
Subscribe
eNewsletter
Ready to get certified?
Free CDCES Coach App
eNewsletter
Free CDCES Coach App

For last week’s practice question, we quizzed participants on having their cake and eating it too. A whopping 94% of respondents chose the best answer. We want to celebrate your success and give you all a shout out for a job well done.
Before we start though if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question: AJ is a 9-year-old with type 1 diabetes, A1c of 7.2%, and uses an insulin pump and CGM. They ask you how to include a piece of birthday cake for an upcoming birthday celebration.
What is the best advice?
Answer Choices:
If you are thinking about taking the certification exam, this practice test question will set you up for success. Test writers anticipate possible answers based on the details in the question. They will wave those “juicy answers” right under your nose. Your job is to weed through the particulars, pluck out the most important elements and choose the BEST Person-Centered answer.
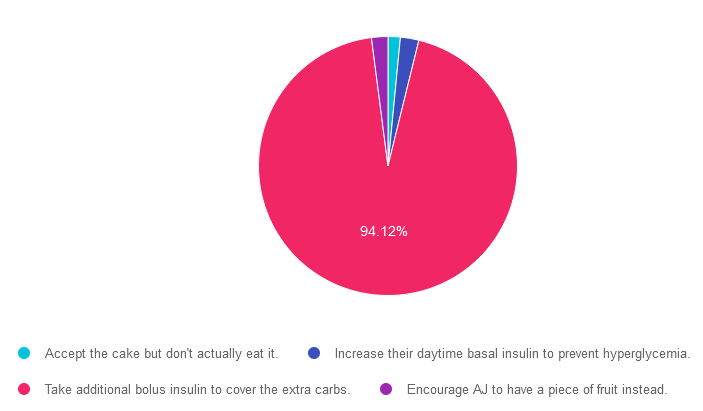
Answer 1 is incorrect. 1.53% chose this answer. “Accept the cake but don’t actually eat it.” Since this doesn’t honor AJ’s choice to accept and enjoy the cake, it is not the best answer. People with diabetes can absolutely enjoy special treats by adjusting their bolus insulin dose to account for the extra carbs to prevent post cake hyperglycemia.
Answer 2 is incorrect. 2.3% of you chose this answer. “Increase their daytime basal insulin to prevent hyperglycemia.” People with diabetes can absolutely enjoy special treats by adjusting their bolus insulin dose to account for the extra carbs to prevent post cake hyperglycemia.
Answer 3 is correct. About 94.12% of respondents chose this. “Take additional bolus insulin to cover the extra carbs.” YAY! This person centered approach is the BEST guilt free answer since it recognizes and respects AJ’s choice to enjoy a piece of birthday cake while still managing blood sugars with extra bolus insulin.
Finally, Answer 4 is incorrect. 2.05% chose this answer. “Encourage AJ to have a piece of fruit instead.” Since this doesn’t honor AJ’s choice to accept and enjoy the cake, it is not the best answer. People with diabetes can absolutely enjoy special treats by adjusting their bolus insulin dose to account for the extra carbs to prevent post cake hyperglycemia.
We hope you appreciate this week’s person-centered rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
You are invited to join our Virtual Conference with our Nutrition expert speaker, Ashley LaBrier, MS, RD, CDCES, who will be providing a half-day presentation on this important topic!

Ashley LaBrier, MS, RD, CDES, is an innovator in the field of diabetes, nutrition, and technology. Ashley is a consultant and the Diabetes Education Program Coordinator at the Salinas Valley Medical Clinic’s Diabetes & Endocrine Center.
Ms. LaBrier is passionate about providing person-centered education to empower those who live with diabetes. Having been diagnosed with type 1 diabetes herself nearly 20 years ago, she combines her professional knowledge with personal experience and understanding.

Whether you are new to diabetes or a seasoned expert, you’ll benefit from this virtual conference with the latest research plus critical content that you can immediately apply to your clinical practice.
