration and better health.
About the author – Coach Beverly has been fine-tuning her guilt-free approach to diabetes education for over 30 years and has witnessed its impact on improving well-being and building connections.
Learn more about effective communication approaches in our ReVive 5 Diabetes Training Program.
Inspired by https://www.niddk.nih.gov/health-information/professionals/diabetes-discoveries-practice/motivational-interviewing-dos-dont
You are welcome to Download Effective Person-Centered Communication Approaches Cheat Sheet to share with your colleagues.
Inspired by https://www.niddk.nih.gov/health-information/professionals/diabetes-discoveries-practice/motivational-interviewing-dos-donts

A diagnosis of diabetes often carries a significant emotional response. People with diabetes experience a myriad of feelings as they come to terms with their diagnosis and anticipate their future. As diabetes healthcare providers, we can learn to address these feelings through person centered coaching and help individuals take steps to get to their best health.
This Coaching Cheat Sheet provides a dozen simple coaching strategies for providers to help people believe in their ability to self-manage their diabetes successfully.

Using a person-centered approach, we can identify the individual’s strengths and expertise and then leverage this information to open a door of possibilities. Our choice of communication techniques can spark behavior change in people living with diabetes.
Adopting this style of communication can be a dramatic shift for some providers. Think of it this way: In usual care, the diabetes healthcare provider steers the boat, brings the fuel, and charts the course. Using the person-centered approach, the provider is simply the rudder, serving as a guide, and the individual steers.
DO: Mindfully Listen to the individuals’ problems and fears.
The first strategy is carefully listening to the person’s fears and concerns. If someone struggles with nutrition, meds, or behavioral changes, listen to the struggle, and try not to push, advise, or fix it. Listen and reflect on what you think is happening for the first few minutes.
For example, reflecting back could go something like this: “Taking medications is hard for you because you are not sure if they are really working.” Or, “It’s hard to eat more vegetables because you are a long-haul truck driver.” Or, “It sounds like you blame yourself for having diabetes.”
DO: Focus on curiosity before exploring possible changes in behavior.
With a person-centered approach, spend more time in the “curiosity” phase before moving to the “action” phase.”
We might ask, “As a truck driver, I am curious to learn more about your food choices when driving.” As care providers, we may be slightly overanxious to get to the “action” phase, which involves aspects such as action, planning, goal setting, and looking at specific foods and exercise prescriptions. It can be disorienting for providers to delay the “action” phase and spend most of the time exploring the “curiosity” phase, and there’s a perception that it takes longer. In fact, it’s probably more efficient with time. It’s a redistribution of the provider’s time in that more time is spent listening to the individual’s barriers and fears and responding to them.
DO: Listen for individual insights and ideas.
After reflecting on the person’s struggles and feelings, the next phase is the “building change” talk. It combines having the person express how a behavior change would benefit them and realistic ways to move to the action phase.
As genuinely curious providers we ask, “what are your ideas about how you can improve this situation?” Then the provider would listen carefully to what the person shares. Along with the struggles and barriers, the individual might say, “I could buy a veggie tray before heading out in my truck,” or “I could try taking my medication every day for a week to see how they affect my blood sugars.”
We want to fine-tune our listening skills so that we can pick up the scent of the trail. People often allude to what they’re willing to do and drop crumbs when they feel safe and heard during the conversation. All we need to do is pick up on the hints and encourage them down the path.
DO: Ask Questions and Collaborate.
Once the individual has identified their motivation and begins brainstorming on ways to make behavior changes, the door is open for respectful collaboration. You’ll want to explore how much change the individual is willing and able to make at that time.
To keep it real and achievable, we start with a very small step by saying, “So, you think you could buy a vegetable tray before heading out?” or “You think you could take your diabetes meds for a week to see if they work?” and let that sit; let the person describe their thoughts and feelings.
Then we might say, “How, if at all, do you see this plan fitting into your life?” We are careful to avoid any form of prescription or declaration and stick with asking questions. If the person volunteers—”I will monitor my blood sugars for a week to see if these diabetes meds work.” Or “I think I could pick up veggie trays on driving days.” We would absolutely reinforce and support these choices.
AVOID: Pressure, fix, or control.
A person-centered approach energizes individuals to take the lead in managing their condition, in step with their providers and supporters. We are careful to avoid forced solutions or controlling language. As providers, we feel like we have these great ideas that we are sure will fix the person, if only…. However, the truth is, our job is to help the person with diabetes find their own answers and solutions.
It’s time to let go of terms like “You must, you should, you have to, it’s better, it’s important, do it for me” since they fall under the category of “controlling motivation”—which can be hurtful and lead to the individual becoming defensive or shutting down. We avoid controlling language because it elicits resistance and defiance. The literature is quite clear about people doing something because someone made them feel guilty, ashamed, or pressured them. The long-term prognosis for behavior change using this approach is underwhelming.
DON’T employ Scare Tactics.
As providers, we genuinely care about people’s health and may try to energize behavior change using fear. Such as, “If you don’t get your A1C down, you are heading for dialysis or amputation.” or “Don’t you want to see your kids grow up?” We don’t generally motivate people by scaring them since research shows it is ineffective, and they may never return for that follow-up appointment.
Short-term, people are usually willing to make changes when they’re terrified—when they first get diagnosed–but that wanes in a relatively short period of time. The question is how to keep the person energized when the initial fear has worn off.
In Conclusion: Celebrate and Recognize Each Person’s Effort
Making behavior changes, like losing weight or adjusting lifelong eating habits, can be extremely difficult.
Find a way to recognize and affirm their efforts even if there is no or little change in clinical measures.
If someone’s A1C has not moved, but they took their medications daily or ate their vegetables, we say, “Wow, I want to recognize the effort you put into this.”
Respond kindly and compassionately to their disappointment, frustration, and fear. It won’t fix the immediate problem, but it helps the person feel that their effort was well-spent. It helps them feel heard instead of just “fixing it” and saying, “Okay, we’ll try a new medication.” Over time, your empathy builds bridges and trust, leading to long term collaboration and better health.
About the author – Coach Beverly has been fine-tuning her guilt-free approach to diabetes education for over 30 years and has witnessed its impact on improving well-being and building connections.
Learn more about effective communication approaches in our ReVive 5 Diabetes Training Program.
Inspired by https://www.niddk.nih.gov/health-information/professionals/diabetes-discoveries-practice/motivational-interviewing-dos-dont
You are welcome to Download Effective Person-Centered Communication Approaches Cheat Sheet to share with your colleagues.
Inspired by https://www.niddk.nih.gov/health-information/professionals/diabetes-discoveries-practice/motivational-interviewing-dos-donts