If you are seeking a state-of-the-art review of current diabetes care, this course is for you. Our team has been fine-tuning this course for over fifteen years, and we know what you need. This program can also be a great addition to your CDCES or BC-ADM exam study plan.
Group discounts are available!*
Download Course Flyer | Download Schedule
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.

This course will transform your test anxiety into calm self-confidence and test-taking readiness.
She will also review sample test questions and the reasoning behind choosing the right answers. We hope you can join us.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
“Why do you say “pregnant people” in your webinars?”
A few years ago, we recognized that we were not including everyone in the conversation when discussing prenatal care in our standards course so we made the shift of changing the language from “Women & Diabetes” to “Pregnancy & Diabetes.”

While the majority of people who become pregnant are women, we know that gender-diverse people and transmen can also become pregnant and including them in discussions around prenatal care is important. We also recognize that the experience of being a parent and/or giving birth varies widely for both cis and trans people; some women who are mothers adopted their children, used a surrogate, or their partner gave birth to their children, while others who give birth are gender-diverse, trans, two-spirit, or intersex and don’t identify as a woman.
Gender-inclusive terms for pregnancy and birthing are not new. Lesbian parents have long distinguished between birth and non-birth mothers, a practice that appears in over a decade of academic literature. In uncoupling gender from a body’s ability to gestate and birth a child, we note that adoptive mothers, cisgender lesbian non-birth mothers and trans mothers who were assigned male at birth (AMAB) all engage in mothering activities and typically identify as mothers.
Recognizing and renaming in obstetrics: How do we take better care with language?
Whether we provide services in the hospital, clinic, or other outpatient settings, we can take steps to help the people we work with feel welcome.
As Diabetes Educators, we recognize the importance of language in providing person-centered care to best support people living with diabetes and prenatal care is no different.
There are a few small changes we can make to provide inclusive care for all people. As we outlined above, “mother” may not fit each and every person who is giving birth and someone might identify as a mother who hasn’t given birth. Because of this, we can change “mother” in our language to “parent” or shift “woman” to “people” when speaking generally about pregnancy.
To make our practices more welcoming, we can establish All Gender Restrooms and update our materials to use gender-inclusive language. Here is a list of terms and tips for shifting this language and creating more inclusive practices.
The easiest way to become more inclusive in our language which respects the autonomy of each individual to describe themselves and their bodies is to give them opportunities to share with us what those terms are and how they would like to be referred to.
A few ways you can do this are by expanding the ways we collect this information in our intake forms or discussing it with the individual in their initial appointment. You can incorporate sections to ask for someone’s pronouns or even a body map where someone can make notes about preferred language that is used around their bodies and pregnancy. Giving space to outline triggering or preferred language for each person can empower not only gender-diverse people but can also support trauma survivors of all genders.
By paying careful attention to each person’s experience from the moment they walk in the door until we say goodbye, we can find ways to create a more inclusive environment. This awareness of the details is the great first step to showing your care and respect for those you work with.
Resources
ADCES Inclusive Care for LGBTQ+ People with Diabetes Handout – this handout provides definitions, terms to avoid, and a cultural competency checklist to help you move towards improving inclusivity within your practice.
ADA’s Considerations for Transgender People With Diabetes
Focus on Forms and Policy: Creating an Inclusive Environment for LGBT Patients by the National LGBT Health Education Center
Diabetes Prevention and Management for LGBTQ+ People Handout – this handout includes research of diabetes within the LGBTQ+ community, along with clinical considerations, programs, and resources for diabetes educators to use within their practice.
Policies on Lesbian, Gay, Bisexual, Transgender & Queer (LGBTQ+) issues – this resource by the American Medical Association lists all the current healthcare policies in place for the LGBTQ+ community.
Helio’s LGBTQ+ Health Updates Resource Center – this is a “collection of news articles and features that provide the latest information on the unique health needs of individuals in the LGBTQ+ community.”
Several studies over the last decade support that post-meal blood sugars can be improved by changing the order of the foods eaten. By starting with vegetables and protein foods, then moving to carbohydrates, participants across studies experienced a significant improvement in postprandial blood glucose levels. This simple adjustment of food order provides people living with diabetes with an easy tool to reach glucose targets.
In a 2015 study published in Diabetes Care, a dozen subjects were fed the same meal of grilled chicken, ciabatta bread, orange juice, lettuce, and tomato salad plus steamed broccoli with butter on two different days. The researchers measured glucose and insulin levels before food ingestion and 30, 60, and 120 min after the start of the meal.
When vegetables and protein were consumed first, before carbohydrates, compared with the reverse food order, there was a 28.6% decrease in average post-meal glucose. The authors concluded that “the temporal sequence of carbohydrate ingestion during a meal has a significant impact on postprandial glucose and insulin excursions”.
The simple action of eating veggies and protein leads to improvement in glycemia through optimal timing of carbohydrate consumption during a meal.

In a different study where researchers recruited 15 participants from Weill Cornell Medical College. Participants consumed the same meal for 3 days changing the three separate food-type orders: carbohydrate, protein, and vegetables.
As with the previous study, researchers found that “although all baseline fasting glucose concentrations were similar, glucose levels were decreased at 30 and 60 minutes after the protein and vegetable first order.”
In addition, the vegetable first meal order resulted in lower glucose levels at 30 and 60 minutes than the carbohydrate first meal order. Researchers found that the vegetable first meal pattern reduced insulin excursions and that incremental AUC for insulin was 43.8% lower than for the carbohydrate first meal order.
Researchers say the reason for improved glucose is complicated, but is probably due to a combination of factors. Eating protein and veggies first may stimulate the early release of GLP-1 hormones and consuming fiber-rich vegetables can slow down carbohydrate digestion.
Fiber Foods – the Unsung Heroes
The benefits of fiber have been supported by over 100 years of research. Studies reveal that eating more fiber can lower your risk of developing serious illness over time.
“When compared with those who consume very little fiber, people at the high end of the fiber-eating spectrum saw their risk for dying from heart disease, stroke, type 2 diabetes and/or colon cancer plummet by 16 to 24 percent, investigators reported.”
Exciting enough, the more fiber a person consumed, the risk of developing those illnesses continued to decrease. The range of illnesses that a higher intake of fiber seemed to impact surprised scientists.
Researchers say that American’s on average, eat less than 15 grams of fiber per day. However, increasing intake to 25-29 gms per day is just “adequate.” The more fiber a person incorporates in their diet, the greater the decrease in the overall risk of early death.
Every additional 15-gram bump in daily whole grain intake was found to curtail an individual’s overall risk of early death — as well as their risk of early death from heart disease — by between 2 and 19 percent.
Researchers also found that increasing fiber intake had no risky health effects and that it is never too late to start embracing fiber every day!
“When considering all the trials of increasing fiber intakes, those participants that did reduce both their body weight and the total cholesterol in their blood, two important predictors of disease.”
Although none of these discoveries are surprising, scientists hope this will lead to changes in dietary recommendations. “This is just one more piece of evidence that supports and further solidifies the recommendations registered dietitian nutritionists have been making for years,” said Sandon.
It is never too late to start eating healthy and fiber may be a great starting point for many!
Here are some common foods and their fiber content:
Please see our Plant-Based Eating Resource Page for more info!
Your team is invited to our Virtual DiabetesEd™ Training Conference! Set your team apart and prepare for diabetes certification!
Join this state-of-the-art conference taught by content experts, Diana Isaacs, PharmD, BCPS, BCACP, BC-ADM, CDCES, Beverly Thomassian RN, MPH, CDCES, BC-ADM, and Ashley LaBrier who are passionate about improving diabetes care.
Group discounts are available!*
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
For last week’s practice question, we quizzed participants on post-meal glucose spikes. 51% of respondents chose the best answer. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question: TR can’t figure out why her BG always spikes after breakfast.
How many grams of carb is in the following breakfast? 2 corn tortillas, 2 fried eggs with salsa, ½ cup hashbrowns and an 8 ounce glass of milk.