While the celebration of Dr. King is global, its spirit is local. As Dr. King said, “Everyone can be great, because everyone can serve” and there is no better way to honor his legacy than through individual and community service.
As Diabetes Specialists, we honor Dr. King’s words by serving people living with prediabetes and diabetes. We advocate for affordable diabetes care, medications, and access to nutritious foods.
We are fully aware that people with diabetes are more likely to struggle with food insecurity, social and financial inequities and lack adequate resources to pay for medications and diabetes supplies. We know that there is still much work to be done. During these challenging times, I am comforted by Dr. King’s resonant statement “The arc of the moral universe is long, but it bends toward justice.”
On this day of national celebration and service, we thank Dr. King for being a beacon of light and clarity with his call to action that still resonates today.
With Gratitude,
Coach Beverly
Sign up for Diabetes Blog Bytes – . It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]
To recognize Indigenous Peoples’ Day, we are honored to share a treasured poem by one of my favorite poets and writers, Joy Harjo. Plus, we also share an interactive map of Indigenous Lands (credit to NPR).
In 2019, Joy Harjo was recognized as the United States poet laureate and served three terms. Harjo is an internationally renowned performer and writer of the Muscogee (Creek) Nation.
She lives in Tulsa, Oklahoma and is the author of nine books of poetry, including the highly acclaimed An American Sunrise, several plays and children’s books, and two memoirs, Crazy Brave and Poet Warrior. Her many honors include the Ruth Lily Prize for Lifetime Achievement from the Poetry Foundation, the Academy of American Poets Wallace Stevens Award, two NEA fellowships, and a Guggenheim Fellowship.
You can learn more about Joy Harjo on her webpage, www.joyharjo.com.
Joy Harjo
Remember the sky that you were born under,
know each of the star’s stories.
Remember the moon, know who she is.
Remember the sun’s birth at dawn, that is the
strongest point of time. Remember sundown
and the giving away to night.
Remember your birth, how your mother struggled
to give you form and breath. You are evidence of
her life, and her mother’s, and hers.
Remember your father. He is your life, also.
Remember the earth whose skin you are:
red earth, black earth, yellow earth, white earth
brown earth, we are earth.
Remember the plants, trees, animal life who all have their
tribes, their families, their histories, too. Talk to them,
listen to them. They are alive poems.
Remember the wind. Remember her voice. She knows the
origin of this universe.
Remember you are all people and all people
are you.
Remember you are this universe and this
universe is you.
Remember all is in motion, is growing, is you.
Remember language comes from this.
Remember the dance language is, that life is.
Remember.
Indigenous Peoples’ Day is a time of reflection, recognition and celebration of the role Native people have played in U.S. history. One way to mark the day — and to learn about Indigenous history year-round — is to learn which Native lands you live on.