Answer Choices:
If you are thinking about taking the certification exam, this practice test question will set you up for success. Test writers anticipate possible answers based on the details in the question. They will wave those “juicy answers” right under your nose. Your job is to weed through the particulars, pluck out the most important elements and choose the BEST answer.
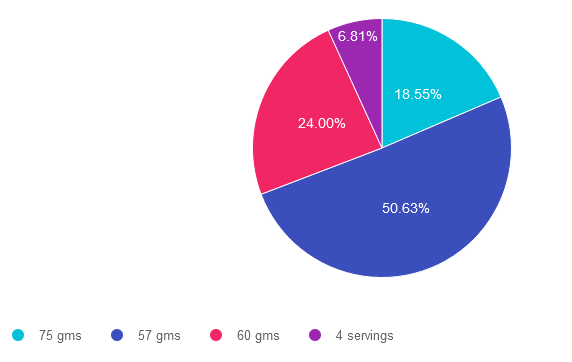
Answer 1 is incorrect. 18.55% chose this answer, “75 gms”. To answer this question accurately, it is important to be familiar with the common servings sizes of carbs and to know which foods don’t count as carbs. This answer is incorrect because it is an over estimate of carbs in this meal.
Answer 2 is correct. 50.63% of you chose this answer, “57 gms”. Yes, this is the BEST Answer. GREAT JOB. Here are the carbs broken down. 2 corn tortillas = 30gms carb, 2 fried eggs with salsa= 0 gms carb, ½ cup hashbrowns – 15 gms and an 8 ounce glass of milk =12gms. 30 + 15+ 12 = 57 gms of carbohydrate in this meal. An important fact to keep in mind for exam success; a cup of milk is 12 gms of carb, not 15gms.
Answer 3 is incorrect. About 24% of respondents chose this, “60 gms” This was the juicy answer. An important fact to keep in mind for exam success; a cup of milk is 12 gms of carb, not 15gms. Here are the carbs broken down. 2 corn tortillas = 30gms carb, 2 fried eggs with salsa= 0 gms carb, ½ cup hashbrowns – 15 gms and an 8 ounce glass of milk =12gms. 30 + 15+ 12 = 57 gms of carbohydrate in this meal.
Finally, Answer 4 is incorrect. 6.81% chose this answer, “4 servings” This answer is tempting, but the question asks “how many gms of carbohydrate” not, how many servings of carb. A great idea is to always eliminate answers that don’t match the unit of measure used in the question.
If you want more info on carb counting, you are invited to join our Virtual Conference in April. Save $100 through April 7, 2023 (see info below). We hope you appreciate this week’s rationale!
You are invited to join our Virtual Conference with our Nutrition expert speaker, Ashley LaBrier, MS, RD, CDCES, who will be providing a half-day presentation on this important topic!
Ashley LaBrier, MS, RD, CDES, is an innovator in the field of diabetes, nutrition, and technology. Ashley is a consultant and the Diabetes Education Program Coordinator at the Salinas Valley Medical Clinic’s Diabetes & Endocrine Center.
Ms. LaBrier is passionate about providing person-centered education to empower those who live with diabetes. Having been diagnosed with type 1 diabetes herself nearly 20 years ago, she combines her professional knowledge with personal experience and understanding.
Whether you are new to diabetes or a seasoned expert, you’ll benefit from this virtual conference with the latest research plus critical content that you can immediately apply to your clinical practice.
If you are seeking a state-of-the-art review of current diabetes care, this course is for you. Our team has been fine-tuning this course for over fifteen years, and we know what you need. This program can also be a great addition to your CDCES or BC-ADM exam study plan.
Group discounts are available!*
Download Course Flyer | Download Schedule
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.
AJ is a 9-year-old with type 1 diabetes, A1c of 7.2%, uses an insulin pump and CGM. They ask you how to include a piece of birthday cake for an upcoming birthday celebration.
What is the best advice?
Click Here to Test your Knowledge
Your team is invited to our Virtual DiabetesEd™ Training Conference! Set your team apart and prepare for diabetes certification!