In 1976, President Gerald Ford started officially recognizing Black History Month during the celebration of the Bicentennial. Black History Month is now celebrated all across the country in educational institutions, centers of Black culture, and community centers, both great and small.
President Ford urged Americans to “seize the opportunity to honor the too-often neglected accomplishments of Black Americans in every area of endeavor throughout our history”.

As a new, slightly goofy nurse working at UCLA Medical Center in the 1980s, I was developing my sense of who I wanted to become as a professional. My style was relaxed and informal and I was often arrived to work a few minutes late.
Later that year, I started graduate school and transferred to the night shift. That’s when I met Ms. Davis, who role-modeled the professional I wanted to become.
Ms. Davis was the only black nurse in our unit and she commanded respect. As a charge nurse, she arrived to work early and listened intently to the report, taking careful notes. Her crisp white uniform, sparkling white shoes, and nurse’s cap pinned proudly on her head inspired me to be better. As a matter of fact, I got my nurse’s cap down from it’s a shelf and started wearing it again, along with shining my shoes and arriving on time.

We never called Ms. Davis by her first name and we never questioned why. We understood that she had earned our deference and respect.
As a new nurse, I had plenty of questions, which Ms. Davis answered with kindness, never making me feel embarrassed or inferior. She was knowledgeable, hard-working, and a natural leader. I was excitable and known to overreact in crisis situations. Ms. Davis’s role modeled calm composure coupled with swift and deliberate action.
Once Ms. Davis found me crying in the break room.
One of my patients had a constricting trachea, gradually stopping airflow, that no surgery would repair. I was devastated and in despair. Ms. Davis wrapped her arms around me and patted my back. This moment might have lasted for seconds or minutes. It didn’t matter, her hug seemed to set my world right again.
Thank you Ms. Davis for showing me what I could become. You are one of my most influential role models as a professional nurse. Your presence, grace, and dignity are etched in my memory forever.
In gratitude,
Coach Beverly
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
This month we are celebrating our amazing sister organization, Just One Person.
Just One Person is a sustainable model program that prepares girls in rural Kenya for post-secondary opportunities, supporting their development towards economic independence. Diabetes Education Services donates the profit from the sale of the Pancreas Pillow to help fund school scholarships and seminars for other girls in rural Kenya.

Mwanaidi’s story:
Mwanaidi, of Just One Person, has hand-sewn hundreds of beautiful Pancreas Partners in her hometown in Kenya and shipped them to the Diabetes Education Services office in California, so we can share them with you.
While Mwanaidi was waiting for admission to college she began sewing the “pancreas pillows” that Diabetes Education Services sells in the US. She used a donated treadle sewing machine, a pattern designed by Just One Person (JOP) Executive Director, Emma Sisia, and traditional leso cloth.