Join this state-of-the-art conference taught by content experts, Diana Isaacs, PharmD, BCPS, BCACP, BC-ADM, CDCES, Beverly Thomassian RN, MPH, CDCES, BC-ADM, and Ashley LaBrier who are passionate about improving diabetes care.
Group discounts are available!*
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.

The ADA Standards serve as the definitive clinical handbook for diabetes care professionals. We rely on it to provide evidence-based guidelines and promote best practices.
Have you ever wondered who reviews and updates these standards every year? It is a group of expert ADA member volunteers who are hand-picked based on their extensive knowledge and contributions to the field of diabetes. They dedicate hundreds of hours to this important task and we are very grateful for their hard work and careful review.
Below is a list of the 21 authors for the Standards of Care and ninth on the list is our esteemed guest speaker at our Virtual DiabetesEd Training Conference in April 26-28, 2023.
Diana Isaacs, PharmD, BCPS, BC-ADM, BCACP, CDCES presents for the Virtual Conference for two full days (April 26 & 27th), walking participants through the nitty gritty of the standards, with an effortless fluidity while summarizing key points in the most understandable terms.
On the first day of the Virtual Conference, Dr. Diana Isaacs and Coach Beverly Thomassian tag-team through the 17 ADA Standards, adding in clinical insights, case studies, and plenty of poll questions to test your knowledge in real-time!
On the second day of the Virtual Conference, Diana does a wonderful show and tell demonstrating insulin delivery devices, pumps and CGMs and other gadgets. Plus, she just returned from the International Technology Conference and has lots of exciting updates to share with all of you.
Day 1 – Topics covered by Dr. Diana Isaacs
Day 2 – Topics covered by Dr. Diana Isaacs
Your team is invited to our Virtual DiabetesEd™ Training Conference! Set your team apart and prepare for diabetes certification!
Join this state-of-the-art conference taught by content experts, Diana Isaacs, PharmD, BCPS, BCACP, BC-ADM, CDCES, Beverly Thomassian RN, MPH, CDCES, BC-ADM, and Ashley LaBrier who are passionate about improving diabetes care.
Group discounts are available!*
All hours earned count toward your CDCES Accreditation Information
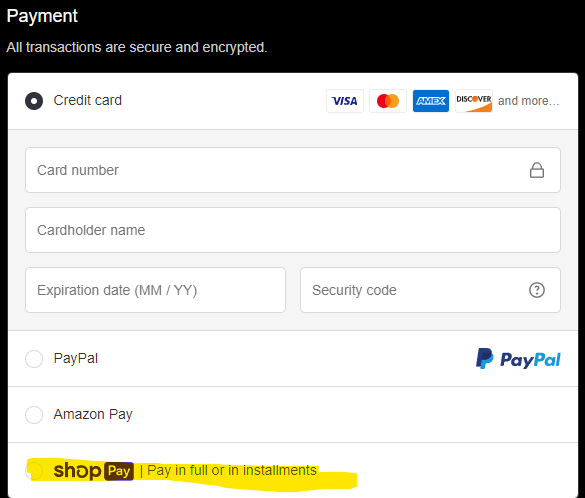
Many of you have requested to set up payment plans for your orders and we have found a great solution for this! During checkout, on the payment page, you can now select “Shop Pay” to pay in 3 installments instead of just one payment.
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparator
For last week’s practice question, we quizzed participants on their nutrition label reading ability. About 59% of respondents chose the best answer, revealing how challenging nutrition labels can be to dissect and understand, even for super-smart health care professionals. We want to clarify and share this important information, so you can pass it on to people living with diabetes and your colleagues, plus prepare for exam success!
Before we start though, if you don’t want any spoilers and haven’t tried the question yet, you can answer it below: Answer Question
Question: You are teaching about counting fat.