Mwanaidi joined the Just One Person (JOP) project in rural Kenya after her high school recognized her potential. Mwanaidi graduated from high school in 2010 and subsequently, became a certified chef. She uses the income from her job to help support her family of 7 siblings along with her mother and father.
After paying Mwanaidi for her beautiful work, Diabetes Education Services donates the profit from the sale of the Pancreas Pillow to help fund school scholarships and seminars for other girls in rural Kenya. Other alumnae of JOP have followed suit and are continuing to produce these wonderful pillows to help ensure the sustainability of our program.
Just One Person’s philosophy is that girls are members of our organization for life. They are committed to sharing their knowledge and resources with their mothers, sisters, neighbors, and daughters for generations to come.
At Diabetes Education Services we are dedicated to supporting the growth and well-being of our future generations.
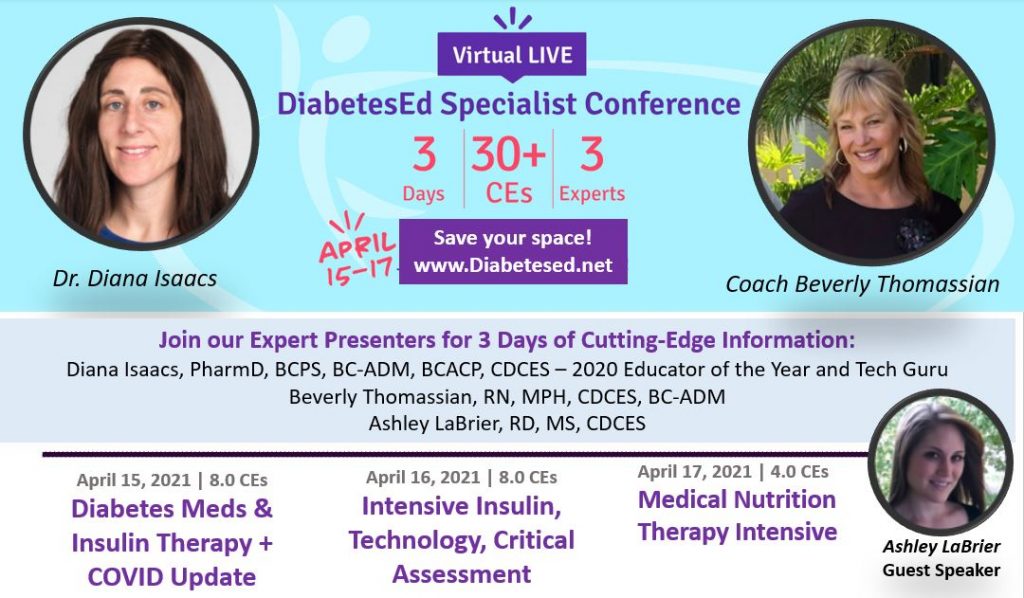
Save your spot for our
Virtual DiabetesEd Specialist Conference | April 15-17, 2021
Whether you are new to diabetes or a seasoned expert, you’ll benefit from this virtual conference with the latest research plus critical content that you can immediately apply to your clinical practice. If you are interested in taking the CDCES or BC-ADM exam or are seeking a state-of-the-art review of current diabetes care, this course is for you.
Entire Program Fee: $399
Dates: April 15-17, 2021
3 Expert Speakers
CEs: 30+ CE hours
Live Webinar Schedule: All webinars start and end times are in Pacific Standard Time
Come join our Virtual DiabetesEd Specialist Program.
Team of expert faculty includes:
In addition to informative lectures, we also use group activities and case studies to highlight the essential knowledge, skills, and strategies needed to succeed in diabetes education today!
Prepare for CDCES or BC-ADM certification or earn hours for renewal.
Your registrations include access to all the Online Sessions plus Bonus Courses through December 31st, 2021.
This virtual program includes:
3 day live webinar courses from April 15th-17th (20 CEs) + enrollment in our Bonus Bundle (14.0+ CEs) from now through December 2021.
View full Conference Schedule and Faculty.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
[yikes-mailchimp form=”1″]
Accreditation: Diabetes Education Services is an approved provider by the California Board of Registered Nursing, Provider 12640, and Commission on Dietetic Registration (CDR), Provider DI002. Since these programs are approved by the CDR it satisfies the CE requirements for the CDCES regardless of your profession.*
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
by Robert Frost
Have you ever taken the road less traveled? What did you learn about yourself and would you take that road again?
Two roads diverged in a yellow wood,
And sorry I could not travel both
And be one traveler, long I stood
And looked down one as far as I could
To where it bent in the undergrowth;
Then took the other, as just as fair,
And having perhaps the better claim,
Because it was grassy and wanted wear;
Though as for that the passing there
Had worn them really about the same,
And both that morning equally lay
In leaves no step had trodden black.
Oh, I kept the first for another day!
Yet knowing how way leads on to way,
I doubted if I should ever come back.
Two roads diverged in a wood, and I—
I took the one less traveled by,
And that has made all the difference.
I shall be telling this with a sigh
Somewhere ages and ages hence:
Two roads diverged in a wood, and I—
I took the one less traveled by,
And that has made all the difference.