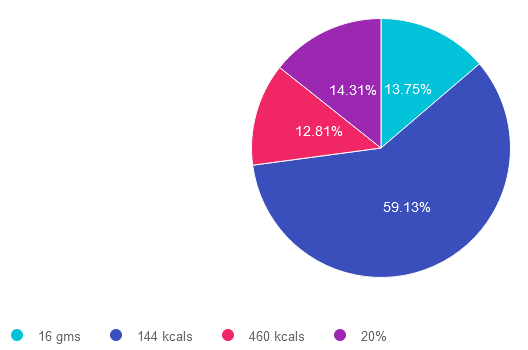
If they ate 2 servings of this Macaroni and Cheese (see label), how many calories would come from total fat?
Answer Choices:

If you are thinking about taking the certification exam, this practice test question will set you up for success. Test writers anticipate possible answers based on the details in the question or image (like this nutrition label). They will wave those “juicy answers” right under your nose. Your job is to weed through the particulars, pluck out the most important elements and choose the BEST answer.
Answer 1 is incorrect. 13.75% chose this answer. “16 gms.” While it is true that there are 16 grams of fat in 2 servings of macaroni and cheese, this question doesn’t ask the test taker, “how many grams of fat”. The intent of the question is to determine how many kcals from total fat. Right away, we know this answer is wrong, because the unit is in gms not kcals.
Answer 2 is correct. 59.13% of you chose this answer. “144 kcals.” GREAT JOB. To get to this answer, you have to do a little math and know one important fact; there are 9 kcals in 1 gm of fat. On this label, one serving of macaroni and cheese has 8 gms, so 2 servings has 16 gms of total fat. 16 gms x 9 kcals = 144 kcals. In preparation for certification exams (and providing nutrition counseling), knowing how to read labels and being familiar with the kcals for protein, carbs and fats is very helpful.
Answer 3 is incorrect. About 12.81% of respondents chose this. “460 kcals.” This would be the correct answer if the question read, “how many total calories” is in 2 servings of this macaroni and cheese. However, the question is only asking for total fat calories in 2 servings. To get to best answer, you have to do a little math and know one important fact; there are 9 kcals in 1 gm of fat. On this label, one serving of macaroni and cheese has 8 gms, so 2 servings has 16 gms of total fat. 16 gms x 9 kcals = 144 kcals.
Finally, Answer 4 is incorrect. 14.31% chose this answer. “20%.” While it is true that there is 20% total fat in 2 servings of macaroni and cheese, this question doesn’t ask the test taker, “what percent of fat”. The intent of the question is to determine how many kcals from total fat. Right away, we know this answer is wrong, because the unit is in % not kcals.
We hope you appreciate this week’s rationale! Thank you so much for taking the time to answer our Question of the Week and participate in this fun learning activity!
You are invited to join our Virtual Conference with our Nutrition expert speaker, Ashley LaBrier, MS, RD, CDCES, who will be providing a half-day presentation on this important topic!
Ashley LaBrier, MS, RD, CDES, is an innovator in the field of diabetes, nutrition, and technology. Ashley is a consultant and the Diabetes Education Program Coordinator at the Salinas Valley Medical Clinic’s Diabetes & Endocrine Center.
Ms. LaBrier is passionate about providing person-centered education to empower those who live with diabetes. Having been diagnosed with type 1 diabetes herself nearly 20 years ago, she combines her professional knowledge with personal experience and understanding.
Whether you are new to diabetes or a seasoned expert, you’ll benefit from this virtual conference with the latest research plus critical content that you can immediately apply to your clinical practice.
If you are seeking a state-of-the-art review of current diabetes care, this course is for you. Our team has been fine-tuning this course for over fifteen years, and we know what you need. This program can also be a great addition to your CDCES or BC-ADM exam study plan.
Group discounts are available!*
Download Course Flyer | Download Schedule
All hours earned count toward your CDCES Accreditation Information
Sign up for Diabetes Blog Bytes – we post one daily Blog Byte from Monday to Friday. And of course, Tuesday is our Question of the Week. It’s Informative and FREE! Sign up below!
The use of DES products does not guarantee the successful passage of the CDCES exam. CBDCE does not endorse any preparatory or review materials for the CDCES exam, except for those published by CBDCE.